CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to discuss some clinical aspects to increasing consistency using a “Straight-Wire Appliance.”
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions in our online quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize certain clinical benefits to passive self-ligating mechanisms.
- Identify Active Early Case Management Protocols.
- Realize the importance of diagnosing in natural head position.
- Identify some aspects of torque expression.
- See the value of optimizing microesthetics in finishing.

Drs. Tom Pitts and Duncan Brown discuss an efficient, gentle approach to orthodontic treatment
“Everything should be made as simple as possible, but not simpler.” — Einstein
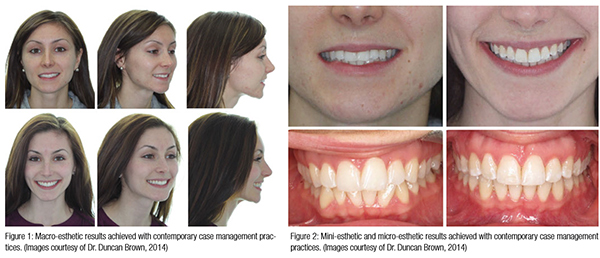
Orthodontic clinical procedures and esthetic preferences are evolving toward fuller lips, greater enamel display, and wider smiles with a reduced tendency toward four-premolar extractions, with increased preference for non-extraction treatment.1 The clinical approaches that we rely on today are different from those earlier generations of orthodontists used frequently.1 Esthetic declines, once common with treatment,2 are no longer acceptable to the majority of patients, and “straight teeth,” once the predominant treatment goal, is now secondary to strategies directed toward esthetic improvement3 (Figures 1-2).
Most orthodontists use a variation of the “Straight-Wire Appliance,” a concept that has dominated our profession since Dr. Larry Andrews’ breakthrough article4 led to its development in the 1970s. In the last 2 decades, appliance developments have revolved around relatively minor changes in appliance prescription, direct bonding, the development of PSL (Passive Self-Ligating)/ASL (Active Self-Ligating) ligating mechanisms, increased use of sliding mechanics, and incorporating reduced force levels.5
The recognition that certain torsion concepts of “straight-wire” theory are not congruent with some modern esthetic goals or with contemporary mechanics does not diminish the value of Dr. Andrews’ landmark concepts. Orthodontists must appreciate the biomechanical flexibility that is required to use the appliance for improving the quality of treatment results.
There was a gain in popularity in ASL/PSL systems during the 1990s when small wires in a larger “closed” slot provided effective movement due to reduced Resistance to Sliding (RTS). For many orthodontists, when larger rectangular wires were used during major tooth movement, results were disappointing5 with “sloppy slots” that lacked control of axial inclination and rotations.Passive ligation demands very accurate slots with special dimensions, particularly in the anterior region for obvious reasons.
We favor the use of a PSL mechanism for many reasons: quick wire changes, consistent bracket engagement, lower forces and wire sliding with control, and improved hygiene, among others. We combine proven PSL case management strategies6 and “Active Early” approaches7 to control torsion and arch development, with the improved slot geometry and tighter tolerances of the H4™ appliance (Ortho Classic), along with more esthetic arch forms.
Clinical Tips
- Don’t get stuck in a biomechanics rut that doesn’t deliver exceptional esthetics: (Impressive Smile and Facial Esthetics has been my field of interest for the last many years.) Most orthodontists appreciate Andrews’ “Six Keys to Normal Occlusion” — (Key 1) the characteristics of molar relationship, (Key 2) crown angulation or tip, (Key 3) crown inclination, (Key 4) no rotations, (Key 5) absence of spaces, and (Key 6) occlusal plane — as being important features of a sound functional occlusion. The work of Dr. David Sarver clearly describes characteristics of great esthetics that supplement the criteria applied to normal occlusions8. The biomechanics and case management used by esthetically motivated orthodontists to achieve great occlusions are likely considerably different from those who are mainly occlusally motivated. Put simply, “Great Occlusions don’t always equal great esthetics,” so clinically, find ways to achieve both.
- Try “Active Early” case management protocols: In “Active Early” protocols,7 the appliance is activated as early as possible, using the Smile Arc Protection (SAP9) bracket position to adjust vertical position of the incisors, inverting groups of brackets when necessary to activate torsion in the appliance, selecting archwire progressions that control axial inclination early in treatment, wider arch forms that develop the posterior segments of the arches sooner, esthetic arch shape, ELSE (Early Light Short Elastics) to control forces and moments, and appropriate disarticulation to encourage early “wanted” tooth movements.6 This controls early vertical erupion and intrusion of teeth. Using these strategies improves patient management efficiency for us (Figure 3).
- Diagnose in Natural Head Position (NHP): Diagnosis for esthetics is based on how the patient presents in day-to-day activity.8 As NHP is reasonably stable in both the short- and long-term,10 the patient should be assessed comfortably standing, engaged in natural conversation, and generating unposed smiles. The orthodontist then makes patient specific determinations of bracket height progressions to generate optimal enamel display8 and assesses the requirement for creation of torsion within the appliance to optimize axial inclination of the maxillary anterior teeth (Figure 4). Far too many finished orthodontic patients end up with proclined maxillary incisors, so we are purposeful in the assessment.
 Optimize tooth shape, and improve gingival contour prior to bonding: The value of optimizing micro-esthetics in finishing is well appreciated.11 The less common strategy of creating a normalized contour of the teeth through positive and negative coronoplasty prior to bonding creates a number of opportunities. Ability to place brackets in vertical positions designed to enhance the smile arc, simplified correction of rotational control, and more predictable performance in third order movements are all benefits of normalizing tooth shape and contour prior to bonding. As SAP upper bracket positions to optimize esthetics are frequently more gingival than conventional positions, soft tissue recontouring can be a tremendous advantage when needed (Figure 5).
Optimize tooth shape, and improve gingival contour prior to bonding: The value of optimizing micro-esthetics in finishing is well appreciated.11 The less common strategy of creating a normalized contour of the teeth through positive and negative coronoplasty prior to bonding creates a number of opportunities. Ability to place brackets in vertical positions designed to enhance the smile arc, simplified correction of rotational control, and more predictable performance in third order movements are all benefits of normalizing tooth shape and contour prior to bonding. As SAP upper bracket positions to optimize esthetics are frequently more gingival than conventional positions, soft tissue recontouring can be a tremendous advantage when needed (Figure 5).- Increase torsion “built into” the appliance by “flipping” where needed: Torque expression is a complex process dependent upon12 magnitude of torsion, wire stiffness or resilience, bracket design, engagement angle, mode of ligation, wire dimension and corner radius of the wire, angulation of the bracket, deformation of the bracket or wire under torsion, manufacturing tolerances in the bracket and the wire, initial tooth inclination, bracket position, and the measurement technique used to evaluate torsion. Fortunately, to the clinician, it matters solely when/if torsion is developed within the slot during commonly used archwire progressions.
 Optimize tooth shape, and improve gingival contour prior to bonding: The value of optimizing micro-esthetics in finishing is well appreciated.11 The less common strategy of creating a normalized contour of the teeth through positive and negative coronoplasty prior to bonding creates a number of opportunities. Ability to place brackets in vertical positions designed to enhance the smile arc, simplified correction of rotational control, and more predictable performance in third order movements are all benefits of normalizing tooth shape and contour prior to bonding. As SAP upper bracket positions to optimize esthetics are frequently more gingival than conventional positions, soft tissue recontouring can be a tremendous advantage when needed (Figure 5).
Optimize tooth shape, and improve gingival contour prior to bonding: The value of optimizing micro-esthetics in finishing is well appreciated.11 The less common strategy of creating a normalized contour of the teeth through positive and negative coronoplasty prior to bonding creates a number of opportunities. Ability to place brackets in vertical positions designed to enhance the smile arc, simplified correction of rotational control, and more predictable performance in third order movements are all benefits of normalizing tooth shape and contour prior to bonding. As SAP upper bracket positions to optimize esthetics are frequently more gingival than conventional positions, soft tissue recontouring can be a tremendous advantage when needed (Figure 5).

With the worldwide tendency to treat more patients without extractions, the control of proclination of the maxillary anterior teeth has become a greater challenge. The correction of pre-existing crowding and proclination, proclination associated with relief of crowding during traditional round wire mechanics, or incisor proclination-associated Class III elastics is particularly problematic. The challenge for many non-extraction patients has been in getting enough lingual crown torsion without having to resort to complex wire bending to attain esthetic results. These are patients that benefit from “flipping (upper anteriors) and flocking (upper cupid)” the maxillary anterior/canine brackets.13
The “tooth by tooth” method of varying torsion “built into” the appliance is not as efficient for us and frequently requires either repositioning of brackets, or complex wire bending to finish precisely.14 In contrast, “flipping and flocking” and varying torsion in groups is far more predictable, requires fewer bracket repositions, and allows wire adjustments with uniformly “spun” wires (Figures 6-7).
- Bond brackets to optimize esthetics not at the center of anatomic crown (FA): As today’s treatment targets for incisor position in three planes of space are based on esthetics,8,15 the reliance on “treatment built” into an appliance for the anterior teeth relative to the occlusal plane is not a practical way to ensure esthetically superior results. In the “Active Early” approach, individualized bracket positions based on esthetics7 (SAP) is combined with other initial planning considerations to gain control of maxillary incisor vertical position. For patients with “flat” occlusal planes or those that require increased enamel display, the divergence of the upper wire plane from molar to incisor created by bracket position must increase to develop the smile arc by extruding the upper incisors relative to the upper premolars. In patients with normal occlusal planes, a more modest progression in the upper wire plane is still advisable to protect the smile arc as we broaden the maxillary arch with treatment. A modest progression in still advised in deep bite cases to avoid excessive reduction in the smile arc as the overbite reduces. Compensating changes in the mandibular wire plane levels the mandibular arch and establishes an optimum overbite. It is not necessary to have a deeper bite to have a great smile arc.
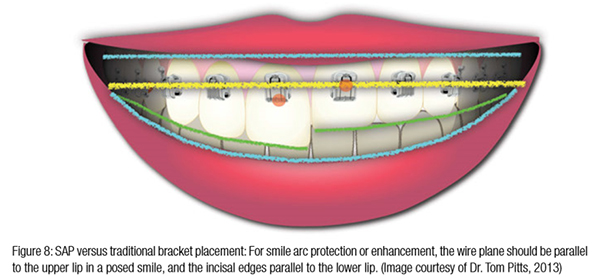
Andrews’ “Six Keys” article, acknowledged as the catalyst for development of the first fully pre-adjusted appliance, advocates using the center of the clinical crown (FA), the long axis of the center of the clinical crown, and the thickness of the clinical crown from the long axis to FA,5 as guides for bracket positioning. This limits the usefulness of the appliance for patients whose teeth or faces deviate from “normal standards.” We do not subscribe to the core “straight-wire” principle that the wire plane must parallel the occlusal plane to attain excellent occlusions, and failure to adjust bracket height to adjust vertical positions of the maxillary incisors can result in esthetic deterioration. SAP bracket placement strategy allows adjustment of the vertical position of the maxillary incisors, which improves their display and the smile arc without increasing the overbite (Figure 8).
- Appreciate the reality of undersize wires and oversized slots: Contemporary fixed orthodontic treatment is usually completed in wire sizes that are less than full dimension15 for the designed bracket slot dimensions. This seems gentler on the patient, and the consequences of this incompletely filled bracket lumen is torsional play that decreases engagement of the contact between the archwire and the bracket.16 While decreasing friction — a potential benefit during early leveling, aligning, and sliding mechanics — torsional play reduces control of axial inclination necessary for ideal esthetics. In clinical practice, incremental increases in archwire size is NOT the most effective means of controlling axial inclination when the slot isn’t filled7 (Figure 9).
- Understand the appliance system you are using: Manufacturing tolerances also vary greatly so that the ability of the appliance to generate torsion with a specific wire progression and deliver stated appliance Rx17 is really what matters. Fortunately, to the clinician, it matters solely when/if torsion develops within the slot during commonly used archwire progressions. Unfortunately, many manufacturer’s tolerances often cause variable slot sizes, which makes torsion unpredictable. However, with the H4 bracket, the manufacturing tolerances are predictably accurate, with reduced slot depth leading to less wire adjustments. By varying bracket height with SAP bracket positioning and “flipping and flocking” maxillary anterior brackets when needed, lingual crown torsion is assured. By proper management of mandibular incisors, those teeth can be kept upright when required (Figure 10).
- Use broader arch forms for better esthetics: Dr. Pitts has found that broader arch width, (not in the canine region) especially in the molars is more attractive, and smaller buccal corridors are preferred in both men and women. The alignment and broadening of maxillary and mandibular dental arches to reduce buccal corridors and producing “10” or “12” tooth smiles results in more space for the anteriors to have more lingual crown torque/inclination. Of course, proper inclination of the premolars and molars must be maintained upon broadening. Research has confirmed that final arch width is a function of arch form, not of the bracket18 used during treatment, so an improved arch form is required for improved esthetics.
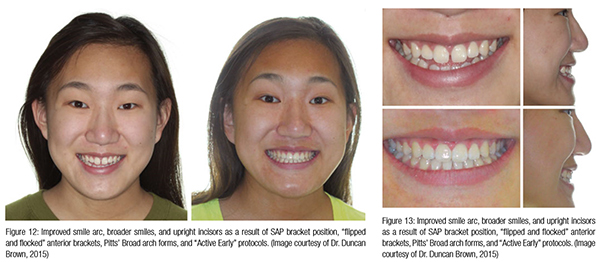
One of the biggest impacts on transverse arch dimension in the molars, and arch form in general has been the adoption of “Pitts’ Broad” arch forms in both nonadjustable and adjustable wire profiles (Ortho Classic). This arch form improves the “flow” of mini-esthetics, making the attainment of a “12 tooth” smile much easier. By using a moderate progression SAP bracket placement, the orthodontist can broaden the arches and still maintain a beautiful smile arc (Figures 11-15). In short, the shape of the arch is just as important as the width.
- Finish micro-esthetics details with optimal esthetics in mind: It was primarily the efforts of Dr. David Sarver who classified the concepts of macro-, mini-, and micro-esthetics19. While optimizing the “white and pink” tissues has been common practice in esthetic dentistry, it is less common in orthodontics20. By mastering the techniques and disciplines applied in cosmetic dentistry, patients have the potential to finish with wonderful micro-esthetics that provide the final touch to patients who have well managed macro- and mini-esthetic results (Figure 16). We take particular care in avoiding “black triangles” at the gingival papilla through management of contacts and connectors during the finishing process.



It is an exciting time to be in orthodontics. Contemporary esthetic-based diagnosis, a modern understanding of how to optimize straight-wire appliances, use of advanced straight-wire appliances that control axial inclination and rotations, using esthetic broader arch forms, adopting the “Active Early” approach to case management, and finishing “white and pink” tissues for esthetics provide expanded opportunities for improving esthetics. In the “Active Early” approach, lighter forces, applied earlier, for longer duration are accomplishing many things more efficiently for the orthodontist and more gentleness for the patient than has ever been possible before.
References
- Janson G, Maria FR, Bombonatti R. Frequency evaluation of different extraction protocols in orthodontic treatment during 35 years. Prog Orthod. 2014;15(1):51.
- Ackerman JL, Ackerman MB, Brensinger CM, Landis JR. A morphometric analysis of the posed smile. Clin Orthod Res. 1998;1(1):2-11.
- Samsonyanová L, Broukal Z. A systematic review of individual motivational factors in orthodontic treatment: facial attractiveness as the main motivational factor in orthodontic treatment. Int J Dent. Epub 2014 May 20. doi: 10.1155/2014/938274.
- Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972; 62(3): 296-309.
- MacLaughlin RP, Bennett JC. Evolution of treatment mechanics and contemporary appliance design in orthodontics: a 40-year perspective. Am J Orthod Dentofacial Orthop. 2015; 147(6):654-662.
- Pitts T, Brown D. The 14 Keys to Pitts Case Management and Active Early Concepts. Pitts Protocol. 2015; 1:8-15.
https://issuu.com/orthoclassic/docs/pitts_protocol_issue_1. Accessed October 12, 2015. - Pitts T, Brown D. Active early Principles. Pitts Protocol. 2015;2: 8-14. https://issuu.com/orthoclassic/docs/pitts_protocol_issue_2. Accessed October 12, 2015.
- Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001; 120(2): 98-111.
- Pitts, T. Begin with the end in mind and finish with beauty. EJCO. 2014;2(2):39-46.
- Peng L, Cooke MS. Fifteen year reproducibility of natural head posture: a longitudinal study. Am J Orthod Dentofacial Orthop. 1999;116 (1):82-85.
- Brandão RC, Brandão LB. Finishing procedures in orthodontics: dental dimensions and proportions (microesthetics). Dental Press J Orthod. 2013;18(5):147-174.
- Archambault A, Major TW, Carey JP, Heo G, Badawi H, Major PW. A comparison of torque expression between stainless steel, titanium molybdenum alloy, and copper nickel titanium wires in metallic self-ligating brackets. Angle Orthod. 2010;80(5): 884-889.
- Pitts T, Brown D. Flipping and Flocking. Pitts Protocol. 2015;3: 6-18.
- Johnson E. Selecting custom torque prescriptions for the straight-wire appliance. Am J Orthod Dentofacial Orthop. 2013;143(4):S161-167.
- Badawi HM, Toogood RW, Carey JP, Heo G, Major PW. Torque expression in self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008; 133(5): 721-728.
- Meling TR, Odegaard J, Meling EO. On mechanical properties of square and rectangular stainless steel wires tested in torsion. Am J Orthod Dentofacial Orthop. 1977;111(3):310-320.
- Dalstra M, Eriksen H, Bergamini C, Melsen B. Actual versus theoretical torsion play in conventional and self-ligating bracket systems. J Orthod. 2015;42(2):103-113.
- Fleming PS, Lee RT, Marinho V, Johal A. Comparison of maxillary arch dimensional changes with passive and active self-ligation and conventional brackets in the permanent dentition: a multicenter, randomized controlled trial. Am J Orthod Dentofacial Orthop. 2013; 144(2): 185 -193.
- Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2): 98-111.
- Sarver DM. Principles of cosmetic dentistry in orthodontics: Part 1. Shape and proportionality of anterior teeth. Am J Orthod Dentofacial Orthop. 2004;126(6):749 – 753.
