Dr. John Graham illustrates the benefits of accelerated tooth movement
Three years ago, I relocated to Salt Lake City, Utah, which is a highly competitive orthodontic market with a number of orthodontists as well as general practitioners who practice orthodontics. Looking for ways to clinically differentiate my new practice, I decided to focus on enhancing the patient experience by offering accelerated treatments and diminishing the pain associated with orthodontics. What I found as I researched and experimented with different techniques is that I needed to look beyond just patients’ perspectives and perceived benefits.
[userloggedin]
As orthodontists, we know there are many health issues and financial burdens also associated with keeping patients in treatment longer than necessary. The clinical issues include increased risk of root resorption, decalcification, caries, gingivitis, and periodontal disease. In addition, emotional issues, such as loss of motivation to maintain treatment compliance and increased frustration on both the patients’ and orthodontists’ part, might occur as ultimately orthodontists begin to lose money on cases when treatment is prolonged.

So what can we do to differentiate our practices, grow our businesses, and become more patient-centric in our treatment options? In a nutshell, we need better, shorter, and more comfortable treatment options. In my practices, this translates into doing fewer extractions, using passive self-ligation with the Damon™ System or Insignia™ (Ormco), and accelerating treatment with AcceleDent® (OrthoAccel® Technologies, Inc.).
 According to the recent American Journal of Orthodontics and Dentofacial Orthopedics (AJO-DO) survey, orthodontic treatment on average takes approximately 2 years to complete. However, nearly 70% of the orthodontists who replied to the AJO-DO survey were interested in adopting additional clinical procedures to reduce treatment time, but many were not aware of such procedures. They deemed a 20%-40% reduction in treatment time to be appealing enough to use alternative techniques that accelerate orthodontic tooth movement.
According to the recent American Journal of Orthodontics and Dentofacial Orthopedics (AJO-DO) survey, orthodontic treatment on average takes approximately 2 years to complete. However, nearly 70% of the orthodontists who replied to the AJO-DO survey were interested in adopting additional clinical procedures to reduce treatment time, but many were not aware of such procedures. They deemed a 20%-40% reduction in treatment time to be appealing enough to use alternative techniques that accelerate orthodontic tooth movement.
In my practice, I see 20%-40% reduction in treatment time and many times much greater than that by using AcceleDent and self-ligating orthodontics. Before presenting those case studies, I want to review other accelerating treatment methods that I’ve experimented with over the years to demonstrate exactly why the AJO-DO report states that neither orthodontists nor patients favor invasive approaches to reducing orthodontic treatment time.1
Invasive techniques to accelerate tooth movement
I opted to do Wilckodontics on a patient of mine named Alex. Alex was a swimmer, and he could not breathe through his nose at all because he had a constricted maxilla. Alex did not want to go through any kind of orthognathic surgical procedure and wanted to have treatment completed as quickly as possible. Alex had significant maxillary constriction, and his breathing area was so constrained throughout his posterior upper oropharyngeal airway that he had less than 100 mm2 of area allocated for breathing (Figure 1). During the actual Wilckodontics procedure, a complete mucoperiosteal flap was reflected far into the buccal vestibule. The idea is to damage the bone as much as is reasonable, so vertical osteotomies are made with a reciprocating saw. Not only are vertical osteotomies made through the cortex, but divots were also made with a round bur. The point of this procedure is to elicit the regional acceleratory phenomenon (RAP) that H. M. Frost first identified in his research in 1983.2 RAP stimulates aggressive bone turnover.
The next step in the process is to pack in freeze-dried bone to augment the accelerated bone physiology that occurs while the patient is being treated (Figure 2). Notice that the patient is already in braces. The braces were put on about a week before the procedure. After his third or fourth visit, Alex reported that he could actually breathe. For the first time as a swimmer, he snorted water down his nose and choked on it. It was the first time he ever had communication between his nose and his lungs, and he was elated! While the end result appeased the patient whose Class 3 corrected significantly, I was not happy as an orthodontist because of how long it took, the ultimate final results, and the invasiveness necessary to perform the procedure.

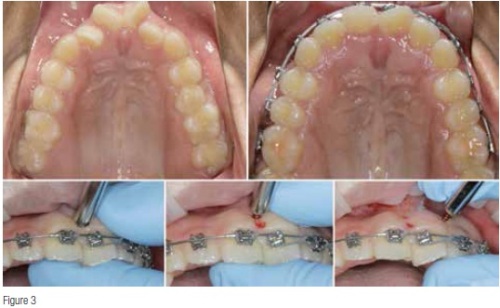
Cortical perforations as a procedure have long been researched, and many orthodontists are familiar with the technique. According to research conducted by Teixeira, et al., in 2010, we know that orthodontic force in concert with cortical perforations produced twice the amount of tooth movement during the same period of time with the same delivery of force in the control. I’ve used this technique as well and have provided an example with a patient whom I bonded in October 2011. The patient had severe anterior rotations, and more than a year later in February 2013, tooth No. 9 still had not rotated. I was frustrated but wasn’t convinced that the tooth was ankylosed. Therefore, I performed multiple cortical perforations along the mesial and distal aspects of the root (Figure 3). One month later, the tooth started to move due to the cortical perforations, but one of the problems orthodontists face with this method is the limited time frame that such a procedure provides. Whether it’s done through cortical perforations, surgery or piezocision, patients only benefit from the procedure for about 6 months, at which time the procedure must be repeated if the accelerated benefits are to be enjoyed over a longer period of time.
To summarize, the disadvantages of using cortical injury to accelerate orthodontic treatment include quick diminishment of RAP after the physiologic peak at 6 weeks, no diminution in the discomfort of orthodontic tooth movement, and no mechanical enhancement to my passive self-ligating treatment. Practically speaking, these issues are the complete converse of the advantages of using AcceleDent.
Passive self-ligation — light biological forces during treatment
I believe in the effective integration of passive self-ligation using Damon and AcceleDent. At least 50% of my practice is comprised of adults, and 80% of those adults are being treated with AcceleDent. I also perform very few extractions — in my last 1,000 cases, my extraction rate was at 0.05%. I realized early on in my orthodontic training that forces conventionally used in orthodontics were far too heavy and actually slowed down tooth movement, which is why I’m much more in favor of light forces or what I call biological forces. It’s very similar movement to what orthopedic surgeons and physicians have employed for years. Pointing to research published in Angle Orthodontist: “All self-ligating designs performed with the efficiency and producibility associated with expectations. Specifically self-ligation out-performed the conventional brackets when coupled with up to 0.020 x 0.020 inch wires.” This article also reported that self-ligating brackets produced lower frictional values, better hygiene, and patient comfort, which is indeed true. Additionally, clinical studies have concluded that orthodontic treatment with self-ligated brackets reduced chair time and shortened treatment. Again, I’ve seen all of this in my practice for over a decade.
My very first Damon case that I did in private practice was with a young girl named Brittany. She was severely crowded in the upper arch and had mild crowding on the lower. When we tried to get Brittany’s smiling photo, we were unable to because she had never smiled before. Brittany’s parents absolutely refused extractions. While I obviously would change a lot about this case today, the photos show the remarkable results that are possible with passive self-ligating brackets. Brittany has great gingival health as there’s no stripping or thinning, and her gingival levels are the exact same as they were when she started treatment. After treatment, she had great Class 1 occlusion on both sides, and her palate and physiological adaptation were remarkable (Figure 4). Two years after treatment, I did another round of CT scans and was very pleased with her stability. She relapsed about a millimeter in the maxillary arch only because she wasn’t wearing her nighttime retainer.

AcceleDent-preferred non-invasive option to accelerate tooth movement
AcceleDent for accelerating orthodontic treatment is supported with much science and clinical evidence (Figure 5). Dr. Clinton Rubin at SUNY Stony Brook demonstrated in a sheep model that pulsatile forces delivered for 20 minutes a day, 30 hertz for a year had robust change in bone physiology compared to the controls. In another double-blind, prospective, placebo-controlled clinical trial, Rubin demonstrated that the healing time of fresh fractures of the radius and tibia was reduced 40%. It has also been demonstrated in the clinical treatment of delayed unions and non-unions.

We know that AcceleDent’s SoftPulse Technology™ works because it’s been used for over 2 decades in orthopedic surgery. AcceleDent employs pulsatile forces at 30 hertz, which is the same frequency used to increase the rate of fracture healing and bone density by cellular signaling. With AcceleDent, I’m increasing the biologic response to pressure, thus moving teeth quicker and assisting the mechanics by the vibratory stimulus helping overcome the already decreased friction in the self-ligating brackets I use. Not to mention, we’re also greatly reducing patient discomfort — again, completely opposite of that which occurs with cortical perforation.
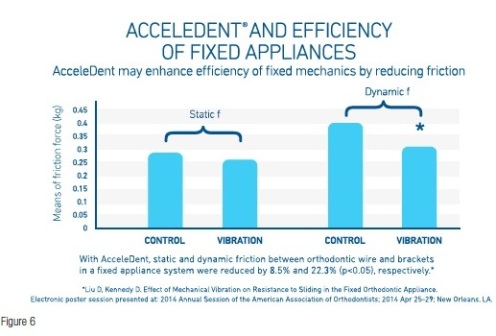
There was a very interesting poster session presented at the American Association of Orthodontists 2014 Annual Session on the topic of “AcceleDent and the Efficiency of Fixed Appliances” (Figure 6). The poster shows that AcceleDent enhances efficiency of fixed mechanics by decreasing friction. It also shows that static and dynamic friction between orthodontic wire and brackets in a fixed appliance system is reduced by 8% and 22.3%, respectively.
AcceleDent case studies
For further demonstration, examine these real patient case studies from my practice.
Allison is 33 years old and was a Class 2, Division 2 case that was bonded January 2014. Like most of my adult patients, she opted to use AcceleDent to accelerate her treatment. Allison’s reset appointment was 4 months later and in 18 x 25 wires. She started in 014 round wires, changed to 018 wire in February. In March, I changed her to a 14 x 25 rectangular copper NiTi wire, and in April, she was changed to an 18 x 25 copper NiTi. She was in light, 2-ounce elastics the entire time. For one visit, she went back down to 14 x 25s, and then in June, she was back to 18 x 25s preparing for the finishing phase in July. After 6 months of treatment, she was in her finishing wires followed by another 6 months of finishing bends. She got her braces off January 2015 and was only in treatment less than 11 months (Figure 7).


Jamie is a 47-year-old AcceleDent patient of mine, and she completed treatment in 11 months. She was bonded in February 2014, changed to 14 round copper NiTi in March, 018 in April and 14 x 25 in May. By June, Jamie was in 18 x 25 copper NiTi, and in July, she went into her upper and lower finishing wires, a 19 x 25 TMA top and a 17 x 25 TMA below. Her finishing appointment was in October, and she got her braces off in January (Figure 8).
In summary, I want to give a few takeaways from my AcceleDent case studies.

While these patients are moving quickly through their treatment, there is no compromise in the finishing.
I see my AcceleDent patients every 4 weeks instead of every 6 or 8 weeks. This also means that reset appointments are pushed back to 4 months instead of the typical 6 to 8 months.
It’s important that you demarcate your AcceleDent patients on their charts because it’s going to affect how you schedule them. In my office, we do that by putting a small toolbox icon near their name.
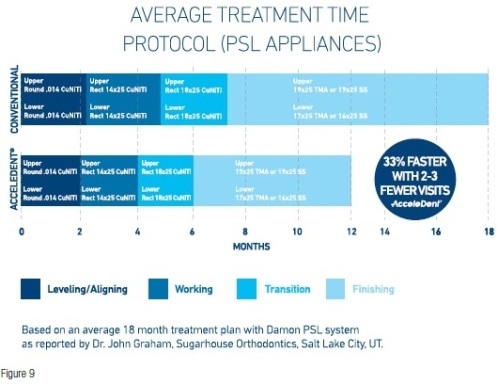
My AcceleDent patients are in the round wire phase for generally 1, sometimes 2 months. Reset appointments are generally at either 4 or 6 months, giving me 6 months of finishing time and allowing me to complete treatment within a year or in less than a year (Figure 9).
You have to educate your patients about AcceleDent. Add the accelerated treatment option information to your website, share patient and staff testimonials via social media, alert patients about accelerated treatment via email, and distribute accelerated treatment marketing materials at events such as bridal expos, community health fairs, and back-to-school programs.
Patients have made it clear that they’re no longer willing to tolerate 2 or more years of orthodontic treatment. We owe it to them to embrace, explore, and utilize technology that will not only enhance their patient experience, but also help us grow and differentiate our practices. I’m not shy to say that AcceleDent has been the single greatest asset in helping me achieve my goal of making sure the patient experience in braces is as brief and comfortable as possible.
References
1. Uribe F, Padala S, Allareddy V, Nanda R. Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time. Am J Orthod Dentofacial Orthop. 2014;145(4 Suppl):S65-73.
2. Frost, HM. The regional acceleratory phenomenon: a review. Henry Ford Hospital Medical Journal. Vol 31, No.1, pp 3-9, 1983.
3. Teixeira CC, Khoo E, Tran J, Chartres I, Liu Y, Thant LM, Khabensky I, Gart LP, Cisneros G, Alikhani M. Cytokine expression and accelerated tooth movement. J Dent Res. 2010;89(10):1135-1141.
4. Sandra P Henao, Robert P Kusy. Frictional evaluations of dental typodont models using four self-ligating designs and a conventional design. Angle Orthod. 2005;75(1):75-85.
[/userloggedin]
[userloggedout][/userloggedout]
Stay Relevant with Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
Read our following terms and conditions before subscribing.
