CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This clinical article aims to discuss a technique that facilitates the correction of crossbites and Class III malocclusions.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article.
Correctly answering the questions will demonstrate the reader can:
- Identify some traditional treatments for correction of crossbites.
- Identify the technique that includes using V-bends to intrude anterior and posterior teeth.
- Recognize the rationale behind the V-bend approach.
- Outline the technique using V-bends.
- Identify the torquing activations of both maxillary and mandibular archwires for bilateral crossbite final correction.

Dr. Suhail A. Khouri discusses a technique that facilitates the correction of crossbites and Class III malocclusions
Abstract
Palatal expanders have long been the principal treatment for the correction of crossbites over the last century, despite their lengthy fabrication procedures, possible complications, and difficulty in achieving satisfying results. Although advances have affected every aspect of the orthodontic specialty over the past few decades, researchers have not found a simpler alternative approach other than palatal expanders for crossbite correction. This study attributes the extreme difficulty of current crossbite correction approaches to the cuspal blockage of posterior teeth perpetuated by the persistent chewing habit and suggests that even the vigorous forces of traditional expander hardware are incapable of eliciting the corrective lateral teeth movement.
Eliminating this cuspal blockage and disengaging posterior teeth constitutes the rationale for a new treatment approach that allows transverse forces to have effectiveness in transverse teeth movements. Placing composite buildups on the occlusal surfaces of posterior mandibular teeth disengages the occlusion and temporarily breaks the shifted chewing habit during the corrective procedure and enables the light and consistent transverse forces of regular super elastic archwires to the transverse teeth movements.
Also, inserting V-bends in both super elastic archwires by Bendistal pliers, can intrude anterior and posterior teeth and extends the time of anterior and posterior teeth disengagement. This facilitates the posterior crossbite correction, mandibular incisor retraction, and simultaneously treats any coexisting Class III malocclusion. With this simplified approach, clinicians can easily activate regular NiTi archwires to deliver vertical intrusive forces, and transverse crossbite corrective forces at buccal, rather than palatal sides of teeth for correcting those challenging malocclusions. This paper displays several patient therapies using this innovative technique.
Introduction
Removable acrylic expanders and Frankel appliances have been widely used for correcting posterior crossbites1-3 with complete patient cooperation.4-5 To ensure their efficiency without patient cooperation, fixed cemented to posterior teeth6-10 — such as a quad helix, Hyrax appliance, and others11-15 — were developed and dominated the trend of this correction. They were mainly used for opening the midpalatal sutures in prepubertal patients; opening closed sutures typically requires surgery to open the palatal suture to facilitate palatal expansion in adult patients.16-18

To simplify the crossbite correction and reduce the hardware involved, some researchers have developed the palatal arches approach19,20 that could move molars in more than one plane. But the high skill and precision required in this customization, activating and placing them in the patient’s palate, have limited their clinical applicability. More recently, thick super elastic wires were introduced to replace stainless steel in making fixed palatal expanders,21-24 in order to deliver lighter and more consistent expanding forces than traditional expanders. Despite the success using all these laboratory-dependent expanders, their costly clinical and lab fabrication procedures have added to patients’ inconvenience and made finding a simpler treatment strategy a professional requisite.

Most expanders deliver their vigorous expansion forces from the lingual surfaces of the posterior teeth. Thus, the question is, Why have there not been attempts in the past 100 years to apply forces from the buccal surfaces of teeth by activating archwires? This article offers an alternative concept and rationale that satisfies this objective.
Rationale of this approach
Although the height of D as shown in Figure 1A does not seem deep enough to block the buccal cusps of maxillary molars from achieving corrective jumps over the mandibular molar cusps, actually they can and do. This small occlusal depth incapacitates even the expander’s vigorous forces from overcoming the abnormal chewing and locking habit, which makes crossbite correction difficult. This new crossbite corrective approach starts by eliminating occlusal blockage by placing composite buildups on mandibular molars (Figure 1B), which frees the interlocked teeth to expand.
The technique
Clinicians have previously used composite buildups on anterior teeth to open the bite and correct crossbites.25-27 But this new technique places the composite buildups on the central grooves of mandibular posterior teeth (Figure 1B), which disengages posterior and anterior teeth, and temporarily breaks the persistence of the altered chewing pattern.
This approach recruits the following elements already available to orthodontists:
- Bendistal pliers to insert lasting V-bends that launch vertical NiTi forces.
- Recruits the vertical light, consistent forces of NiTi wires in simplifying teeth intrusion.
- Harnesses this intrusion to simplify the correction of crossbites and Class III malocclusions.
Disengaging posterior teeth makes it possible for light transverse forces launched by step out/in V-bends of regular NiTi archwires to move teeth out of crossbites without blockage. The therapy starts by using 0.016″ NiTi archwires for the initial alignment in both dental arches. After aligning all teeth, insert intrusive V-bends with Bendistal pliers’ intraorally distal to the canines. The tips of these bends should always point occlusally in both maxillary and mandibular archwires to intrude posterior and anterior teeth located on both sides of these bends. This intrusion permits occlusal disengagement and allows buccal forces from regular archwires to expand the maxillary molars and correct posterior crossbites. This also and facilitates retraction of the mandibular incisors to correct Class III malocclusions.
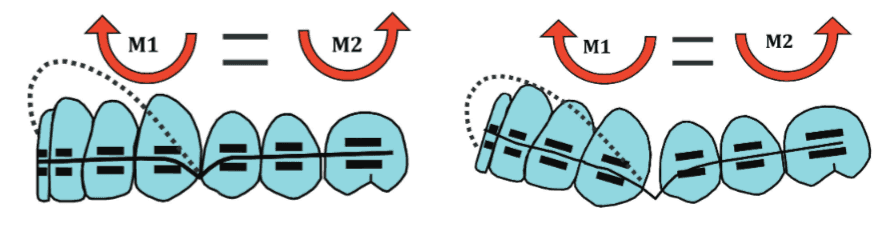
The use of NiTi archwires in this technique not only simplifies initial teeth alignment without loops, springs, or helixes, while their light and consistent forces of V-bend mechanics applied on both sides also simplifies intrusion and occlusal disengagement. Additionally, the extrusion of adjacent canines and first premolars on both sides of the maxillary V-bends have the advantage of augmenting the disengagement of the more distant teeth (Figure 2). Similar but inverted, V-bends in mandibular archwires will double the extent and time of teeth disengagement and will assist the simultaneous correction of crossbite and Class III malocclusion. Rectangular 0.016″ x 0.022″ NiTi archwires, or larger, with V-bends, will deliver relatively stronger forces when more disengagement is required.
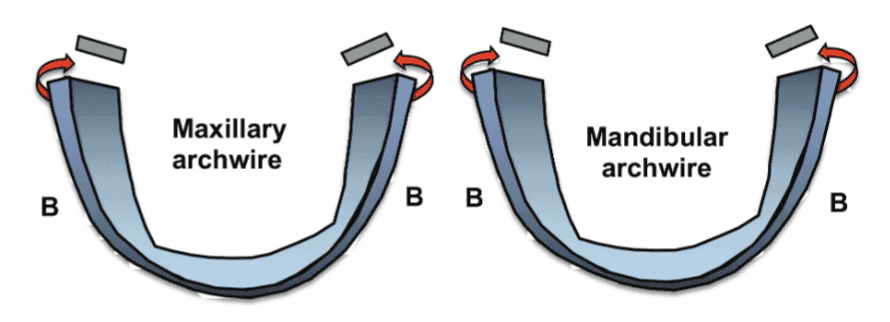
A V-bend inserted in the midline of a maxillary NiTi archwire will activate it to bilaterally and gently expand the maxillary posterior teeth (Figure 3B). Double opposite transverse V-bends can activate archwires to expand and/or constrict posterior teeth on the affected sides. Flexibility of NiTi archwires allows easy engagement of step bends for more efficient and faster movement of teeth. These mechanics continue for about 2 to 4 months until restoration of anterior and posterior teeth overjets. Afterward, remove the composite buildups and pursue further stages of treatment, including closing the resulting open bites, using finishing archwires and intermaxillary elastics to bring treatment to the normal occlusal standards. When dealing with more severe skeletal cases, torquing of stainless steel 0.016″ x 0.022″ archwires or larger (Figure 4) can restore the normal crown’s overjet, and correct the abnormal bucco-lingual roots axial inclinations often found in crossbites, and help establish stability (Figure 5).

Torquing effects
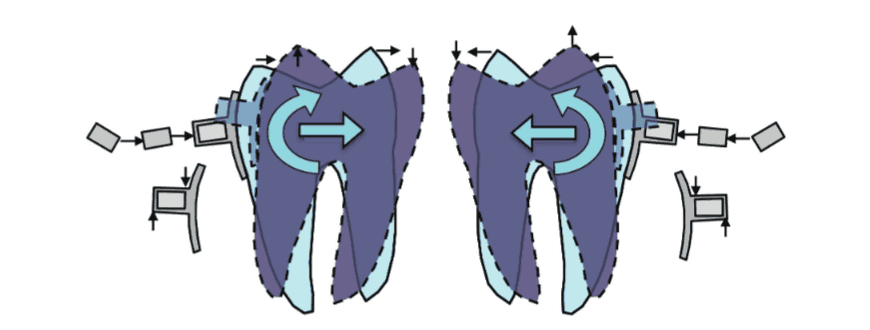
Torquing activations of maxillary and mandibular stainless steel rectangular archwires acting on posterior teeth, as illustrated in Figure 4, will correct the bucco-lingual axial inclination of posterior teeth and finish the correction of bilateral crossbites. Upon inserting the torqued distal parts of archwires in the molar tubes and premolar brackets, moments at the molar tube sites start to expand maxillary posterior teeth crowns and push their roots lingually, while the same direction torque on mandibular archwires constricts mandibular posterior teeth crowns and pushes their roots buccally, as illustrated in Figures 5A and 5B.
Monitoring these mechanics is required at regular visits to avoid undesirable side effects. Overtreatment of 1 mm-2 mm per side helps minimize relapse. Finishing treatment will require the use of bite closing and/or intermaxillary elastics to achieve normal occlusal standards and intercuspation.
Patient 1
Patient 1: Top row shows intraoral photographs of a 16-year-old female patient with a left posterior crossbite involving a segment from left lateral incisor to second premolar. Second row shows an initial NiTi wire with a 6 mm step-up bend fully engaged to brackets of those blocked-out left maxillary teeth to intrude and disengage them as an initial step. Mandibular 0.016” x 0.022” NiTi archwire with intrusive V-bends and composite buildup placed on the left molar enhanced disengagement. Third row shows treatment images showing the halfway movement of the affected canine and premolars before removing the composite. Fourth row shows posttreatment intraoral photographs after 7 months of treatment.
 Patient 2
Patient 2
 Patient 2
Patient 2Patient 2: Top row shows pretreatment models of a 14-year-old female patient with a severe skeletal Class III (7 mm underjet), and bilateral posterior crossbite. Treatment plan called for mandibular first premolars extraction, consolidating existing spaces, and using V-bend 0.016″ x 0.022″ NiTi archwires, which intruded mandibular incisor teeth to create a torque that prevents incisors tipping during the space closing forces. Later, stainless steel archwires helped stabilized retraction of the mandibular incisor teeth. Second row shows final stage of treatment with both bilateral crossbite and Class III malocclusion corrected. Third row shows posttreatment intraoral photographs 3 years after retention. Fourth row illustrates that the posttreatment panoramic and cephalometric radiographs show no root resorption.
 Patient 3
Patient 3
 Patient 3
Patient 3Patient 3: Top row shows intraoral pretreatment photographs of a 14-year-old female patient with a right unilateral posterior crossbite, anterior crowding, and Class III canine relation. Treatment called for four premolar extractions and crossbite correction. Second row shows that after alignment, the interlock, the composite buildups on mandibular molars enhanced by the bend. Bends on maxillary and mandibular 0.016″ x 0.022″ NiTi archwires disengaged posterior teeth. Third row shows the correction of crossbite and Class III relations have been achieved at the finishing stage. Bottom row shows the posttreatment photos using this technique.
 Patient 4
Patient 4
 Patient 4
Patient 4Patient 4: First row shows the pretreatment photographs of a 14-year female patient with severe left side posterior crossbite and deep Class III malocclusion. Second row shows the use of composite buildups and the V-bend NiTi archwires disengaged posterior and anterior teeth on both side, and facilitated correction of the massive crossbite and Class III occlusion. Third Row shows posttreatment photos. Fourth row shows pre- and-posttreatment cephalometric radiographs exhibiting improved incisal relation without root resorption.
 Patient 5
Patient 5
 Patient 5
Patient 5Patient 5: Top row shows retreatment intraoral photos of a 15-year-old female patient with total right unilateral posterior crossbite and Class III malocclusion. Second row shows the intrusive effects of the V-bend 0.016” x 0.022” NiTi archwires disengaged anterior and posterior teeth in the right side without composite buildups, allowing effective transverse forces of activated archwires to correct this massive crossbite and the Class III relation as well. Bottom row shows the posttreatment intraoral photos.

Patient 6:
Top row shows pretreatment intraoral photographs of a 13-year old female patient with a bilateral crossbite and class III tendency. Nonextraction treatment was performed using the V-Bend technique as usual. Second row shows post treatment photographs.
 Discussion
Discussion
 Discussion
DiscussionThis article presents a diagnostic ration-ale for the difficulty of current strategies of crossbite correction and provides a solution for them. Molar cusp blockage accentuated by the persistent shift of chewing acts as an anchorage to elicit unwanted undesirable expansion of the normal side of maxillary teeth only.
This article illustrates how Bendistal pliers can place V-bends on NiTi archwires, which launches light and consistent forces that create moments that facilitate the correction of crossbites and Class III malocclusions simultaneously.
Furthermore, it shows how torquing stainless steel rectangular archwires can help restore normal bucco-lingual axial inclinations of the teeth involved in the crossbites and enables the corrections.
This approach conserves chair time, laboratory time, and cost involved in expander’s custom-making and provides convenience to patients and orthodontists who can correct these challenging orthodontic problems by activating adjustment of regular archwires during patient’s routine visits.
Posterior crossbites can also result in facial asymmetries. Read Dr. Bradford N. Edgren’s article, “Facial asymmetries,” to explore how appropriate early orthodontic treatment can successfully improve and resolve facial asymmetries in young patients
References
- McDougal PD, McNamara JA Jr, Dierkes JM. Arch width development in ClassII patients treated with the Fränkel appliance. Am J Orthod. 1982;82(1):10-22.
- Brin I, Ben-Bassat Y, Blustein Y, et al. Skeletal and functional effects of treatment for unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 1996;109(2):173-179.
- Firatli S, Ulgen M. The effects of the FR-3 appliance on the transversal dimension. Am J Orthod Dentofacial Orthop. 1996;110(1): 55-60.
- Kirjavainen M, Kerjavainen T, Haavikko K. Changes in dental arch dimensions by use of an orthopedic cervical headgear in ClassII correction. Am J Orthod Dentofacial Orthop. 1997;111(1):59-66.
- Kirjavainen M, Kerjavainen T. Maxillary expansion in ClassII correction with orthopedic cervical headgear. A posteroanterior cephalometric study. Angle Orthod. 2003;73(3):281-285.
- Erdinç AE, Ugur T, Erbay E. A comparison of different treatment techniques for posterior crossbite in the mixed dentition. Am J Orthod. Dentofacial Orthop. 1999;116(3):287-300.
- Boyson B, La Cour KA, Thanasiou AE, Gjessing PE. Three-dimensional evaluation of dentoskeletal changes after posterior cross-bite correction by quad-helix or removable appliances. Br J Orthod. 1992;19(2)97-107.
- Wedrychowska-Szule B. [Treatment of lateral cross-bite with active plates in condition of raised dental occlusion and by the quad helix method]. [Article in Polish] Ann Acad Med Stetin. 1995;41:233-243.
- Bench RW. The quad helix appliance. Semin Orthod. 1998;4(4):231-237.
- Erverdi N, Okkar I, Kücükkeles N, Arbak S. A comparison of two different rapid palatal expansion techniques from the point of root resorption. Am J Orthod Dentofacial Orthop. 1994;106(1):47-51.
- Braun S, Bottrell JA, Lee KG, Lunazzi JJ, Legan H. The biomechanics of rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2000;118(3):257-261.
- Memikoglu TU, Iseri H. Effects of a bonded rapid palatal expansion appliance during orthodontic treatment. Angle Orthod. 1999;69(3):251-256.
- Toroglu MS, Usel E, Kayalioglu M, Uzel I. Asymetric maxillary expansion (AMEX) appliance for treatment of true unilateral posterior crossbite. Am J Ortho Dentofacial Orthop. 2002;122(2):164-173.
- Chang JY, McNamara JA, Herberger TA. A longitudinal study of skeletal side effects induced by rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 1997;112(3):330-337.
- Bell RA, LeCompte EJ. The effects of maxillary expansion using a quad helix appliance during the deciduous and mixed dentitions. Am J Orthod. 1981;79(2):152-161.
- Bell WH, Jacobs J. Surgical-orthodontic correction of horizontal maxillary deficiency. J Oral Surg. 1979;37(12):897-902.
- Lehman JA Jr, Haas AJ, Haas DG. Surgical-orthodontic correction of transverse maxillary deficiency: a simplified approach. Plast Reconstr Surg. 1984;73(1):62-68.
- Chung CH, Goldman AM. Dental tipping and rotation immediately after surgically assisted rapid palatal expansion. Eur J Orthod. 2003;25(4):353-358.
- Wichelhaus A, Sander C, Sander FG. Development and biomechanical investigation of a new compound palatal arch. J Orofac Orthop. 2004;65(2):104-122.
- Baldini G, Luder HU. Influence of arch shape on the transverse effect of transplalatal arches of Goshgarian type during application of buccal root resorption. Am J Orthod. 1982;81(3):202-208.
- Ciambotti C, Ngan P, Durkee M, Kohli K, Kim H. A comparison of dental and dentoalveolar changes between rapid palatal expansion and nickel-titanium palatal expansion appliance. Am J Orthod Dentofacial Orthop. 2001;119(1):11-20.
- Karaman AI. The effects of titanium maxillary expander appliances on dentofacial structures. Angle Orthod. 2002;72(4):344-354.
- Ferrario VF, Garattini G, Colombo A, et al. Quantitative effects of nickel-titanium palatal expander on skeletal and dental structures in primary and mixed dentition: a preliminary study. Eur J Orthod. 2003;25(4):401-410.
- Kenworthy CR, Sheats RD. A bonded functional ramp to aid in asymmetric expansion of unilateral posterior crossbites. Am J Orthod Dentofacial Orthop. 2001;119(3):320-322.
- Tzatzakis V, Gidarakou I. Correction of anterior crossbite using occlusal buildups. J Clin Orthod. 2007;4(7):393-397.
- Tzatzakis V, Gidarakou I. A new clonical approach for the treatment of anterior crossbites. World J Orthod. 2008;9(4):355-365.
- Janakiraman K, Abadi S, Nanda R, Uribe F. An alternative method for correcting unilateral posterior crossbite with functional shift in an adult patient. J Clin Orthod. 2015;49(8):525-532.
- Khouri SA. Using V-bends on NiTi Wires for nonsurgical correction of Class III malocclusions. Orthodontic Practice US. 2016;7(1):24-2
