CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This self-instructional course for dentists aims to show the benefits of two digital tooth-moving technologies — Invisalign® and LightForce® — for patients with different compliance levels.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify characteristics of Invisalign technology.
- Identify characteristics of LightForce technology.
- Realize some shortcomings of traditional, non-digital treatment planning.
- Observe the case of a previously noncompliant patient who needed braces.
- Observe the case of a previously treated patient who was compliant and received clear aligners.

Dr. David Alpan shares his expertise with two digital tooth-moving technologies
Abstract
I thought it would be interesting to do a retrospective comparison6 of two different digital-based treatment outcomes with patients who presented with similar mal-occlusions, treatment time, age, and a desire for similar outcomes. This article will focus on two digital-based treatment systems while looking at two different patients — one treated with Invisalign® and the other treated with LightForce® braces. Both patients were given vibration devices to accelerate treatment and reduce discomfort. Digital-based treatments start with an initial digital 3D scan. We use the iTero® system by Invisalign/Cadent to capture our images. Invisalign and LightForce systems require a digital submission; although Invisalign will still accept PVS impressions, it is not recommended. LightForce will only accept digital scans based on numerous studies. Showing an initial 3D intraoral scan is more precise then PVS systems, especially because the PVS impressions have to be scanned. This extra step introduces more errors than a direct intraoral scan. We also prescribe i-CAT 3D X-rays to view ceph, pano, airway, and TMJ images. The initial submission process is very similar, but the compliance required to achieve the desired outcome is dramatically different. Each system offers its benefits to patients, and the results can be almost identical, but the underlying difference between a clear removable aligner and fixed braces is assessing the patient’s compliance level. Great compliance will always lead to better treatment outcomes, but what if the patient is not compliant? I will show that we can we still achieve excellent results with a digital-based fixed bracket system in a less or noncompliant patient.
Introduction
Invisalign is a series of removable clear aligners completely customized to each patient’s specific needs. Yet aligner therapy requires compliance to achieve the desired tooth movements in a reliable way.5 Attachments are utilized with aligners to improve the control and reliability of the outcomes. Attachments function by increasing the surface area and creating a lever, so the plastic can apply the force required to move the teeth very much like a bracket. Adjuncts are utilized in conjunction with aligners to achieve many of the more difficult desired results that aligners alone are not able to accomplish. There are many systems to create adjuncts to overcome the limitations of aligners and, in combination, can treat any malocclusion. I routinely use aligners with TADs and vibration to treat orthognathic surgical patients in 18 months, reducing overall treatment by 6 to 12 months in comparison to a worldwide average of 22 to 26 months.2,3,4
LightForce Orthodontics creates a fixed bracket system that is completely customized based on the desired movements, so torque, tip, and angulations are programmed into the bracket for full control in three dimensions of space. The 3D-printed base on the bracket eliminates the need for custom wires. It is truly a straight-wire technique with the goal to completely remove the need to bend wires. I personally don’t mind bending wire, but the patients and my team have expressed issues about that part of the process. Detailing wires takes up doctor chair time, and the patients usually have more sensitivity at this stage of treatment.
The introduction of prescription brackets and nickel-titanium wires were some of the first techniques introduced to reduce wire bending; then as composite material improved, repositioning brackets became another way to reduce wire bending. With a fully custom bracket, the fundamental goal is to eliminate the wire bending and reduce overall treatment time. Efficiency is always our goal in orthodontics, and eliminating repositioning of brackets and bending wires will reduce treatment time in every fixed bracket case. I still find myself doing detail bends as my ability to get the 3D image just as I would in the mouth is still not as detailed as I prefer.
Both systems are founded on a platform that begins with the end in mind with a final 3D tooth setup of all the teeth, including the bite. The 3D interface can display the before and after with the contact points visible or the amount of IPR needed. Digital-based treatment planning is far superior to the traditional “wait-and-see” to adjust systems. With traditional systems, the clinician needs to be prepared to make necessary multiple decisions mid-treatment. I was trained with edgewise brackets with a straight wire philosophy and have moved away from traditional bracket systems as I moved into the digital world.
Clinically, placing brackets with indirect bonding has proven to be more accurate than just using my eyes. Using a custom fabricated tray or jig system can insure a higher level of accuracy and precision in my treatment and if utilized properly can save overall treatment time and visits to the office. There are some limitations on devising final treatment planning details clinically compared to using 3D digital models. It is difficult to see as much or as well as you can on a model compared to clinically where there is a tongue, cheeks, and a personality to help determine the plan. The efficiency of incorporating digital treatment planning to orthognathic surgical cases has proven to reduce treatment time by 6-12 months.1 Coordination of arches prior to surgery is much easier and effective with digital treatment planning then traditional orthodontic bracket systems.
We do not submit 3D X-rays to either Invisalign or LightForce at this time, but we hope to integrate this data in the future. During 3D digital planning, I presume we will be able to verify root position, morphology, torque, tip and angulations, prognosis of roots, and other valuable information. My experience has been that with more data, we can hope to plan for specific force vectors with these custom appliances to achieve more ideal finishes with fewer case refinements and/or details to our finishing archwires.
I chose two patients with similar diagnosis and treatment plans. Both of my patients presented in their late 20s with a desire to widen and improve their smiles. We scanned both patients with iTero and submitted the digital images as well as a standard set of photos, ceph, and pano with the prescription form submitted online. The 3D setup was created from my prescription, and refined through modifications until I was happy with the final set up (Figure 25). The digital interface gives me the ability to analyze the final outcome prior to ever treating the patient. I am also able to create more than one treatment outcome and evaluate multiple treatment options without ever touching the patient. As an example, I can set up an extraction versus non-extraction set up, or a single mandibular incisor extraction setup to see how much IPR will be needed in the maxillary arch. All my treatment planning can be verified with the 3D digital setup.
Both Invisalign and LightForce provide a 3D digital rendition of the final outcome that can be manipulated by the clinician until satisfaction with the final result is achieved (Figures 11 and 25). Once I accept the digital setup (Figures 11 and 25), I receive my appliances 4 to 5 weeks after submission. I follow the series of aligners just as I would if I were changing archwires. The big difference with my digital planning is I am not doing a mid-treatment progress pano to evaluate the roots and planning to reposition brackets. All my planning is done in the digital stage, so I am not left to guessing during treatment. The only time I am not able to do this is when a tooth is impacted or blocked out, and I have to rescan after the tooth is accessible.
Patient No. 1 — CC
Patient No. 1, CC, had attempted to use Invisalign twice prior, once with a dentist and once with an orthodontist. Both times she didn’t progress past the first few aligners. She had excuses for why the aligners did not work, but after discussing her compliance, there was no question removable aligners would never achieve the treatment goals based on her lack of compliance. I indicated I would not treat her with Invisalign and explained that LightForce braces would achieve her goals in 6 to 12 months. She was not happy about wearing braces as a young, attractive woman in her mid-20s, but agreed based on her lack of success due to noncompliance with removable aligners. Our experience with LightForce was that the custom bases of the brackets fit the contour of the tooth so well that we had no broken brackets due to increased bond strength of a 3D-printed custom bracket base. No broken brackets helped reduce treatment time and improve the experience for the patient (Figures 1-10). When the bracket duplicates the morphology of the tooth, there is less reliance on the adhesive and, therefore, a stronger bond.












Patient No. 2 — HA
Patient No. 2, HA, had been treated with braces as a teenager but stopped wearing her retainers and noticed relapse in her early 20s. Her goal to widen her smile was related to her profession as an actress. She wanted to achieve the result without interfering with her career. I offered her Invisalign treatment that would take 6 to 12 months, explained the compliance needed, and she agreed. If she was not compliant with her aligners, I would have transferred her to braces. I have patients sign a compliance agreement that acknowledges that if they fail with aligners, we will succeed with braces. With a high level of motivation and a persistent desire to be compliant, she achieved her result without the use of braces or any adjuncts (Figures 13-24). After the completion of her treatment, we highly recommended a fixed retainer. Based on her past history with her retainer, we wanted some more “insurance” against relapse — that she would not need retreatment a third time.













Results
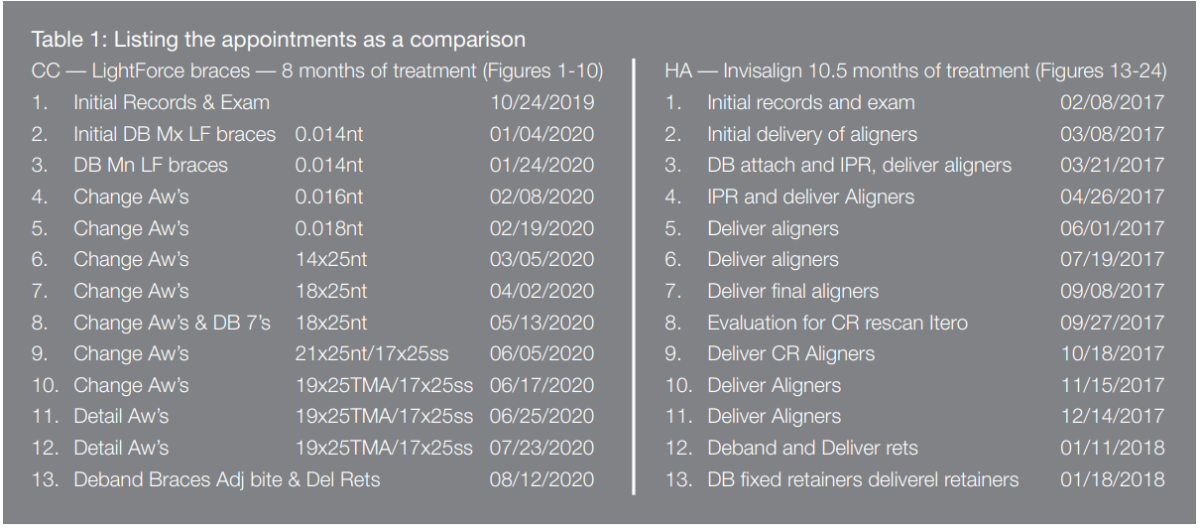
Both patients ended up with a nice broad smile, aligned midlines, resolution of crowding, spacing, rotations of teeth, improved overbite and overjet in a similar number of visits to the office with two different digital-based orthodontic treatments. LightForce completed the treatment in 8 months, and Invisalign in 10.5 months. I don’t think the results are dramatically different, but the LightForce treatment created more arch expansion than Invisalign in less treatment time. There are many similarities in the treatment sequence, as you can see in the figures and in the appointment comparison chart below (Table 1). The exact tooth movement is in the Rx data charts (Figure 26).

Conclusion
Invisalign and LightForce braces treatments created resolution of crowding, rotations, spaces, increased arch width, aligned midlines, and improved overbite and overjet. Both patients were completed in less than 1 year with the use of digital treatment planning and acceleration (vibration). After careful inspection, fixed appliances were able to achieve more arch expansion then clear aligners in a similar treatment time (Figures 9 and 10 versus Figures 20 and 21). I don’t think Invisalign or LightForce is better than the other, but I think one is more suited for the noncompliant patient and the other is not. When a patient asks me which digital-based treatment appliance is better, I inform them one is for compliant, disciplined, organized, and responsible patients, and the other is for noncompliant patients. I can achieve the same results with both digital-based systems in less time and with less sensitivity then traditional non-digital brackets systems. Adding digital treatment planning with acceleration has reduced overall treatment time and number of visits to the office and has lead to more efficiency and overall increased capacity. I choose the digital treatment plan based on the patient’s compliance level and the desire to have treatment be as clear and unnoticeable as possible.
Dr. Alpan has written about digital orthodontic technologies and accelerated orthodontics techniques that he uses in his practice. Read his article, “Combining accelerated orthodontics with orthognathic surgery to reduce overall treatment time” here: https://orthopracticeus.com/ce-articles/combining-accelerated-orthodontics-with-orthognathic-surgery-to-reduce-overall-treatment-time/
Author Info
 David Alpan, DDS, MSD, earned his dental degree in 1996 and completed his orthodontic specialty certificate from University of the Pacific Arthur Dugoni School of Dentistry in 1998. He was awarded a MSD after writing his Master’s thesis on the results of a TMJ research project. Dr. Alpan currently treats patients out of four private practice locations: Los Angeles, Century City, Woodland Hills, and Hawthorne, California. He has lectured for Invisalign® from 1992-1998 at over 250 locations to over 10,000 doctors. He played an integral part of implementing the Invisalign system into the Dental School curriculum. Alpan was an Ormco™ insider and helped 3M™ as a research panelist for many years. Alpan is a key opinion leader for AcceleDent and Propel and has published several articles on accelerated orthodontics. As a Center of Excellence member for Incognito™ and a high-volume Insignia™ provider, he has incorporated several digital-based systems with custom brackets and wires into his digital workflow. Dr. Alpan is currently treating all his patients with Invisalign or LightForce® digital-based systems with airway and TMJ in mind. He is an active member of ADA, CDA, LADS, PCSO, AAO, CAO, AO, OKU, and TKO. His hobbies are racing cars, as a member of Pirelli cup NASA, POC, PCA, CSM, and BMW CCA. He is also a competitive shooter with NSSA, USPSA, UPL, and IDPA, and spends his free time with his family.
David Alpan, DDS, MSD, earned his dental degree in 1996 and completed his orthodontic specialty certificate from University of the Pacific Arthur Dugoni School of Dentistry in 1998. He was awarded a MSD after writing his Master’s thesis on the results of a TMJ research project. Dr. Alpan currently treats patients out of four private practice locations: Los Angeles, Century City, Woodland Hills, and Hawthorne, California. He has lectured for Invisalign® from 1992-1998 at over 250 locations to over 10,000 doctors. He played an integral part of implementing the Invisalign system into the Dental School curriculum. Alpan was an Ormco™ insider and helped 3M™ as a research panelist for many years. Alpan is a key opinion leader for AcceleDent and Propel and has published several articles on accelerated orthodontics. As a Center of Excellence member for Incognito™ and a high-volume Insignia™ provider, he has incorporated several digital-based systems with custom brackets and wires into his digital workflow. Dr. Alpan is currently treating all his patients with Invisalign or LightForce® digital-based systems with airway and TMJ in mind. He is an active member of ADA, CDA, LADS, PCSO, AAO, CAO, AO, OKU, and TKO. His hobbies are racing cars, as a member of Pirelli cup NASA, POC, PCA, CSM, and BMW CCA. He is also a competitive shooter with NSSA, USPSA, UPL, and IDPA, and spends his free time with his family.
Disclosure: Dr. Alpan did not receive financial compensation for any of the products mentioned in this article, but he is a key opinion leader for LightForce®.
References
- Paunonen J, Helminem M, Peltomaki T. Duration of Orthognathic-Surgical Treatment. Acta Odontol Scand. 2017;75(5):372-375.
- Luther F, Morris DO, Karnezi K. Orthodontic treatment following orthognathic surgery: how long does it take and why? A retrospective study. J Oral Maxillofac Surg. 2007;65(10):1969-1976.
- Dowling PA, Espeland L, Krogstad O, Stenvik A, Kelly A. Duration of orthodontic treatment involving orthognathic surgery. Int J Adult Orthod Orthognath Surg. 1999;14(2):146-52.
- Slavnic S, Marcusson A. Duration of orthodontic treatment in conjunction with orthognathic surgery. Swed Dent J. 2010;34(3):159-66.
- Rossini G, Parrini S, Castroflorio T, Andrea Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod.2015:85(5):881-889.
- Alpan D. A review of accelerated orthodontics. Orthodontic Practice US.2017;7(5)28-32.
