Dr. Anoop Sondhi illustrates innovative treatment for a teenage patient

 A 16-year-old male patient presented for orthodontic treatment with an atypical Class II Division 2 malocclusion. Although the overall dental and skeletal pattern featured a Class II Division 2 discrepancy, tooth No. 9 demonstrated a significant labial inclination, as opposed to a lingual inclination. Given the patient’s age, it was evident that the Class II correction would prove to be a challenge.
A 16-year-old male patient presented for orthodontic treatment with an atypical Class II Division 2 malocclusion. Although the overall dental and skeletal pattern featured a Class II Division 2 discrepancy, tooth No. 9 demonstrated a significant labial inclination, as opposed to a lingual inclination. Given the patient’s age, it was evident that the Class II correction would prove to be a challenge.
[userloggedin]
The treatment plan, therefore, called for the integration of various systems, including Variable Prescription Appliances, self-ligation, and Class II Correctors.
As seen in the diagnostic records (Figures 1A-1C), the anteroposterior discrepancy was a full-cusp Class II malocclusion. Given the patient’s facial and lip profile, extractions were considered undesirable. It was also quite evident that the correction of the Class II discrepancy would require a fixed Class II corrector. The panoramic radiograph reveals an impacted tooth No. 32. Due to the proximity of the roots to the inferior alveolar canal, the oral surgeon opted to defer extraction of tooth No. 32. The tooth was kept under observation.
The Variable Prescription Orthodontics technique (VPO – 3M) was used for this case. The maxillary arch called for Medium Torque brackets on all the teeth except tooth No. 8, where a High Torque bracket was placed. Because the fixed Class II correctors generally cause some proclination of the mandibular anterior segment, Low Torque brackets were placed in the mandibular arch.
Figure 2 shows the initial placement of the maxillary and mandibular fixed appliances. The case was treated with Clarity™ SL Self-Ligating Brackets (3M Oral Care) on the maxillary arch, and SmartClip™ SL3 Self-Ligating Brackets (3M Oral Care) on the mandibular arch. Resin-reinforced glass ionomer cement was placed on the occlusal surfaces of the maxillary first molars to dis-articulate the patient and to avoid traumatic contact between the maxillary incisal edges and the mandibular incisor brackets.
Once initial alignment of the arches had been obtained (Figure 3), rectangular wires were inserted to begin expression of the maxillary and mandibular torque. As soon as the curve of Spee had been leveled to an acceptable degree, Forsus™ Class II Correctors (3M Oral Care) were engaged to begin the Class II correction (Figure 4).
The Forsus Correctors were activated by the addition of 1 mm spacers at 6-week intervals.

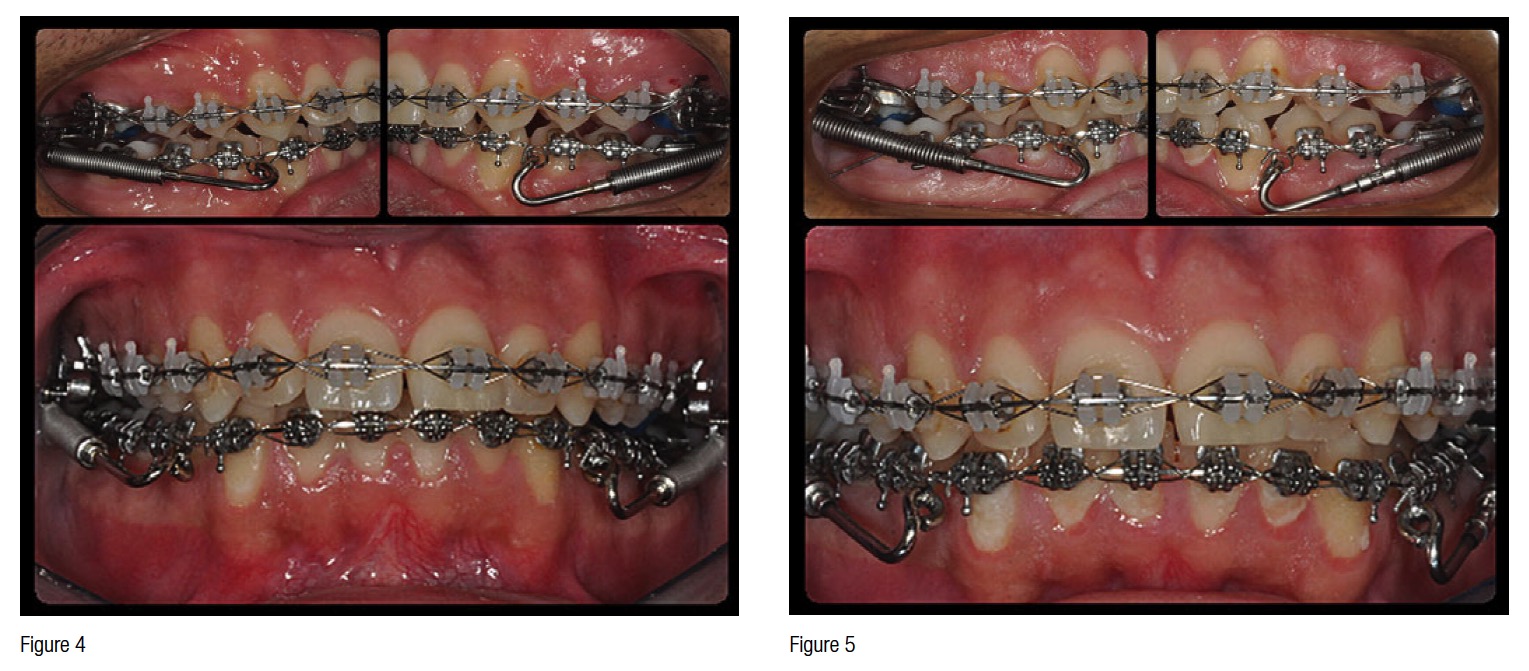
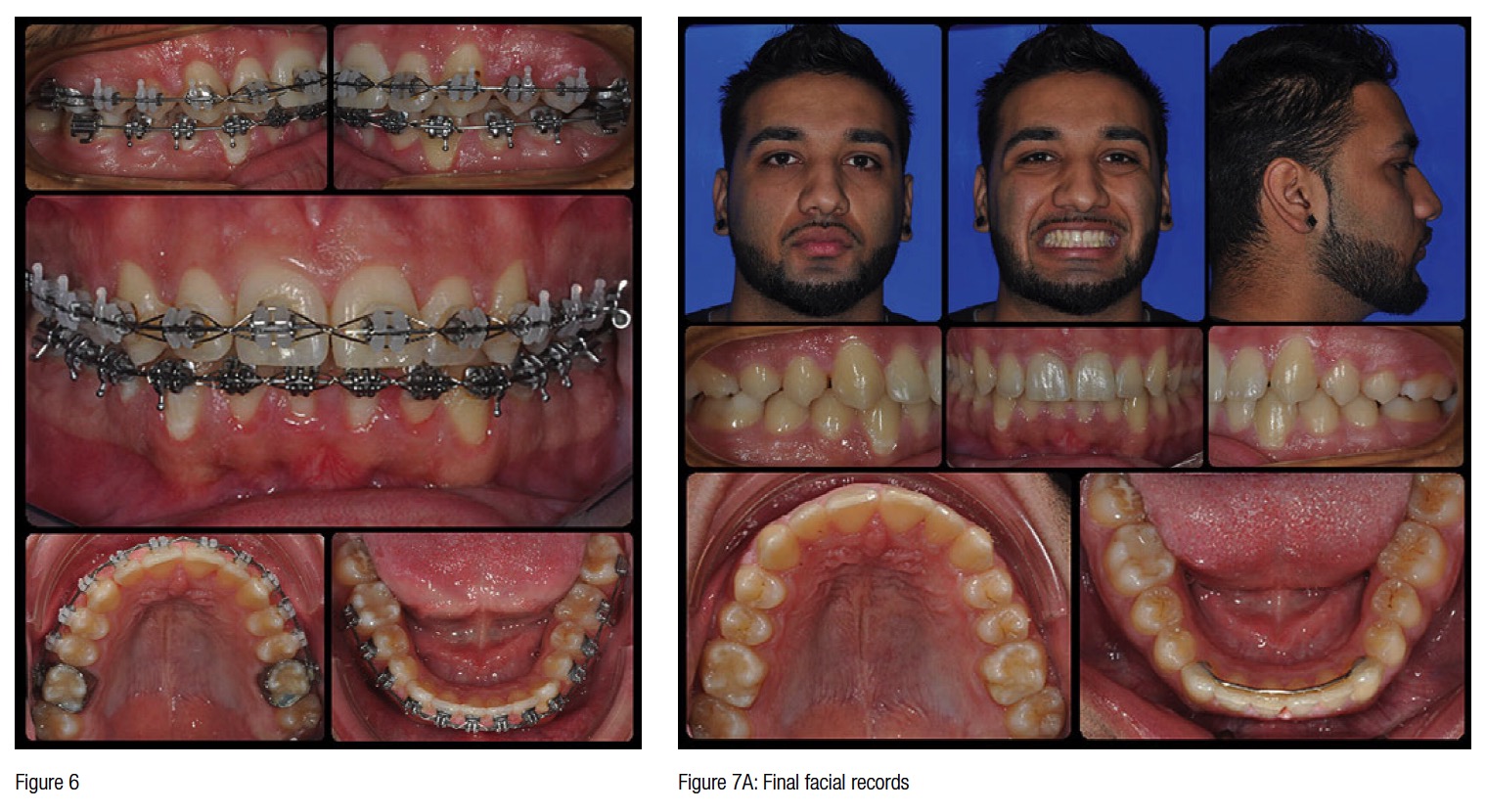
Figure 5 shows the status of the case following completion of the Class II correction with Forsus Correctors. At this time, the finishing archwires were placed, and finishing elastics were engaged to complete the detailing required.

Figure 6 demonstrates the finishing archwires as we approached the completion of treatment, and Figures 7A-7C show the posttreatment records, and the cephalometric and panoramic radiographs.
Because of the efficiency afforded by the use of Variable Prescription brackets, self-ligation, as well as the enhanced efficiency of the Class II correction with Forsus Correctors, the patient’s total treatment time was 16 months. This is quite remarkable, given that we were dealing with a patient who was essentially non-growing. The archwire sequence was as follows:
- 9/19/11 – 2/1/12: Maxillary .012 Nitinol/Mandibular .014 Nitinol
- 2/1/12 – 3/28/12: Maxillary .014/.014 Nitinol Tandem Archwires/Mandibular .014/.014 Nitinol Tandem Archwires
- 3/28/12 – 5/23/12: Maxillary .016 x .025 Beta III Titanium Archwire with enhanced curve of Spee/Mandibular .016 x .025 Beta Titanium w/ exaggerated curve of Spee
- 5/23/12 – 11/29/12: Engagement of the Class II Corrector; inserted .016 x .025 Beta III Titanium archwires
- 11/29/12 – 1/22/13: Class II Corrector removed; inserted .016 x .025 Beta III Titanium archwires
- 1/22/13 – 2/27/13: Placement of a finishing .016 x .025 Beta Titanium wire in the mandibular arch, with finishing elastics
- 2/27/13: Case complete
 Dr. Anoop Sondhi, DDS, MS, received his dental degree from the Indiana University School of Dentistry and his postgraduate certificate and MS in orthodontics from the University of Illinois in 1977. He practices in Indianapolis and is a visiting professor for several graduate programs in orthodontics. He has presented seminars and continuing education courses to several dental and orthodontic organizations all over the world. Dr. Sondhi devotes a significant amount of his work to the development of effective and efficient treatment systems, indirect bonding, interceptive treatment of complex malocclusions, and the orthodontic management of temporomandibular disorders.
Dr. Anoop Sondhi, DDS, MS, received his dental degree from the Indiana University School of Dentistry and his postgraduate certificate and MS in orthodontics from the University of Illinois in 1977. He practices in Indianapolis and is a visiting professor for several graduate programs in orthodontics. He has presented seminars and continuing education courses to several dental and orthodontic organizations all over the world. Dr. Sondhi devotes a significant amount of his work to the development of effective and efficient treatment systems, indirect bonding, interceptive treatment of complex malocclusions, and the orthodontic management of temporomandibular disorders.
Disclosure: In the past, Dr. Sondhi has received honoraria from 3M.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
