CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to introduce a methodical treatment approach aimed at simply correcting Class III malocclusions without patients’ cooperation or orthognathic surgery.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize the basic concepts behind this technique.
- Identify some of the biomechanics of the intrusive V-bends.
- Realize the reasons behind the various stages of the technique.
- Realize when this technique should be used or when other treatment options should be implemented.

Dr. Suhail A. Khouri discusses a method of delivering light and consistent forces over a long range of effective intrusive tooth movement
Abstract
Orthodontic correction of Class III malocclusions in growing adolescent and adult patients has long challenged orthodontists due to the extreme difficulty in disengaging the locked-out maxillary teeth without surgery. Currently available treatment modalities include various functional appliances, maxillary protraction and cervical headgears, and reversed twin blocks1,2 for growing prepubertal patients. Although these approaches are successful for this group of patients, nevertheless, such clinical triumphs depend totally on patient compliance, and they have high genetically determined potential for relapse. That is why establishing normal overjet in Class III patients is often onerous with orthodontic therapy alone. On the other hand, orthognathic surgical treatment offers dental, skeletal, and esthetic improvement in deep bite skeletal Class III patients; however, the trauma, high cost, and possibility of growth-related relapse of this approach discourages many patients and their parents from accepting it.
The advent of superelastic wires and the ability of Bendistal Pliers (DynaFlex®) to activate them with permanent V-bends, enhanced by the composite build-ups’ bite raisers, evolves into a new treatment protocol that shows efficiency and effectiveness in incisor intrusion and the correction of deep overbite patients.3 Utilizing the same concept to intrude and disengage the locked-out maxillary incisor teeth in Class III patients demonstrated efficiency in the retraction of mandibular incisors into available or created spaces and correction of this malocclusion. This article introduces this methodical treatment approach aimed at simply correcting Class III malocclusions without patients’ cooperation or ortho-gnathic surgery and presents patients who have been successfully treated with this V-bend technique.
This article introduces this methodical treatment approach aimed at simply correcting Class III malocclusions without patients’ cooperation or orthognathic surgery …
Concept of the technique
The primary objective in correcting Class III malocclusions is restoring the anterior overjet. Since there was no effective standard clinical method to free the locked-out maxillary teeth, orthognathic surgery became the clinician’s only choice to elicit the jump in adult patients. Once this difficult task had occurred, orthodontists could routinely perform all remaining tooth movements.
This technique aims primarily at disengaging maxillary and mandibular incisors nonsurgically by intruding them, with the help of bite-raising composite build-ups.
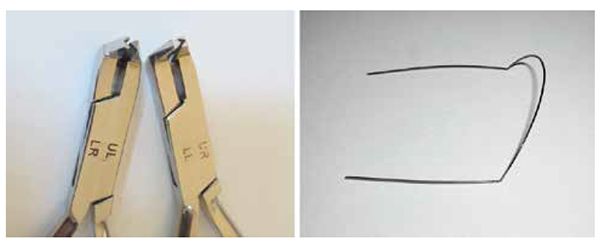
Following bonding of both arches and initial alignment, intrusion of maxillary and mandibular incisors is started by placing sharp and permanent V-bends on the superelastic archwires with the Bendistal Pliers (Figure 1). These V-bends3,4 on round and rectangular superelastic archwires have demonstrated effectiveness in activating them to deliver light and consistent intrusive forces over a long range of activation, which intrudes anterior segments and efficaciously opens deep overbites.3-5 Applying the intrusion mechanics of the V-bends6-8 on superelastic wires to correct most Class III malocclusions has unlocked and disengaged maxillary incisors and allowed the retraction of mandibular incisors, thus restoring the normal overjet.
Although this technique functions well in dental and moderate skeletal Class III malocclusions, complicated cases with skeletal bilateral crossbites and/or skeletal open bites, and excessive mandibular growth tendency will eventually need orthognathic surgery.
Technique description
1. Alignment stage
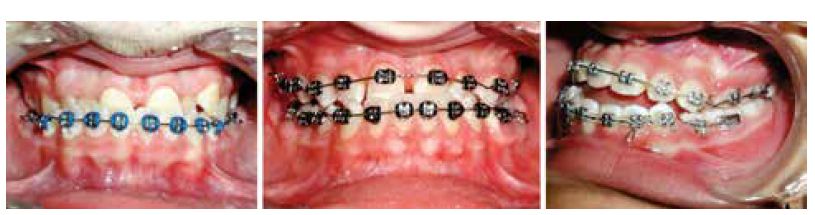
Since the mandibular incisors typically block out the maxillary incisors, mandibular teeth are bonded first, and a 0.016″ round NiTi archwire is placed for initial alignment (Figure 2A). If there is an adequate underjet space or bite-free areas on labial surfaces of the maxillary incisors, clinicians can bond the maxillary teeth and start intrusion mechanics in both arches simultaneously. Bite-opening composite build-ups on mandibular posterior teeth will open the occlusion enough and allow maxillary teeth bonding and enhance incisor disengagement to shorten treatment time (Figures 2B and 2C).
To intrude the incisors, place the V-bends behind canine areas in both archwires with the tips of V-bends always directed occlusally on the NiTi archwires. The V points down in the maxillary archwire and points up in the mandibular archwire. If more intrusion is required, in deep-bite Class III malocclusions, the initial archwires should graduate to 0.016″ x 0.022″ NiTi archwires to increase the light intrusive force level. Further bite opening, if needed in the case of severe deep bite of an individual tooth, may be achieved by tucking the elastic wire underneath the maxillary incisor bracket tie wings and on top of the mandibular incisor bracket tie wings (Figure 4A). Once intrusion and composite build-ups disengage incisors, as seen in Figure 2C, the clinician can retract mandibular incisors.
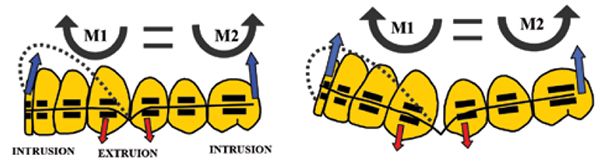
Biomechanics of the intrusive V-bends: To obtain maximal central and lateral incisor intrusion, V-bends work most efficiently when located behind the canines. V-bends deliver an apically directed intrusive force at the bracket sites of the farthest teeth from the V-bends — namely, the central incisors and the terminal molars. These forces act at the bracket site buccal to the center of resistance and cause rotation of the incisors in line with their long axis, while simultaneously intruding them. This creates a clockwise moment (M1) that intrudes the incisors anterior to the V-bend and an equal and opposite anticlockwise moment (M2), that intrudes the terminal molar posterior to the V-bend. As the force system of the V-bend establishes equilibrium, the incisors and molars will intrude, while the canines and first premolars extrude. The collective effects of this force system results in efficient bite opening8 (Figure 3).

2. Intrusion and disengagement stage
Anterior teeth intrusion and disengagement is the primary objective of this technique. This crucial stage of treatment begins immediately after mandibular arch alignment by placing intrusive V-bends behind the mandibular canines on the aligning .016″ NiTi archwire to start mandibular incisor intrusion. Once mandibular incisors intrude halfway and expose part of the labial surfaces of the maxillary incisor crowns, they can be bonded, the aligning archwire is tied in, and similar V-bends can be placed on it (Figures 2A-2B). Clinicians can combine the intrusion mechanics on both archwires with composite build-ups9-11 on mandibular molars to speed up anterior disengagement and start mandibular incisor retraction. Later on, clinician can graduate archwires to intrusive .016″ x .022″ NiTi to increase force level and accelerate treatment (Figure 2C). 3. Mandibular incisors retraction stage
Clinicians should decide during treatment planning how to provide spaces for mandibular incisor retraction. Several options exist for creating mandibular dental spaces — i.e., using residual spaces if any, and creating spaces with interproximal enamel reduction and/or mandibular first premolar extraction. Retraction starts as soon as full disengagement occurs by using a power chain with the mandibular V-bends in place. The V-bends’ intrusive force acting on mandibular incisors should continue during their retraction, not only to maintain incisor disengagement, but also more importantly, to provide the moment necessary to translate them and prevent their uncontrolled tipping, according to Burstone’s segmented arch technique. Once mandibular incisor retraction into the created spaces is completed, and a positive overjet occurs, the intrusion process is discontinued and followed by placing the same size rectangular archwires without V-bends in both arches. 4. Incisors bite jump and finishing stage
Once the mandibular spaces close and proper overjet occurs, the finishing stage can commence. The incisal jump achieves a customary overjet following completion of the retraction of the incisors into the created spaces. Clinicians can start the detailed finishing stage by establishing normal overbite, overjet, and closure of the posterior open bite affected by the V-bends’ intrusion mechanics. Posterior bite-closing inter-maxillary elastics are used to achieve proper teeth intercuspation. Rectangular 0.016″ x 0.022″ NiTi followed by stainless steel archwires without bends are used as the finishing wires to correct the final root positions (Figure 4C). Any other detailed tooth movements to achieve standard molar/cuspid relations and overbite/overjet may be carried out in a routine manner.
Patient 1

Patient 2
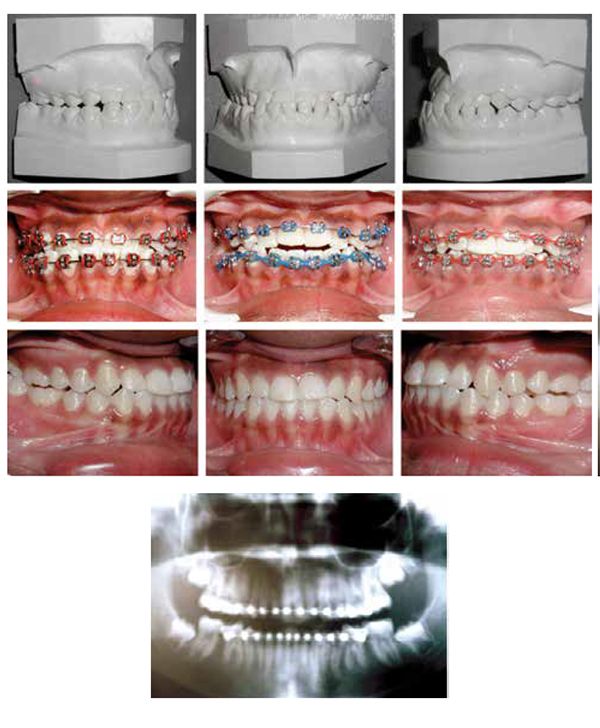
Patient 3

Patient 4

Patient 5

Patient 6

Discussion
Placing sharp and permanent V-bends on superelastic wires to activate them and deliver light and consistent forces over a long range of effective intrusive tooth movement comprises the essence of this technique. These bends are not to be placed on superelastic wires without the unique bending ability of Bendistal Pliers. Although V-bend mechanics, elastic properties of NiTi wires, and the bite-raising composite may not be new to orthodontists, orchestrating and employing these elements to correct such difficult orthodontic problems are a new approach. Combining such elements has evolved into developing this therapeutic method as a new simple and clinically applicable technique. It proved its efficiency in nonsurgical correction of Class III malocclusions, and I have used it throughout my entire 35-years of orthodontic practice. The bite-raising composite build-ups were used to enhance anterior teeth disclusion in deep bite cases to shorten treatment time.
The patients presented have varying degrees of difficult Class III malocclusions that were successfully treated by this alternative therapy without using any removable functional appliances, headgear, or surgery. This patient therapy illustrated the possibility of using anterior intrusions alone, or combined with the bite raiser composite-build-ups, to simplify and shorten treatment time necessary for disengaging the blocked out anterior teeth, leading to Class III non-surgical complete correction.
Patients with severe Class III mal-occlusion and skeletal deformities may require orthognathic surgery; patients and parents should be informed that orthodontic treatment alone could not achieve the needed therapy. To avoid surgery for moderate Class III malocclusions, patients should be informed that mandibular first premolar extractions might be needed to provide spaces into which mandibular incisors will be retracted. They should also know that esthetic improvement in facial soft tissue might not match the improvement that orthognathic surgery often gives.
Acknowledgment
With great appreciation, the author thanks Dr. Larry White for his outstanding help in editing this article
References
- Westwood PV, McNamara JA Jr., Baccetti T, Franchi L, Sarver DM. Long-term effects of Class III treatment with rapid maxillary expansion and facemask therapy followed by fixed appliances. Am J Orthod Dentofacial Orthop. 2003;123(3):306-320.
- Shastri D, Nagar A, Tandon P. Treatment of pseudo-Class III malocclusion with a modified reverse twin block and fixed appli-
ances. J Clin Orthod. 2015;49(7):470-476. - Khouri SA. Correcting deep bites with V-bends and superelastic wires. World J. Orthod. 2006;7(2):213-217.
- Khouri SA. The bendistal pliers: a solution for distal end bending of superelastic wires. Am J Orthod Dentofacial Orthop. 1998;114(6):675-676.
- Khouri SA. Using the bendistal pliers for the correction of common orthodontic problems. World J. Orthod. 2002;3(2):172-174.
- Tran PH. The three-tooth problem: a facial plane force system delivered by a gabled archwire segment. [Master’s thesis] St. Louis, Mo.: Saint Louis University; 2004.
- Lopez I, Goldberg J, Burstone CJ. Bending characteristics of nitinol wire. Am J Orthod. 1979;75(5):569-575.
- Burstone CR. Deep overbite correction by intrusion. Am J. Orthod. 1977;72(1):1-22.
- Nanda R. Correction of deep overbite in adults. Dent Clin North Am. 1997;41(1): 67-87.
- Tzatzakis V. A new clinical approach for the treatment of anterior crossbites. World J of Orthod. 2008;9(4):355-365.
- Tzatzakis, V, Gidarakou I. Correcting of anterior crossbite using occlusal build-ups. J Clin Orthod. 2007;4(7):393-397.
