Dr. Ron Roncone explains the PhysioDynamic System (PDS)
As orthodontists, we are very aware of the incredible changes that have occurred in the profession. Yet even though these changes have occurred, many issues are still debated.
Case (extraction) versus Angle (non-extraction); Wuerpel could not draw the “ideal” face as Angle had requested. It is too subjective. Stallard’s view of joint position and occlusion versus multiple areas; the Steiner analysis, based on one case, still used today has been joined by over 100 other analyses; non-tipped, non-torqued, and non-angulated brackets versus multiple types of pre-adjusted appliances; non self-ligating versus self-ligating brackets; active versus passive, and so on.
The author’s orthodontic odyssey has included treatment of more than 32,000 patients with many very successful results but also many failures. The old days seemed so simple — a lot of work for the orthodontist — but simple. All of the advancements that we enjoy today have made orthodontics more complicated — easier for the orthodontist — but complicated. For more than 30 years, my quest has been to simplify functional orthodontic treatment while giving the patients what they most wanted — esthetic treatment accomplished in a timely manner.
At times efficiency and esthetics are at odds. At times, esthetics and overhead are at odds. Difficult choices have to be made between superb esthetics and profitability.
The epitome of esthetic orthodontics is obviously lingual treatment. Lingual orthodontics proved to be very difficult. Indirect, custom bases, high lab fees, size of brackets, placement of archwires, and difficulty in finishing were only some of the problems. Lingual has become much easier than in previous years because the brackets are smaller; they can be self-ligating, and wires can be pre-formed. Our European and Asian colleagues have worked diligently over the last 30 years to obtain more accurate bracket placement.
Aligners also offer a high degree of esthetic treatment but can be very expensive to the practice and the ultimate bottom line. My decision is to offer lingual and aligners where appropriate but to add at a minimum at least 1.5 times the lab fee to the typical patient fee for the cost of a labial fee.
So what has this 40-year journey taught me that I can offer to patients? How do we simplify the vast majority of orthodontics?
The SEA Principle is basic to our orthodontic practice. We need to use three areas available to us.
The first is Science. What is in the literature that is practical and proven? What has been shown in the laboratory that can be applied to human anatomy and physiology? The second area we have available to us is our Experience. What have we observed hundreds or thousands of times in our treatment of patients? It is the author’s opinion that the vast majority of emphasis should be placed in this area. The last area of this SEA Principle is Artistry. How do we give the patient the very best artistic finish? This obviously would include the very best facial, smile, and tooth esthetics genetically possible.
If science is the foundation of what we do for our patients, then it stands to reason that what we do must be based on physiology, anatomy, and function. What can we do to allow muscles, bone, teeth, and periodontal complex to be in harmony and equilibrium? It is certainly not in attempting to force the above factors to function where we would like them to function! Our job is to remove impediments to proper muscle, bone, tooth, and periodontal development and function. Mechanics does not trump physiology. We should be attempting to achieve a physiologic orthodontic result.
This thought has led to the development of the PhysioDynamic System (PDS). This system is based on reducing the complexities surrounding treatment of each patient to relatively simple parts. There are six interdependent areas that must be followed sequentially. This certainly is not to say that this is the only way to practice orthodontics. Superb orthodontics is being performed all over the world using many different techniques. However, if you could see 90% of your patients in 6-8 total appointments; if this 90% only needed 2-3 wires in each arch; if you could eliminate the vast majority of errors, emergencies, re-dos, and unnecessary appointments; if you could finish this 90% of your patients in 13-16 months with a functional finish; would that be interesting to you?
The PhysioDynamic System (PDS) — This system of orthodontic practice has at its core, “Simplifying the Complex.”
PhysioDynamics is…
More patient-centric:
- Shorter appointment visits and frequencies — 6-8 total visits for 90% of patients.
- Significantly less discomfort for patients. Internal studies show a discomfort level which averages 4 on a scale of 1-10. This is a subjective scale asked of thousands of patients between 1988 and 2013.
- Reduced treatment times — 13-16 months for 90% of patients.
- Esthetic treatment and results, utilizing the PhysioDynamic QuicKlear® and BioQuick® LP SL brackets (Forestadent USA, Inc.), and the Roncone PDS Prescription, developed for both functional and esthetic tooth position.
Focused on integrated physiological finishes:
- Relaxed musculature
- A natural joint position
- Superb functional occlusions
Centered on the proper use of friction:
- Interactive slot-to-wire relationships using PhysioDynamic interactive QuicKlear and BioQuick LP bracket.
- Proper wire metallurgies lead to more optimum force levels.
- The importance of the correct wire diameters being used in the specific stages of treatment. Larger round wires not smaller at the start of treatment and are kept in place for a minimum of 6 months.
- Simplified wire sequencing.
- Coordinated archforms achieving more functional treatment results.
The Roncone PhysioDynamic Quick System:
- Encompasses a prescription for each tooth designed for both functional and esthetic placement.
- Eliminates the need for anchorage devices such as TPAs, TADs, headgear, etc. in all but a few cases.
- Allows for physiologic control of periodontial fibers allowing them to stay physiologically “flexed” and not over taxed.
- Greatly enhances control of the vertical dimension.
- Addresses all 28 reasons for relapse.
Specific Adjuncts as Integral to the PDS:
- Correct use of anterior turbos.
- Correct anatomical and functional archforms.
- PDS titanium springs with precise forces.
- Utilizing Beta looped wire to achieve ideal vertical control as well as A-P.
- Absolute, precise placement of brackets on teeth.
- Virtual elimination of emergencies and SOS visits (under 1% of all patient visits)
The esthetic finish is centered on:
- Tooth position — horizontally, vertically, and axially
- Smile line
- Individual tooth esthetics
- Full arch natural smiles
- Functional occlusion
The Six Steps of the Physio-Dynamic System (PDS) are:
- Achieving full muscle relaxation of head, neck, and face. This is absolutely essential. It is not in any way related to the use of pulse machines or electromyography. It is relatively simple to achieve.
- Superb diagnosis using a checklist method and attention to the “Diagnostic Dozen.”
- The PDS Prescription using self-ligating brackets for maximum efficiency only.
- Precise bracket placement with JSOP® jigs.
- Three distinct stages of treatment. Knowing when you are finished greatly reduces relapse.
- Post-removal finishing for function and esthetics.
PhysioDynamic System (PDS) Wires
Let’s discuss a few key elements of the PDS; the wires and the three stages of treatment. There has been much discussion about size and force of wires. Which wires move teeth faster? Do smaller diameter wires work better?
With rare exception, all wires used in the Roncone PhysioDynamic System are Titanium Alloy Wires. The combination of larger diameter, specific force level PDS Wires (thermal and super elastic) in Stage 1, along with larger heat activated rectangular “quality
control” wires (for Stage 2) and finally PDS Beta Titanium finishing wires for Stage 3 — combined with the active clip — produces superb results and rapid tooth movement. In order to correct rotations, obtain proper archform, and correct the Curve of Spee, a single large
diameter or two smaller diameter wires in the slot at the same time are used for a minimum of 6 months.
Contrary to what has become popular in recent years, the use of small diameter wires does not move teeth more quickly or with improved directional forces. The role of reducing friction and its relationship to more rapid tooth movement has not been proven. In fact,
Experience has shown the opposite.
Larger diameter wires such as a .018 H.A. wire or twin .014 SE wires are, in the author’s opinion, much more effective in correcting rotations, obtaining correct archform, and leveling the Curve of Spee. The twin wires have been used in my practice for 40 years. An article published by Dr. Jim Ackerman, a superb orthodontist, teacher, and researcher in the early 1970s highlighted the use of two .012 stainless steel arches in a .022 slot. This concept has been mainstay in our practice. In 1988, stainless steel wires were replaced with twin Niti wires. Since that time, appointment intervals were dramatically increased.
Wires — Stage 1 (6 months)
For mild to moderate tooth displacement, a PDS Thermal .018 wire is used.
For moderate to severe tooth displacement, two (2) PDS superelastic SE .014 wires are placed in the slot simultaneously. These create a much more optimally directed force level. The large diameter wire or two small diameter wires in the slot at the same time are critical to quickly moving teeth.
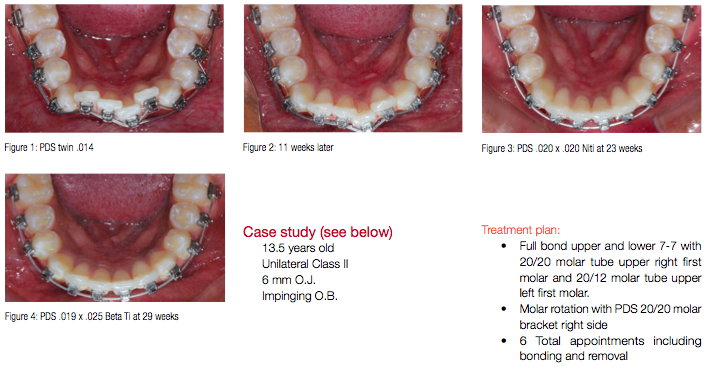
The wires are placed, checked in 12-14 weeks, and the patient is not seen again for another 12 weeks. Only then is a rectangular second stage wire placed. Figures 1-4 show progression of tooth movement over approximately 6 months. On many occasions, tooth alignment occurs within 8-10 weeks. The wires should still be kept in place for 6 months to correct the Curve of Spee and to achieve proper archform.
A huge additional advantage of a large diameter single wire or twin smaller wires is the root parallelism which occurs during the initial 6 months of treatment.
Wires — Stage 2 (6-10 weeks)
After achieving Stage 1 goals with round titanium wires which are kept in place for 6 months, an .020 x .020 heat-activated wire is placed. The purpose of this wire is one of quality control. This wire will almost fill the slot in the vertical. This allows the orthodontist to check bracket placement. Incisal edges and marginal ridges should be perfect. This wire is left in place for 6 weeks. If bracket placement was proper, the .020 x .020 HA wire is removed, and Stage 3 wires are placed. If tooth position is not ideal, then appropriate brackets are changed, the same wire is replaced for 4 weeks, and then, Stage 3 begins (Figure 3).
Wires — Stage 3 (4-6 months)
The final wires are .019 x .025 Beta titanium. The flex in these wires versus stainless steel allows the teeth to fit more easily. The upper arch has a “P” or Snoopy loop distal to the lateral incisors. If adjustments are needed for torque or anterior guidance, they can easily be done intraorally. Figure 4 shows the lower arch with an .019 x .025 Beta PDS wire. If necessary, elastics can be worn during this stage.
Case study (see below)
13.5 years old
Unilateral Class II
6 mm O.J.
Impinging O.B.
Treatment plan:
- Full bond upper and lower 7-7 with 20/20 molar tube upper right first molar and 20/12 molar tube upper left first molar.
- Molar rotation with PDS 20/20 molar bracket right side
- 6 Total appointments including bonding and removal


Last, let’s discuss one of the Auxiliaries of the PD System:
Anterior bite turbos
Why are they important? There are several important reasons for their use:
- When lower posterior are bonded, bite forces do not cause loose brackets.
- To disclude (separate) posterior teeth. This allows:
- Lower posterior teeth to erupt very easily to correct the COS where appropriate.
- If posterior teeth occlude during treatment, muscular forces will always depress teeth into the apical area of the root. Even if full-size stainless steel wires are used, muscular forces will “win.” The turbos will allow these voids at the apices of teeth to fill in with bone. The turbos are kept in place for many months (9-12). This eliminates relapse of overbites.
- Eliminates the significant occlusal forces that occur during tooth contact. (The average person swallows between 1,700-2,400 times per day.)
- The elimination of posterior tooth contact during treatment suppresses the neuromuscular proprioception which causes people to “bite” where the teeth currently fit.
- Because most teeth are not in contact, teeth move more quickly.
- In moving from Class II to Class I, wear of teeth (especially canines) is virtually eliminated.
- There is a very significant reduction of force levels when only lower anterior teeth contact the bite ramps.
- Condylar position is very easily maintained. The mandible remains “loose.”
- The clear Triad turbos are easily adjusted versus the metal.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
