Editor’s intro: Drs. Eckhart and Al-Jewair compared MARA-device treated boys and girls to those using mandibular advancers. See their results regarding how much more chin growth can be achieved using the MARA during treatment intervals of a little more than a year during gender-appropriate ages of pubertal mandibular growth.
Drs. James E. Eckhart and Thikriat Al-Jewair study the relationship between incisor movements and horizontal versus vertical expression of the mandibular growth
Abstract
Objectives
To compare the mandibular growth rate of pubertal MARA-treated boys and girls to untreated controls, and to study the relationship between incisor movements and horizontal versus vertical expression of the mandibular growth.
Materials and Methods
This retrospective study evaluated head films approximately 1-year apart from pubertal MARA-treated deep bite Class II boys and girls. Changes in incisor position and Gnathion were measured for vertical and horizontal components and were compared to similar-age boy and girl controls. The movements of the incisor incisal edges were then combined, and that sum was graphed against the ratio of the Gnathion horizontal or vertical movement vector to the Gnathion overall movement vector.
Results
The boy MARA patients grew the mandible 5.7 mm in 14.2 months (a treatment effect increase of 1.7 mm over controls), and the girl MARA patients grew the mandible 3.7 mm in 12.5 months (a treatment effect increase of 1.5 mm over controls). There was a strong linear correlation between the total of incisor movements and the percent Gnathion horizontal or vertical movement in boys (p < 0.05) and girls (p < 0.05).
Conclusion
MARA boys grew the mandible radially 43% more than controls, and the horizontal expression of that growth was 81% more than for controls. MARA girls grew the mandible radially 64% more than controls, and the horizontal expression of that growth was 82% more than for controls. The sum of growth movements of the incisors is related approximately linearly to the percentage horizontal or vertical growth changes
in Gnathion.
Introduction
It is possible to enhance mandibular growth compared to what would have occurred in untreated controls using mandibular advancers, provided that the treatment occurs during puberty and provided that the treatment period would be long enough.1,2,3,4 This study examines how much more chin growth (compared to controls) can be achieved using the MARA during treatment intervals of a little more than a year, separately for boys and girls, during gender-appropriate ages of pubertal mandibular growth. It has been published that the pubertal period for both sexes averages 30 months, during which the unassisted mandibular growth rate averages 59% higher for boys and 34% higher for girls than the pre-puberty average of 2.4-2.1 mm per year.5 A recent study6 found that pubertal boy controls grew the mandible 4.0 mm in 14.2 months (0.27 mm/month), and pubertal girl controls grew the mandible 2.3 mm in 12.5 months (0.18 mm/month).
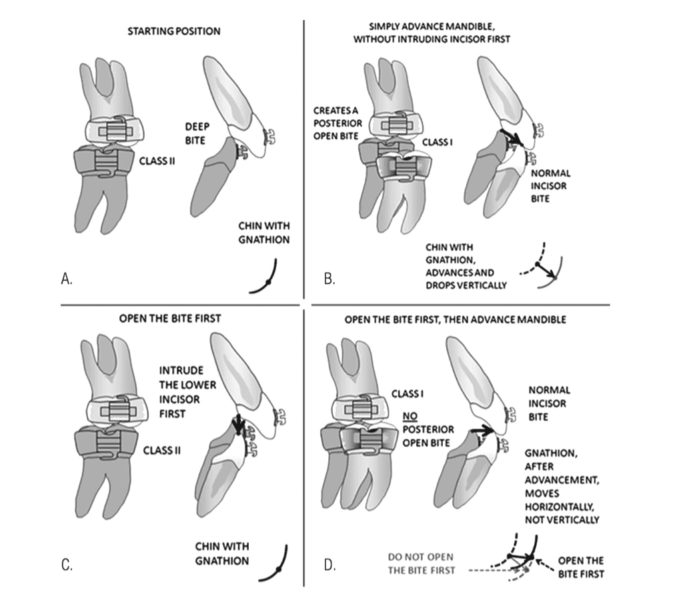
Enhancing the ratio of the mandibular horizontal growth vector to the overall mandibular growth vector is also discussed in this paper. Drawings6 of the mechanics of mandibular growth illustrate that the horizontal and vertical components of Gnathion growth largely relate to how the upper and lower incisors are handled (specifically in deep bites) because extrusion and retraction of the upper incisor — whether by orthodontic movement within the maxilla or by orthopedic movement of the maxilla or both — causes downward vertical rotation and slight backward rotation of the chin, and extrusion and protraction orthodontic movement of the lower incisor promotes downward and slight backward rotation of the growing chin. In the present study, it was determined to open any deep bite with braces and intrusion arches and bite turbos prior to advancing the mandible, allowing the chin to be advanced without requiring it to be dropped vertically due to incisal guidance (Figure 1).
Materials and methods
Two Class II study groups were selected for MARA treatment, one each of pubertal boys and girls. Each group was compared to age-matched Class II controls from Bolton and Michigan.6,7 If the beginning occlusion was a severely deep bite, the MARA was sometimes postponed until after bite opening. If the preliminary bite opening took longer than 6 months, a new T1 film was taken prior to placement of the MARA. The fact that girls start puberty as early as they do sometimes required us to place braces on deciduous teeth while opening the bite. We took a T2 film immediately after removal of the MARA so as to assess accurately the MARA changes. If the T2 film was not taken within 6 months of removal of the MARA, that patient was excluded from this study.
There were three time points chosen for selection of head films. T0 was before any treatment. If the MARA was placed within 6 months of the T0 film, that film was used for the beginning measurements. T1 was after bite-opening braces, if any, before MARA, if the beginning braces took 6 months or longer. T2 was immediately after MARA removal. (This time was chosen deliberately so as not to dilute the growth per month experienced by the MARA patients, which would have seemed to be if we used the T3 film taken after all active treatment was used, since the T2-T3 interval was often another 12 months.)
There were 21 boys with an average beginning age of 13.2 years, and 11 girls with an average age of 11.5 years. The head films were chosen to represent accurately the time the MARA was in place (Table 1).
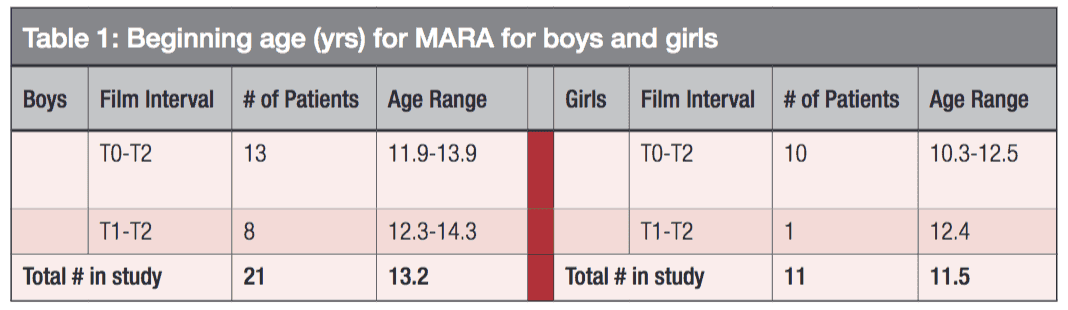
The decision of what age to start the MARA treatment for each study participant was guided by the discussion in Mellion, et al.,5 regarding pubertal chronological age, statural growth, and mandibular growth. The MARA boys started at an average age of 13.2 years, with a range of 11.9-14.3 years, and the MARA girls started at an average age of 11.5 years, with a range of 10.25 years to 12.5 years.
To study the effects of the treatments on incisor positions and chin growth, we made measurements in PowerPoint. (Figure 2). All our films had embedded rulers for standardized enlargements. In both MARA groups, lines were drawn on the T1 film for SN, S-A, S-U1, S-Gn, palatal plane, and functional occlusal plane. Also, the incisal tip of L1 was marked, and three dots circumscribe Sella (Figure 2A). These points were chosen because they are easy midline structures to identify accurately. Although many published studies measured Co-Gn, or Ar-Gn to assess mandibular length, it was found to be easier to see S-Gn when comparing two films. This method had a small error of overlooking fossa growth, which we ignored due to its small magnitude and due to the short T1-T2 intervals. Mandibular radius was approximated to be from Sella to Gnathion for both T1 and T2, because only the change in Gnathion was being examined.

Next, the lines and dots were grouped, copied, and pasted (Figure 2B), and transferred to the T2 film and superimposed on SN at S (Figure 2C). Sometimes the T2 film had to be rotated in PowerPoint so the grouped lines would superimpose correctly on SN, depending on the variation in tip angle of the head between T1 and T2. The T2 A pt, U1, L1, and Gn were then marked and grouped onto the T2 film (Figure 2C).
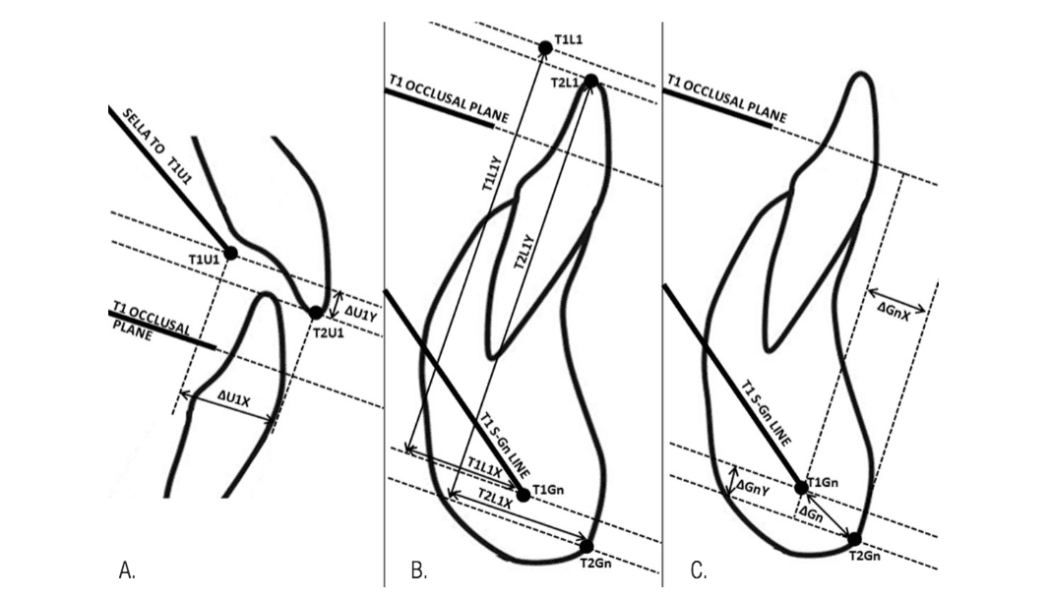
Next, the ΔU1, ΔL1, and ΔGn were measured in their X and Y distances from the T1 U1, L1, and Gn, using the T1 occlusal plane as the reference X axis (Figure 3).
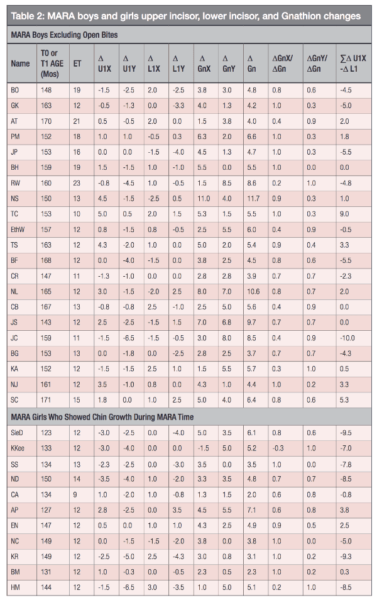
The Δ measurements were made by viewing the films at 200% to increase accuracy, and then correcting the tables to 100% in Excel. The measurements are compiled in Table 2.
Results
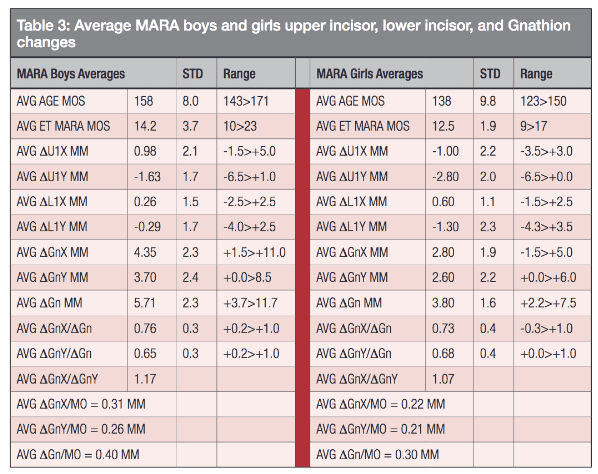
Table 3 shows the average movements of the incisors and Gnathion separately for MARA boys and girls.
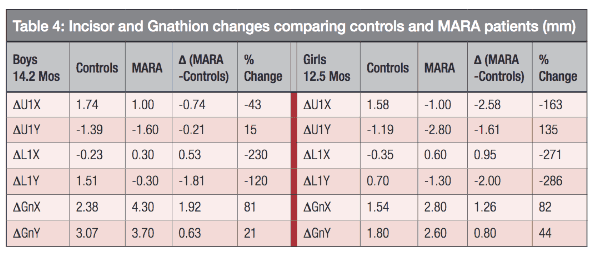
Table 4 shows the comparison of incisor movements and Gnathion movements between MARA and controls for boys
and girls.
The MARA boys moved the upper incisor backward 0.74 mm in 14.2 months compared to controls, a retraction of 43%. The MARA boys moved the lower incisor forward 0.53 mm compared to controls, an increase of 230%. The MARA boys had a small 15% increase in downward movement of the upper incisor, but a large 120% increase in downward movement of the lower incisor, which can be explained by the deliberate bite opening mechanics prior to MARA placement. The MARA boys increased the vertical component of chin growth only 21% compared to controls, but increased the horizontal component of chin growth by 81% compared to controls, nearly a 2 mm increase.
The MARA girls moved the upper incisor backward 2.58 mm in 12.5 months compared to controls, a retraction of 163%. The MARA girls moved the lower incisor forward 0.95 mm compared to controls, an increase of 271%. The MARA girls had a significant 135% increase in downward movement of the upper incisor, and a large 286% increase in downward movement of the lower incisor. The MARA girls increased the vertical component of chin growth only 44% compared to controls, but increased the horizontal component of chin growth by 82% compared to controls, nearly a 1.3 mm increase.
MARA girls had more retraction and extrusion of the upper incisor than boys did. Both boys and girls showed a large increase in Gnathion horizontal growth, and slight increase in Gnathion vertical growth.
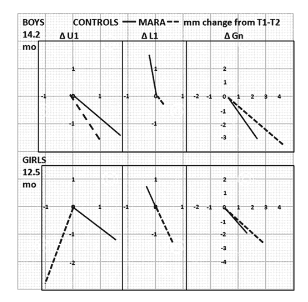
Figure 4 shows that compared to controls, for 21 MARA boys in 14.2 months, the upper incisor moved slightly down and back. The lower incisor moved slightly forward and intruded nearly 2 mm. Gnathion nearly doubled its forward movement, and slightly increased its vertical movement. The mandible increased in length an average of 0.40 mm per month, compared to 0.27 mm per month for controls. This shows an increase in boys’ radial mandibular growth rate with the MARA of 43%. Compared to controls, for 12 MARA girls in 12.5 months, the upper incisor moved down over 1.5 mm and backward 2.5 mm. The lower incisor moved slightly forward and intruded nearly 2 mm. Gnathion significantly increased its forward movement, and slightly increased its vertical movement, and the mandible increased in length an average of 0.30 mm per month, compared to 0.18 mm per month for Controls. This shows an increase in girls’ radial mandibular growth rate with the MARA of 61%.
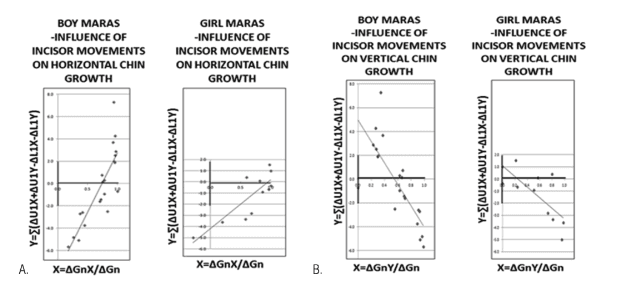
Using the data in Table 2, it is possible to plot a scatter graph showing the relationship between total incisor movements and percentage of horizontal chin change (Figure 5).
Statistics
For control and MARA boys and girls, the sum of the upper incisor X and Y movements, minus the sum of the lower incisor X and Y movements, was related linearly to the proportion of chin growth that was horizontal and to the proportion of chin growth that was vertical. For control boys, the Pearson correlation coefficient was r = 0.8262, and the probability factor was p = < 0.00001. The result is significant at p < 0.05. For control girls, the Pearson correlation coefficient was r = 0.8081, and the probability factor was p = 0.000267. The result is significant at p < 0.05. For MARA boys, the Pearson correlation coefficient was r = 0.8297, and the probability factor was p = < 0.00001. The result is significant at p < 0.05. For MARA girls, the Pearson correlation coefficient was r = 0.83092, and the probability factor was p = 0.00059. The result is significant at p < 0.05.
Discussion
Both control boys and girls and MARA boys and girls showed a significant relationship between incisor vector changes and horizontal and vertical chin change. There is no doubt that the direction of chin growth is influenced by how the incisors are handled.
It should be repeated that this study uses T2 films that were taken shortly after removal of the MARA prior to final braces removal, and this fact may distinguish this study from other published reports. As a safeguard to prevent artificial anterior displacement of the mandible, tomograms were taken prior to MARA removal to assure that the condyles were centered in the fossa.
This study does not mix boys and girls.
If data becomes available regarding the chin growth vector amounts and ratios for intermaxillary push-pull Class II correctors, it may prove that the use of the MARA produces superior chin changes, albeit small, compared to those devices that are suspected of increasing the vertical vector of chin growth, particularly any which extrude the lower molars.
It appears that the MARA minimally advances the lower dentition compared to controls, which may not be true of other intermaxillary Class II correctors.
Larger MARA horizontal chin changes might be attempted by deliberately retracting lower incisors, such as by removing lower bicuspids, and leaving the MARA in during a longer portion of puberty, creating a Class III molar relation in order to double the horizontal chin increase. Especially for boys, the MARA increase in monthly growth rate of the mandible over controls might be even greater if the advancement of the mandible is greater, and the total mandibular growth might more than double if the MARA is left in twice as long.
By carefully selecting the optimum treatment age, recognizing that girls need to start 2 years earlier than boys, and by controlling the effect of incisor position on hinging of the growing mandible, it can be shown that chin prominence can be enhanced.
A similar study might be done with other Class II corrector cases to see how they affect chin radial growth and the ratio between chin horizontal growth and chin radial growth.
Conclusions
Movements of the upper and lower incisors are related to horizontal and vertical chin change in both control and MARA deep-bite boys and girls.
There was a 43% increase in overall growth of the mandible comparing MARA boys to control boys, and a 61% increase in overall growth of the mandible comparing MARA girls to control girls.
There was a 81% increase in horizontal chin growth comparing MARA boys to control boys and a 82% increase in horizontal chin growth comparing MARA girls to control girls (probably at least partly due to managing incisor movements).
There was a 1.9 mm increase in horizontal chin change comparing MARA boys to control boys and a 1.3 mm increase in horizontal chin change comparing MARA girls to control girls.
The MARA did not move the boys’ or girls’ lower dentition much forward compared to controls (less than 1.0 mm forward).
The MARA barely changed the vertical component of chin growth compared to controls (21% increase for boys; 44% increase for girls).
For non-deep-bite cases, braces are compatible with the MARA but not necessary. Some of these MARA boys were treated with Invisalign after the MARA.
Interested in the MARA device? Read more insights from Drs. Eckhart and Al-Jewair about pubertal mandibular growth in their article, “Magnitude of monthly pubertal mandibular growth in untreated Class II teens, and the relationship between upper and lower incisor movements and horizontal versus vertical expression of chin growth.”
- Freeman DC, McNamara JA Jr, Baccetti T, Franchi L, Fränkel C Long-term treatment effects of the FR-2 appliance of Fränkel. Am J Orthod Dentofacial Orthop. 2009;135(5):570.
- Rabie AR, She TT, Hägg U. Functional appliance therapy accelerates and enhances condylar growth. Am J Orthod Dentofacial Orthop. 2003;123(1):40-48.
- Malta LA, Baccetti T, Franchi L, Faltin K Jr, McNamara JA. Long-term dentoskeletal effects induced by bionator therapy. Angle Orthod. 2010;80(1):10-17.
- Franchi L, Pavoni C, Faltin K Jr, McNamara JA, Cozza P. Long-term skeletal and dental effects and treatment timing for functional appliances in class II malocclusion. Angle Orthod. 2013;83(2):334-340.
- Mellion ZJ, Behrents RE, Johnston LE Jr. The pattern of facial skeletal growth and its relationship to various common indexes of maturation. Am J Orthod Dentofacial Orthop. 2013;143(6):845-854.
- Eckhart JE, Al-Jewair T, Magnitude of monthly pubertal mandibular growth in untreated Class II teens, and the relationship between upper and lower incisor movements and horizontal versus vertical expression of chin growth, Orthodontic Practice US, Jan-Feb 2019, 10:1, (16-26)
- AAOF Legacy Collection, https://www.aaoflegacycollection.org/aaof_home.html
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
