CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to identify some orofacial characteristics that may necessitate myofunctional therapy and also describes exercises designed to facilitate myofunctional therapy.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify some characteristics of the orofacial area that may indicate a need to co-treat with a myofunctional therapist.
- Identify some causes and therapy targeting tongue thrust.
- Recognize some causes and therapy for improper oral resting posture of the tongue.
- Recognize the connection between myofacial functioning and OSA.
- Recognize the co-treatment goals of the myofunctional therapist.

Nicole Cavalea, MS, discusses co-treatment goals of myofunctional therapy

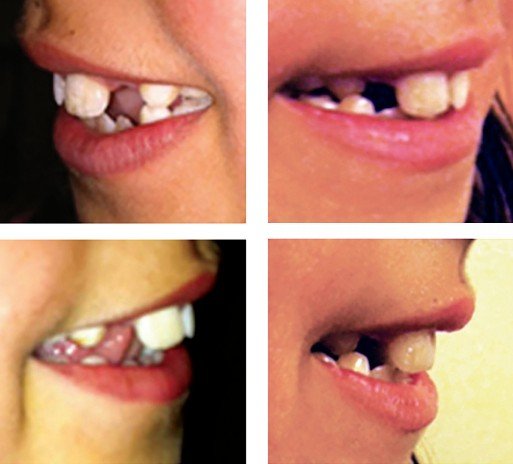
Orthodontists and pediatric dentists are often the first professionals to identify a patient’s abnormal patterning of the mouth and tongue, as these abnormalities interfere with the structural integrity of orthodontic treatment. A visual assessment of the following characteristics can indicate the need to co-treat with an orofacial myofunctional therapist:
- forward tongue protrusion during resting, speech, and/or swallow
- open mouth posture
- weak lip seal
- postural changes to face
- open bite
- distorted speech
- jaw instability
- dark eye circles
- long face
- high, narrow palate
When a patient presents with a tongue thrust, the clinician will observe resting the tongue against the teeth, swallowing with the tongue pushing against the teeth, and making sounds (meant for placement on the alveolar palate) with tongue pressure against the teeth. Having a tongue thrust will apply pounds of pressure on the anterior teeth daily. This postural and functional imbalance may cause serious dental problems and greatly interfere with the efficiency of orthodontic treatment. If incorrect muscle patterning or swallowing has created a malocclusion, learning proper techniques to correct these imbalances may prevent further damage as special orthodontic appliances or braces will be needed to reposition dental problems that have already occurred. If atypical swallowing is not corrected early, it can cause alterations in the development of the stomatognathic apparatus. Furthermore, the improper function of the tongue, in conjunction with dental malocclusion, will often lead to jaw instability, thus causing pain and headaches for the patient. For these reasons, myofunctional therapy is a useful adjunct treatment to orthodontics in subjects with myofunctional dysfunction.7

Two important factors in the correction of tongue-thrust swallowing are 1) growth and 2) orthodontic treatment to place the teeth in their proper positions and thus simplify proper tongue placement. However, growth and orthodontic treatment alone will not correct tongue-thrust swallowing. In correction therapy, the 22 muscles that are used in normal swallowing should be re-educated to eliminate the tongue-thrust swallowing habit in order for the patient to be able to unconsciously swallow in the correct manner.8
Therapy targeting a tongue thrust is aimed to strengthen, coordinate, and retrain the muscles involved in swallowing, resting posture, and speech. First, an assessment is used to determine the nature of the postural imbalances that are present and how they affect craniofacial development. Next, the patient is given a set of exercises to activate and strengthen the weakened muscles used incorrectly during swallow and involved in postural imbalances. Proper placement and precision are taught in regard to the function of swallowing. When swallowing correctly, the patient is instructed to voluntarily place the tongue against the roof of the mouth while bringing lips together and creating a suction to swallow. The patient is then taught correct resting posture and speech.
Lip exercises to strengthen the lip seal and to habituate a closed-mouth posture are elicited. The nature of therapy is to correct habitual use of the tongue while working on strengthening and patterning of the soft tissue involved. Treatment will last anywhere from 4 to 6 months with exercises and practice daily.
 Improper oral resting posture of the tongue will have a negative influence of the oral cavity and airway. The anatomy of the upper airway in turn guides the growth and development of the nasomaxillary complex, mandible, temporomandibular joint, and ultimately, the occlusion of the teeth; thus, malocclusion and facial dysmorphism may be the result of compensation for a narrowed airway.5 Short lingual frenulum is a known factor in altering orofacial growth particularly impacting development of the maxilla due to the low placement of the tongue. It leads to the abnormal development of a high and narrow hard palate, and secondarily, mouth-breathing during sleep.4
Improper oral resting posture of the tongue will have a negative influence of the oral cavity and airway. The anatomy of the upper airway in turn guides the growth and development of the nasomaxillary complex, mandible, temporomandibular joint, and ultimately, the occlusion of the teeth; thus, malocclusion and facial dysmorphism may be the result of compensation for a narrowed airway.5 Short lingual frenulum is a known factor in altering orofacial growth particularly impacting development of the maxilla due to the low placement of the tongue. It leads to the abnormal development of a high and narrow hard palate, and secondarily, mouth-breathing during sleep.4
Obstructive sleep apnea (OSA) has become increasingly recognized as a notable health concern in children, given its consequences on behavior, function, and quality of life. Statistically, 40% of children who suffer from sleep-disordered breathing (SDB) develop ADD, ADHD, and/or a learning disability. Additionally, children are diagnosed with SDB in the first 5 years of life, and left untreated, they are 60% more likely to require special needs education by age 8.1
Most children with OSA have difficulty breathing through the nose. Allergic rhinitis is the most commonly cited disease, followed by hypertrophy of the tonsils and adenoids.1 Orofacial and pharyngeal muscles are involved in important functions including breathing, with the vital role of maintaining airflow. Any upper airway (UA) obstruction may induce changes in neuromuscular function in order to ensure the passage of air. The most common consequence of UA obstruction is mouth breathing, a functional adaptation that may affect craniofacial growth and development during childhood. Another possible consequence is obstructive sleep apnea (OSA).1
Myofunctional treatment is aimed at correcting abnormal breathing patterns and muscular dysfunction that may impair upper airway patency.1 Adenotonsillectomy (T&A) and palatal expansion have established roles in the treatment of OSA after demonstrating considerable improvement related to adenoid or tonsillar hypertrophy, maxillary or mandibular deficiency, and orthodontic or craniofacial abnormalities. However, the implementation of other modalities such as myofacial re-education also plays a crucial role in the optimization of sleep-disordered breathing, as maladapted orofacial functions may be irreversible or present insufficient improvement even when their original cause is eliminated.1 If nasal breathing is not restored, despite short-term improvements after adenotonsillectomy, continued use of the oral breathing route may be associated with abnormal impacts on airway growth and possibly blunted neuromuscular responsiveness of airway tissues, both of which may predispose to the eventual return of upper airway collapse in later childhood or in the full blown syndrome of OSA in adulthood.2
Co-treatment goals of the myofunctional therapist follow: First, determine the nature of the postural imbalances that are present and how they affect craniofacial development and functional ability. Next, correct muscular imbalances of the lips, tongue, and jaw through exercises meant to re-pattern, coordinate, and strengthen these areas involved. Children with OSA were found to have relative impairments in orofacial functions and lesser muscular coordination.1 The therapist activates and strengthens the oral facial muscles of mastication to support the mandible and the genioglossus at night.
Approximately 30% of OSA patients have poor genioglossus muscle responsiveness to airway narrowing during sleep.6 The tongue muscles are trained to achieve palatal tongue rest position (aiding in correct tongue posture during rest, speech, and swallow). Proper placement and precision are taught in regard to the function of swallowing. When swallowing correctly, the patients are instructed to voluntarily place their tongue against the roof of the mouth while bringing lips together and creating a suction to swallow. Finally, correct nasal breathing, along with a proper resting oral posture, is established. Achieving proper nasal breathing will result in improving lung volume, increasing nitric oxide through the body, improvement in sleep, and the reduction of allergies and illnesses.
To restore efficiency in breathing, first, the myofunctional therapist will educate patients on proper nasal/diaphragmatic breathing. Once coherence is established, they will learn a series of exercises that focus on the biomechanical and biochemical aspects of breathing. Biochemically, patients are instructed to breathe in a way that creates a desire for air (such as narrow, light breaths). This technique will decrease their sensitivity for CO2, therefore creating a larger threshold to eliminate sleep disturbances. Biomechanically, patients are instructed on ways to practice techniques that maximize breathing skills. For example, they learn deep, slow breathing through the nose where the air effectively expands the diaphragm. Treatment will last anywhere from 4 to 6 months, with exercises and practice daily.
Conclusion
Research indicates that successful treatment of functional postural abnormalities depends on the collaboration of multidisciplinary teams. Comprehensive management requires an integrated effort of the sleep physician, otolaryngologist, allergist, orthodontist, pediatric dentist, and myofunctional therapist.
Treatment of myofunctional therapy can be carried out in office or through telepractice (i.e., telemedicine or telehealth). Both modalities provide effective measures of intake, assessment, collaboration, and treatment for the patient.
Read Dr. Daniel Klauer’s article on the key role of orofacial myofunctional therapy in orthodontic treatment here: https://orthopracticeus.com/clinical/myofunctional-therapy-plays-a-key-role-in-the-orthodontic-practice/
Author Info
 Nicole Cavalea, MS, is the founder of Strategies for Success, a speech-language pathology practice and myofunctional therapy clinic. She has worked in the field of communication disorders for 19 years. She received her MS degree in Speech and Language Pathology from San Jose State University. Cavalea has extensive expertise working with children of all ages in the assessment, treatment, and management of speech and language disorders, auditory processing delays, and myofunctional disorders. After incorporating myofunctional techniques into her practice, she began noticing her patients improving with quicker and more precise results, leading her to further her training in myofunctional disorders and treatment, and attending multiple intensive training courses from the Academy of Orofacial Myofunctional Therapy. Recent studies include an advanced course on breathing re-education, focusing on restoring adequate breathing in sleep apnea patients. Recently, Cavalea has expanded her practice nationwide through telepractice, and values and enjoys collaboration and cotreatment with multidisciplinary teams across the country. Nicole Cavalea can be reached at ncavalea@gmail.com.
Nicole Cavalea, MS, is the founder of Strategies for Success, a speech-language pathology practice and myofunctional therapy clinic. She has worked in the field of communication disorders for 19 years. She received her MS degree in Speech and Language Pathology from San Jose State University. Cavalea has extensive expertise working with children of all ages in the assessment, treatment, and management of speech and language disorders, auditory processing delays, and myofunctional disorders. After incorporating myofunctional techniques into her practice, she began noticing her patients improving with quicker and more precise results, leading her to further her training in myofunctional disorders and treatment, and attending multiple intensive training courses from the Academy of Orofacial Myofunctional Therapy. Recent studies include an advanced course on breathing re-education, focusing on restoring adequate breathing in sleep apnea patients. Recently, Cavalea has expanded her practice nationwide through telepractice, and values and enjoys collaboration and cotreatment with multidisciplinary teams across the country. Nicole Cavalea can be reached at ncavalea@gmail.com.
References
- De Felicio CM, da Silva Dias FV, Folha GA, et al. Orofacial motor functions in pediatric obstructive sleep apnea and implications for myofunctional therapy. Int J Pediatr Otorhinolaryngol. 2016;90:5-11.
- Guilleminault C, Sullivan SS. Towards restoration of continuous nasal breathing as the ultimate treatment goal in pediatric obstructive sleep apnea. Enliven: Pediatr Neonatol Biol. 2014;1(1):001.
- Huang YS, Guilleminault C. Pediatric obstructive sleep apnea and the critical role of oral-facial growth: Front Neurol. 2012;3:184.
- Huang YS, Quo S, Berkowski A, Guilleminault C. Short lingual frenulum and obstructive sleep apnea in children. Int J of Pediatr Res. 2015;1:1.
- Moeller JL, Paskay LC, Gelb ML. Myofunctional therapy: a novel treatment of pediatric sleep-disordered breathing. Sleep Med Clin. 2014;9:235-243.
- Osman AM, Carter JC, Carberry JC, Eckert DJ. Obstructive sleep apnea: current perspectives. Nat Sci Sleep. 2018;10:21-34
- Saccomanno S, Antonini G, D’Altari L, et al. Patients treated with orthodontic-myofunctional therapeutic protocol. Eur J Paediatr Dent. 2012;13(3):241-243.
- Straub WJ. Malfunction of the tongue. Am J Orthod. 1962;48(7):486-503.
