Dr. Luis Nelson Núñez illustrates treatment phases that lead to precision, predictability, and efficiency
 While self-ligating brackets have proven efficacious in treating a wide variety of malocclusions, they are especially proficient in treating crowding. Active self-ligation has been widely proven to provide better control throughout treatment, and the In-Ovation® line of products is undoubtedly the best. In this review, you will notice how effectively and efficiently In-Ovation® C brackets performed. I’ve had the opportunity to work with many different appliances during my professional career, and I’ve found the
While self-ligating brackets have proven efficacious in treating a wide variety of malocclusions, they are especially proficient in treating crowding. Active self-ligation has been widely proven to provide better control throughout treatment, and the In-Ovation® line of products is undoubtedly the best. In this review, you will notice how effectively and efficiently In-Ovation® C brackets performed. I’ve had the opportunity to work with many different appliances during my professional career, and I’ve found the
In-Ovation brackets give me everything I need to finish cases with precision, predictability, and efficiency. One of the most controversial points about self-ligating brackets is the torque expression during the final phase of treatment. However, Dr. Celestino Nobrega has proven that
In-Ovation active SL brackets express 100% of their torque values when combined with a .019 x .025 stainless steel archwire.1
In my daily practice, I want to be as efficient as possible, avoiding complications and enjoying the day with my patients. During this article, we will explore a brief description of the treatment phases related to the archwire sequence.
Class I with severe lower crowding and upper central incisors up-righting
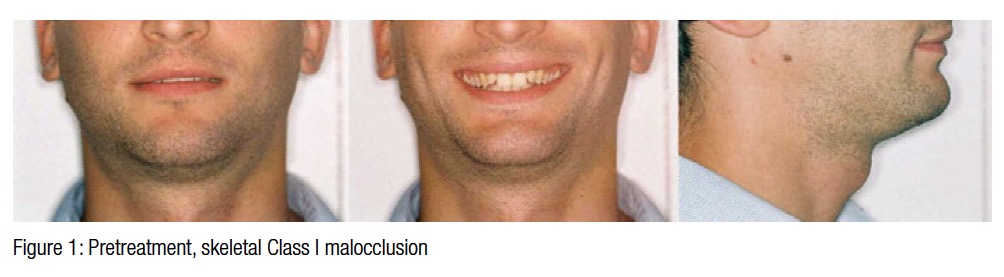
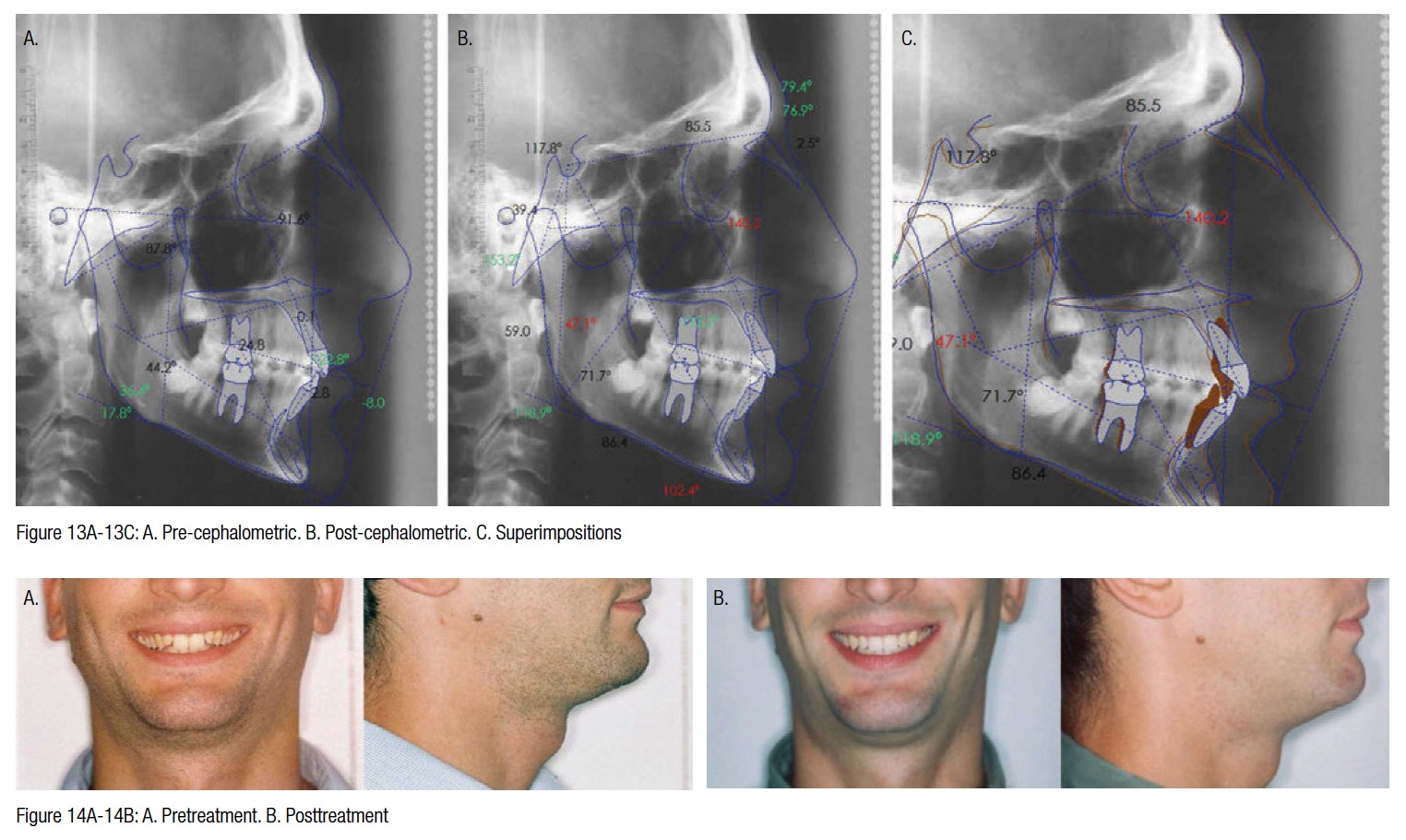
This male adult patient has a brachicephalic biotype with a skeletal Class I malocclusion. The frontal image shows an asymmetry, with his left hemi face higher and behind the contra-lateral side. The profile image shows a bi-retrusion of the lips, resulting in a concave profile.
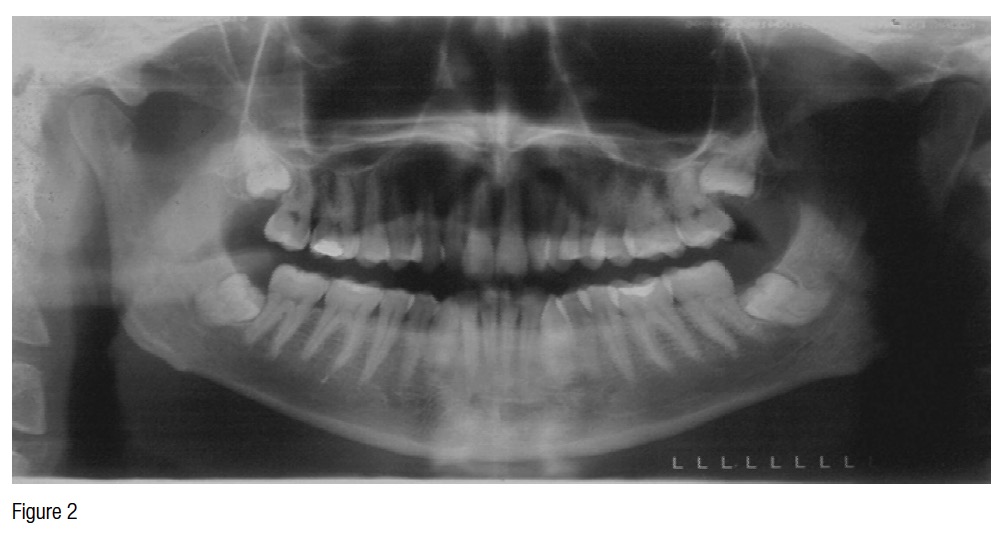
On the pretreatment dental panoramic radiograph, the position of the third molars and the extrusion of the lower incisors can be seen. The third molars will be extracted after the orthodontic treatment.
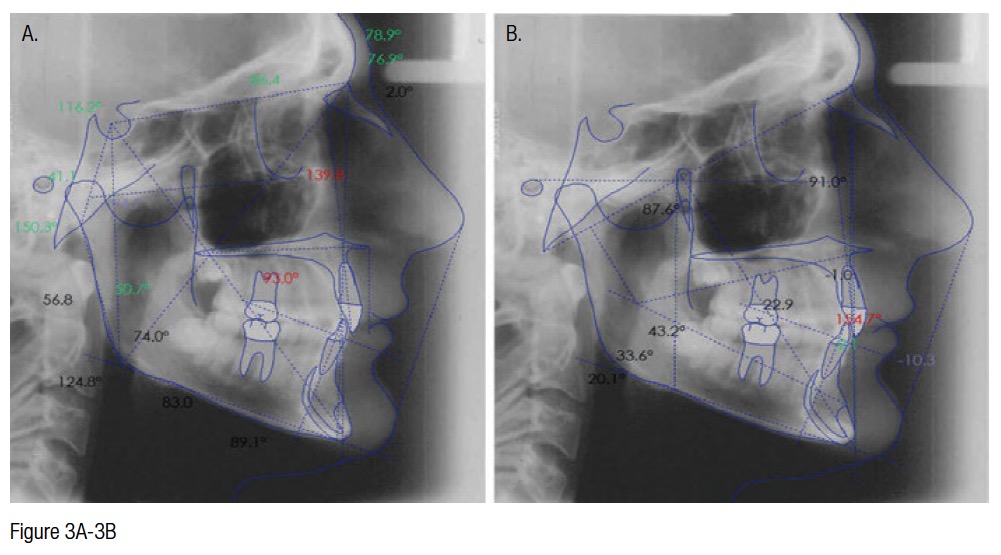
After performing the Björk cephalometric and Ricketts analyses, we can see that the patient has a strong symphysis that is camouflaging a mandibular Class I.
With the soft tissue tracing, we confirm the bi-retrusion of the lips. Also, a high uprighting of the upper incisors can be diagnosed.
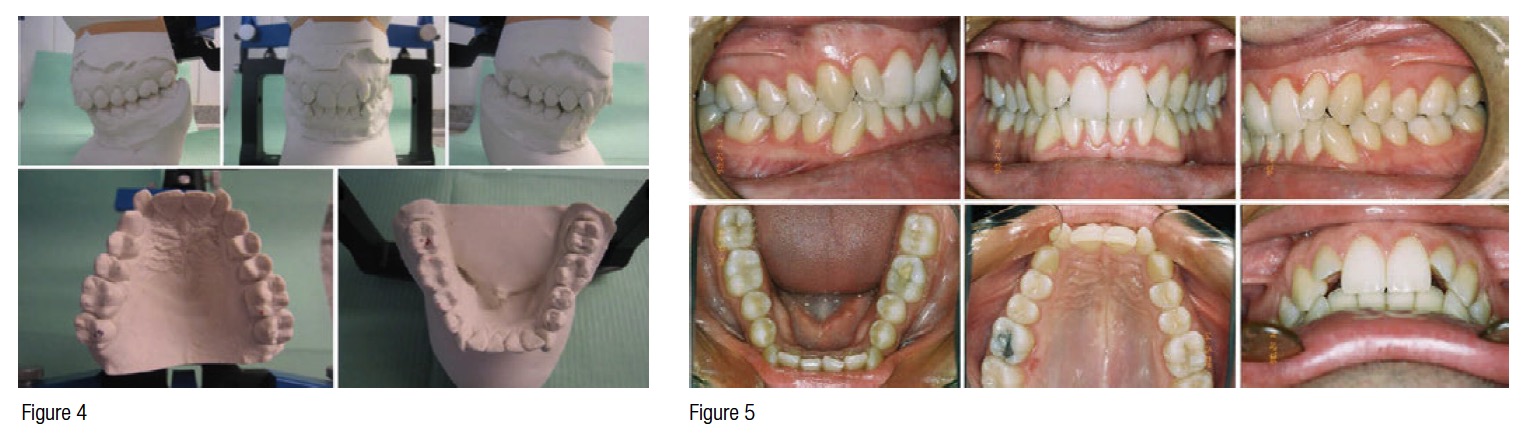 When mounting the model in centric relation, it’s evident that there’s a small opening of the bite generated by the premature contact between right second molars (a slight bilateral cuspids Class II).
When mounting the model in centric relation, it’s evident that there’s a small opening of the bite generated by the premature contact between right second molars (a slight bilateral cuspids Class II).
The initial pictures show good gingival health and oral hygiene. In OC, molars and cuspids are in Class I. The overjet is too tight, and the overbite is almost 3 millimeters. Both dental alveolar arches are square in shape, and in the lower one there is a negative discrepancy of 6 to 7 millimeters. The lower cuspids are proclined or tipped mesially, which makes us think about a fast protrusion of incisors and bite opening as soon as we introduce the preprogrammed appliance and first archwire.
Diagnosis
- Male adult patient
- Brachyfacial
- Skeletal Class I
- Good periodontal health
- TMJ without any dysfunctional sign
- Retrusion of both lips
- Prominent chin
- Molar Class I and cuspids in relative Class I in OC and slight Class II on the way to CR with premature contact between both right second molars
- Square type dental arches
- Uprighting of upper and lower incisors
- Lower dentoalveolar discrepancy of 6 to 7 millimeters and peg upper lateral incisors
Treatment plan
 First stage
First stage
 First stage
First stageLeveling and aligning: Level and align; begin giving ovoid shape to both dental arches; protrude and torque upper central incisors to make room for lower brackets; protrude lower incisors to move lower cuspids into the dental arch.
Second stage
Working stage: Give torque; level occlusal plane until getting parallel archwires; fully express the prescription; reshape peg lateral upper incisors. It is important in this patient to get to full-size archwires and to reach our goal of a flat occlusal plane and good overbite.
Third stage
Finishing stage: Seat the occlusion. Appliance: In-Ovation C Roth .022
Retention: Fixed 3 x 3 in the lower arch and fixed 2 x 2 plus a Hawley retainer in the upper one.
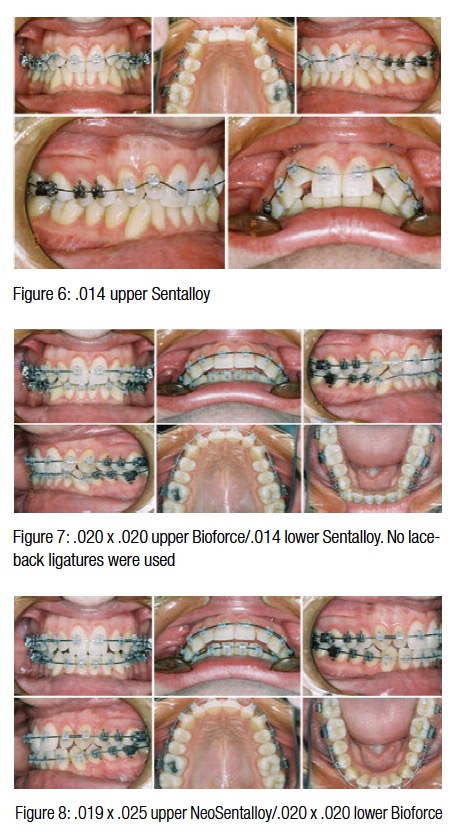
Archwire sequence
First stage
A .014 Sentalloy® (Dentsply GAC) superelastic nickel-titanium archwire was in place for 10 weeks until the leveling and aligning allowed me to move forward to the .020 x .020 Bioforce®. This second archwire is also a superelastic nickel-titanium wire, but with three progressive forces in its internal structure. The Bioforce archwire releases the appropriate force on the molars to prepare the anchorage, on the cuspids and premolars giving the ovoid shape to the dental arch, and a lighter force on the single-rooted teeth to correct their positions. The Bioforce archwire was in place for 8 weeks.
Second stage
A .019 x .025 Neo-Sentalloy® super-elastic nickel-titanium archwire was inserted to begin the working stage. This archwire had to give dental arches the final ovoid shape, express the appliance prescription, express any possible bonding mistake, and show the size discrepancy of the peg upper laterals. A .021 x .028 Neo-Sentalloy archwire and .021 x .025 stainless steel archwire shared the objective of flattening the occlusal plane and closing the open bite generated during treatment evolution.
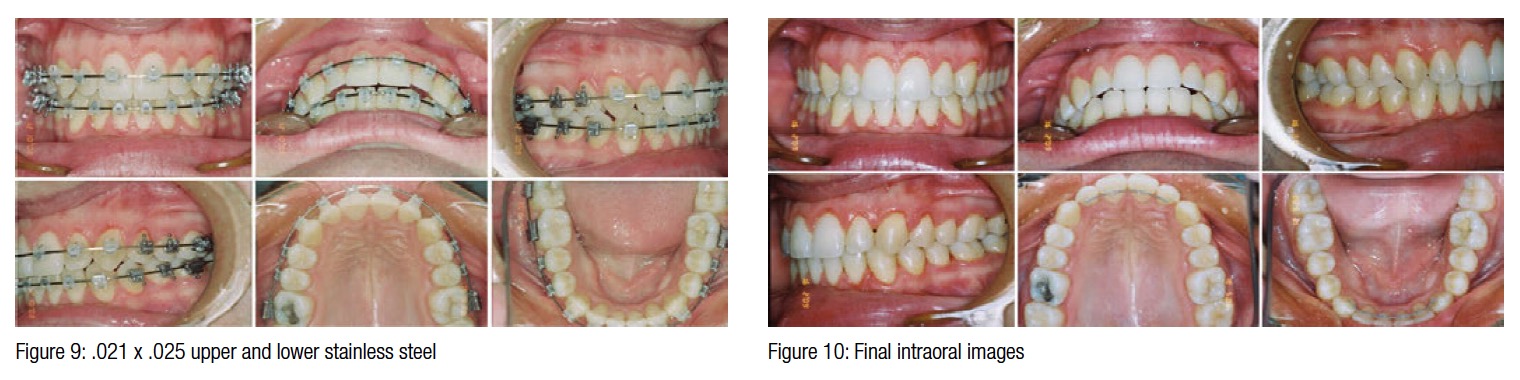
Third stage
A .021x.025 braided archwire is my preferred choice for finishing most cases. With its rectangular section and flexibility, this archwire gives the orthodontist the possibility to seat the occlusion with elastics and to let teeth get their individuality back.
Clinical images
As you may notice, the overbite almost inverted at this point. Remember, we planned to move forward in the archwire sequence until we reached full-size wires in order to make the wires parallel and correct this quasi-open bite.
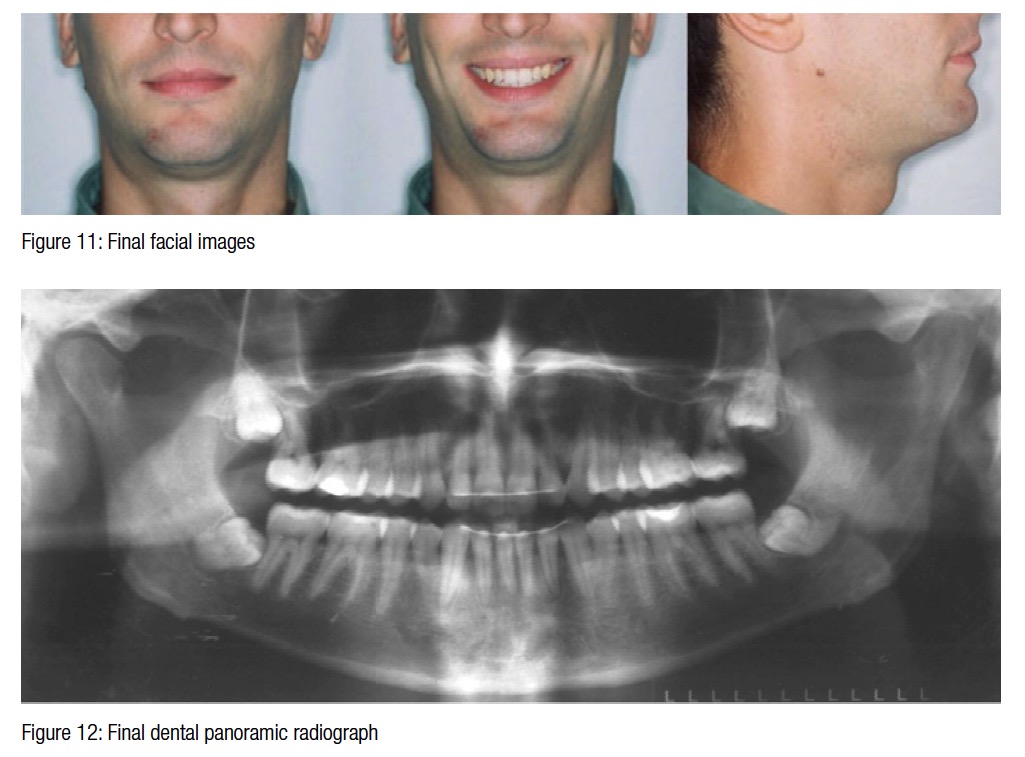 The orthodontic correction achieved during treatment made it possible to get this final result on the face of the patient. The lower third (lips) had a nice improvement just by correcting the torque on the incisors.
The orthodontic correction achieved during treatment made it possible to get this final result on the face of the patient. The lower third (lips) had a nice improvement just by correcting the torque on the incisors.
The results of this case were so satisfying that it helped convince me to use In-Ovation R and In-Ovation C Roth (and CCO) in all my cases.
The secret to achieving results of this kind in all patients is to know the appliance we will be working with and the appropriate archwire sequencing for each case. Knowing the appliance will give us the chance to get the best out of it in regular situations and how to work with it to overcome any complications that may arise.
 Dr. Luis Nelson Núñez, DMD, MS, graduated from the Uruguayan Public University, UDELAR, where he also received his Orthodontic training. He is a graduate of the Roth/Williams Center at the Uruguayan Catholic University.
Dr. Luis Nelson Núñez, DMD, MS, graduated from the Uruguayan Public University, UDELAR, where he also received his Orthodontic training. He is a graduate of the Roth/Williams Center at the Uruguayan Catholic University.
Currently, Dr. Núñez is an Assistant Professor at the UDELAR Orthodontics and Dento-Facial Orthopedics Department, a position he has held for the last 10 years. He also teaches the short-term Orthodontics courses at the NYU for Latin American Doctors. Dr. Núñez is a member of the Uruguayan Orthodontists Society, Latin American Orthodontists Association, and the World Federation of Orthodontists. Dr. Núñez serves as the Latin American consultant for DENTSPLY GAC. He runs a private practice in Montevideo, Uruguay.
- Nobrega C. Biomechanical behavior of self-ligating interactive systems. Ortho CE – North American Edition. 2014;3(1).
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
