CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to discuss the preferred amount of facial protrusion for orthodontic
treatment among 21st century African American people.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions on page XX to
earn 2 hours of CE from reading this article. Correctly answering the questions will
demonstrate the reader can:
- Realize that patients of different races, genders, and generations have subtle
differences in their esthetic preferences. - Identify the characterization of African Americans’ historical perception of beauty.
- Recognize the possible orthodontic esthetic preferences of African Americans.
- Realize that esthetic preferences have changed from the early 90s to the current time.
- Realize the importance of understanding the patient’s preference regarding the protrusion threshold when planning orthodontic treatment.

Dr. Larry White discusses a simple and easily managed apparatus
Introduction
Cantilevers offer orthodontists perhaps the most simple and easily managed apparatus for solving Class II malocclusions because they give clinicians statically determinate and efficient mechanisms that they can employ without fears of uncontrollable and unneeded side effects.
Cantilevers are simple beams secured at one end and free on the other. The secured end will carry a load and produce a force and a moment, whereas the free end will attach with a one-point contact and produce only a force with no accompanying moment.
Orthodontists will use cantilevers as Class I levers where the effort is usually applied via a single point of contact with a tooth or wire and where the resistance will be within a tube or bracket. Orthodontic cantilevers can also have a reactive anchor within the acrylic of a removable or fixed appliance and the free end touching a tooth or wire at only one point.1
 Cantilever corrector designs
Cantilever corrector designs
Nanda2 fabricated a cantilever for correcting Class II malocclusions (Figure 1) using a design by Burstone.3,4 The elastic activates the cantilever by providing a distal force to the molar, which creates a strong moment that tips the molar distally. The resultant force from the cantilever and the elastic is downward and backward (Figure 2).
An alternate strategy for producing similar movements on the molar is with a two-piece cantilever that uses an anterior sectional arch in the incisor brackets. This cantilever design has the disadvantage of intruding the maxillary incisors, which is seldom indicated. Clinicians can offset this intrusion by applying Class II elastics to the anterior sectional wire.

The Pendulum Appliance5 (Figure 4) offers another illustration of a cantilever that fixes the wire within the acrylic of the mechanism, while the free end of the wire makes a one point contact within the lingual sheath of the molar.

The Carriére® Motion™ Appliance (Figure 5), on the other hand, has the fixed, reactive part of the cantilever beam attached to the canine or premolar, while the active part has a one point contact via the rotational ball-and-socket that works against the molar. This mechanism is totally dependent upon the patient wearing Class II elastics to the anterior part of the cantilever to effect movement of the teeth. A new and different Class II cantilever
This article displays a simplified Class II cantilever that requires minimal instrumentation, which orthodontists typically have in their armamentarium.
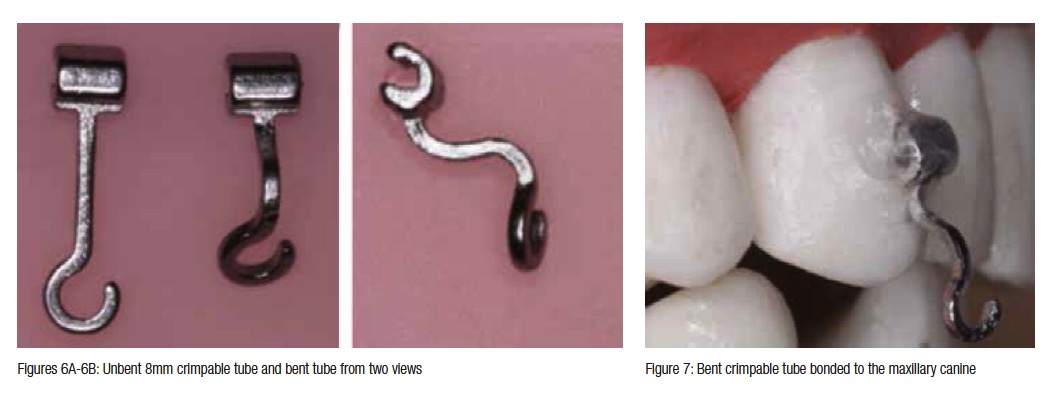
An 8 mm crimpable hook is bent 90° twice to give a horizontal span to which a sectional archwire hook can attach (Figures 6A and 6B). The bent tube is then bonded to the canine with a light-cured composite (Figure 7).
A slightly long .016 x .022 stainless steel sectional archwire is made with a large omega loop that abuts the molar tube on one end and a hook that will have a one-point contact against the bent crimpable hook bonded to the canine. The sectional archwire is tipped upward about 45°, and when the omega loop touches the molar tube, the anterior cantilever hook will lie forward of the bonded canine attachment by 1 mm-2 mm. As the sectional archwire is brought occlusally and attached to the horizontal span of the crimpable hook, it will slightly compress the omega loop, which will created a distal force on the molar along with a strong clockwise moment and, simultaneously, will produce a forward and intrusive force on the canine but no moment (Figure 8). Class II elastics or NiTi springs will cancel the intrusive and anterior forces on the canine (Figure 9). 
 Figures 10-13 illustrate an adolescent female patient treated with this Class II cantilever mechanism.
Figures 10-13 illustrate an adolescent female patient treated with this Class II cantilever mechanism.
Conclusion
Class II malocclusions account for some of the most formidable challenges orthodontists encounter, which clinicians have sought to solve with complicated and expensive mechanisms — e.g., Herbst, Jasper Jumpers, Forsus, MARA, Distal Jet, Pendulum, Carriére® Motion™, etc.
The Class II cantilever corrector featured in this article offers the profession a simple, effective,  efficient, and inexpensive technique of correcting Class II malocclusions with sound Newtonian principles without the harmful side effects of the aforenamed appliances. The Herbst, Jasper Jumper, MARA, and Carriére Distalizer and other fixed interarch functionals ordinarily displace the mandibular incisors excessively facially, while the Pendulum, Distal Jet, and other intra-arch appliances force the maxillary incisors facially.
efficient, and inexpensive technique of correcting Class II malocclusions with sound Newtonian principles without the harmful side effects of the aforenamed appliances. The Herbst, Jasper Jumper, MARA, and Carriére Distalizer and other fixed interarch functionals ordinarily displace the mandibular incisors excessively facially, while the Pendulum, Distal Jet, and other intra-arch appliances force the maxillary incisors facially.
 This cantilever corrector requires a minimum of instrumentation, instruction, and skill to implement and permits clinicians to solve the most difficult feature of Class II malocclusions at the initiation of treatment when patients are likely to display more enthusiasm and compliance. Once the Class II malocclusion has changed into Class I, the malocclusion becomes much easier to complete.
This cantilever corrector requires a minimum of instrumentation, instruction, and skill to implement and permits clinicians to solve the most difficult feature of Class II malocclusions at the initiation of treatment when patients are likely to display more enthusiasm and compliance. Once the Class II malocclusion has changed into Class I, the malocclusion becomes much easier to complete.
References
- Melsen B, Fiorelli G. Biomechanics in Orthodontics. 3rd ed. Aarhus, Denmark: 2013. https://www.ortho-biomechanics.com.
- Nanda R. Biomechanics in Clinical Orthodontics. Philadelphia, PA: W.B. Saunders; 1997.
- Burstone CJ. Precision lingual arches. Active applications. J Clin Orthod. 1989:23(2):101-109.
- Hoederath H, Bourauel C, Drescher D. Differences between two transpalatal arch systems upon first-, second-, and third-order bending activation. J Orofac Orthop. 2001;62(1):58-73.
- Hilgers JJ. The pendulum appliance for Class II noncompliance therapy. J Clin Orthod. 1992;26(11):706-714.
- Carrière L. A new Class II distalizer. J Clin Orthod. OP 2004;38(4):224-231.
