CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to discuss the benefits and several common uses of the vertical slot.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
· Identify vertical slot ligation.
· Realize the variety of uses of the T-Pin.
· Recognize the function of rotation springs when placed in the vertical slots.
· Realize the function of torquing auxiliaries.
· Identify power arms and how, when inserted into the slot, they exert a force closer to the center of resistance of a tooth

Dr. Mark W. McDonough reviews several common uses of the vertical slot
 Are you interested in increased treatment efficiency? Do you like to treat challenging cases? Would you like a better bracket at no additional cost? If you answered “yes” to any of these questions, you should have a vertical slot in your bracket. The vertical slot or V-slot can be traced back to Dr. Raymond Begg in 19281 (Figure 1). As our profession progresses, we often lose sight of how we got here and disregard the past as we focus on the future. There have been relatively few articles published recently on the vertical slot, and this may be the reason it has fallen out of favor with the current generation of orthodontists.2 We all have preferences and often discuss the benefits of .018 versus .022 slots, standard versus self-ligating, Roth versus MBT prescription. However, the one constant should be that the bracket has a vertical slot. This article reviews several common uses of the vertical slot and will make the case that 100% of fixed appliances should have a vertical slot.
Are you interested in increased treatment efficiency? Do you like to treat challenging cases? Would you like a better bracket at no additional cost? If you answered “yes” to any of these questions, you should have a vertical slot in your bracket. The vertical slot or V-slot can be traced back to Dr. Raymond Begg in 19281 (Figure 1). As our profession progresses, we often lose sight of how we got here and disregard the past as we focus on the future. There have been relatively few articles published recently on the vertical slot, and this may be the reason it has fallen out of favor with the current generation of orthodontists.2 We all have preferences and often discuss the benefits of .018 versus .022 slots, standard versus self-ligating, Roth versus MBT prescription. However, the one constant should be that the bracket has a vertical slot. This article reviews several common uses of the vertical slot and will make the case that 100% of fixed appliances should have a vertical slot.
If you review most bracket manufacturers’ websites, you will note that about 25% of braces manufactured today are offered with a vertical slot. Most vertical slots are .018 X .018, and TP Orthodontics has the widest variety of auxiliaries for the vertical slot. Many orthodontists indicate that they do not have a vertical slot due to the increased profile of the bracket, which will cause interference on lower incisors, and their patients do not like thicker brackets. This is a common misconception. Figure 2 reviews the Mini Diamond® Twin bracket from Ormco (Orange, California), which I use, and shows no significant difference in the base thickness of a lower incisor bracket with a vertical slot on the left (0.58) or without a vertical slot on the right (.060). This is due to improvements in manufacturing, which allow for a lower profile vertical slot bracket. Most other manufacturers show similar findings.
In order to demonstrate why orthodontists need a vertical slot, the most common uses of the vertical slot will be reviewed. These cases represent the use of the vertical slot in our practice from most frequent to less frequent. This is not meant to be an exhaustive review of vertical slots, but a practical review of common situations we all face every day. The article will conclude with a difficult transposition patient who could not have been treated as efficiently or with fewer side effects without a vertical slot.

 Vertical slot ligation
Vertical slot ligation
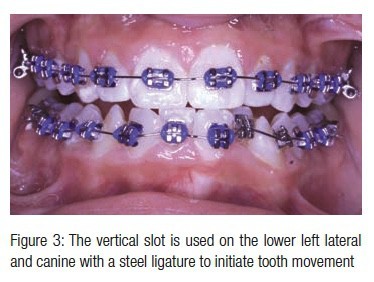
The most common use of the vertical slot is to allow insertion of ligature wires through the vertical slot, which is tied to the archwire for severely displaced teeth at the initial bonding (Figure 3). We all acknowledge that low friction and wide inter-bracket distance are desirable for efficient tooth movement. When forces are directed through the center of rotation, tooth movement is enhanced. Loosely tying a displaced or ectopic tooth through a vertical slot accomplishes all of these goals. It also decreases the force to the teeth involved, which increases patient comfort while increasing tooth movement by preventing excessive force to the periodontal ligament.
For the following visit, the steel ligature can be tightened, and gradually the tooth is brought in the arch. This avoids additional archwire changes, which saves chair time and overhead expense. Figure 4 shows exactly 5 months later, and the bite is open, and the arches are aligned.
 Without a vertical slot, the displaced teeth would need to be ligated to the two tie wings closest to the archwire, which would exert an undesirable rotational force as the tooth moves toward the archwire. Later in treatment, this undesired rotation would have to be addressed, which increases treatment time. Also, with this method of tying only two tie wings, there is the chance the ligature loosens and falls off, which further lengthens treatment time. When you tie through the vertical slot, there is no chance the ligature falls off.
Without a vertical slot, the displaced teeth would need to be ligated to the two tie wings closest to the archwire, which would exert an undesirable rotational force as the tooth moves toward the archwire. Later in treatment, this undesired rotation would have to be addressed, which increases treatment time. Also, with this method of tying only two tie wings, there is the chance the ligature loosens and falls off, which further lengthens treatment time. When you tie through the vertical slot, there is no chance the ligature falls off.
T-Pins
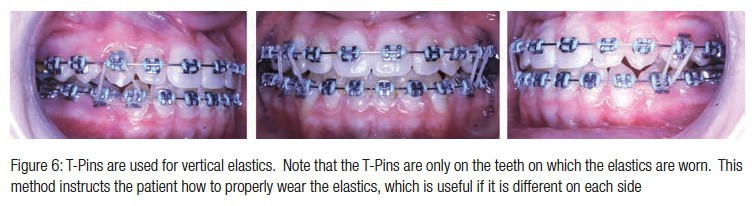
T-Pins (Figure 5) can be inserted through vertical slots for a variety of uses. The most common is as hooks for elastic bands. Unlike ball hooks that many brackets have permanently attached to the bracket, which irritate the patient throughout treatment, T-Pins can be added and removed as needed. Since they are at the base of the bracket, they protrude less than ball hooks and are more comfortable for the patient. They have the added benefit that they ensure that the patient is wearing the elastics as prescribed, since the T-Pins are only placed in the brackets as needed. An additional benefit is that as the elastics change from Class II elastics to triangle elastics or vertical elastics, it becomes readily apparent to patients how they should wear their elastics. This is especially useful when patients have different types of elastics on each side (Figure 6).


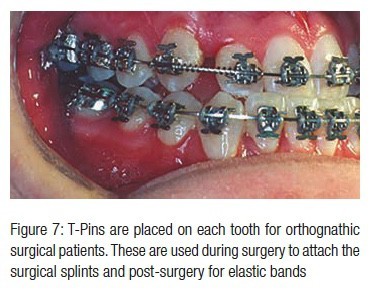
T-Pins are also an alternative for ball hooks crimped to the archwire for orthognathic surgical patients for the surgeon to use at the time of surgery to ligate the surgical splints (Figure 7). The T-Pins are easily inserted, have a lower profile than ball hooks, and are less expensive. Unlike ball hooks, they do not slide on the wire, and the surgeon will not introduce torque on the wire, which can cause unwanted postsurgical tooth movement. Some surgeons request ball hooks, but are unaware that T-Pins are an alternative.
Another use for T-Pins is to secure nitinol springs as shown in this indirect anchorage TAD-supported case for missing maxillary second premolars (Figure 8). The T-Pin is at the same height as the hook on the molar, and this keeps a more horizontal force for the nitinol spring and has the added benefit that the T-Pin can be bent buccally to prevent the nitinol spring from impinging on the gingiva.
Rotation springs
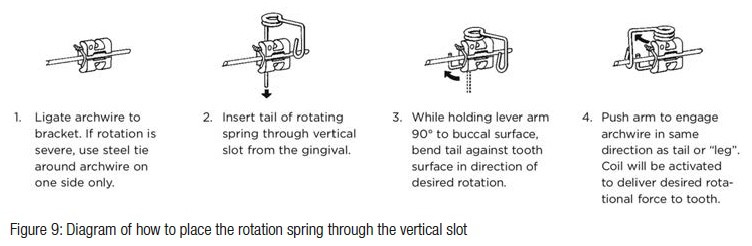
Rotation springs are placed in the vertical slots and are used to correct individual tooth rotations. These are easy to place (Figure 9) and provide more control than a superelastic wire since they are able to be used with larger stainless-steel wires. They are particularly useful if a patient breaks a bracket and a tooth rotates near the end of treatment when larger diameter wires are in place. Typically, the bracket is rebonded, and a smaller flexible wire is used to unrotate the tooth. At a later visit, the larger wire is replaced, and valuable treatment time was wasted due to the broken bracket. With a rotation spring, the need to step back in wire size is negated, and treatment time is not affected.


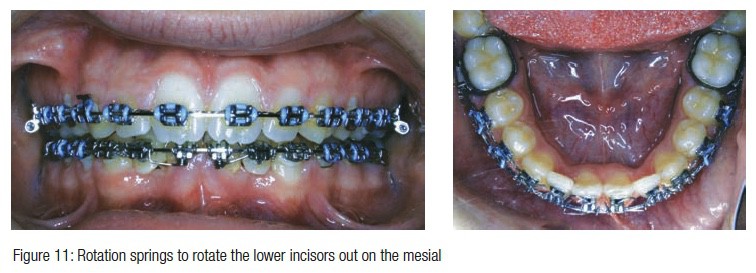
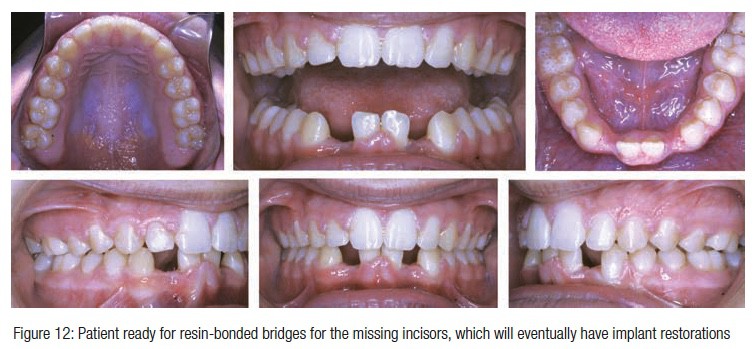
Another case where rotation springs proved useful is shown below when a patient was congenitally missing two lower incisors. The prosthodontist requested the incisors to be brought together so that implants could be used to restore the case, since implants with natural teeth on either side of the implant have a better restorative outcome than two implants next to each other. As the teeth were brought together, there was a mild rotation to the mesial. Correcting this with flexible wires would have been difficult, since pontics were attached to the 19 X 25 stainless steel wire and the case was near the end of treatment. The rotation springs aligned the teeth in only 6 weeks with no need to change the wire (Figures 10, 11, 12).
Torquing auxiliaries
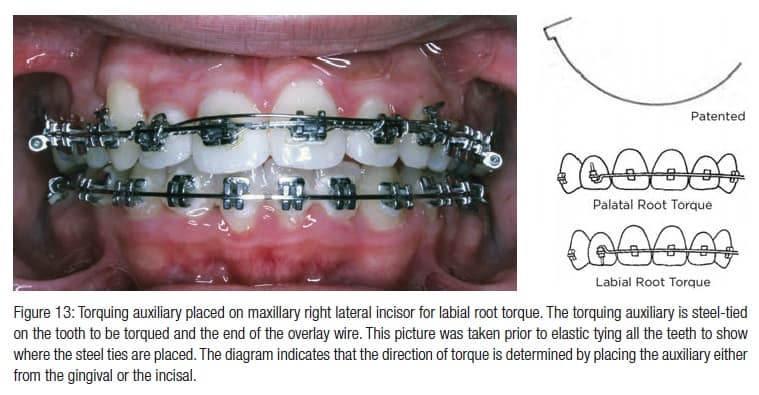
Adding labial or lingual root torque to a tooth is often the most difficult tooth movement to do because the force is generated in the slot of the bracket, which is .022 or .018 inches high. The archwire must exert the torquing moment over a very small distance, which is very inefficient. Fortunately, the Individual Root Torquing Auxiliary (Figure 13) from TP Orthodontics can exert either labial or lingual root torque by having a rectangular stainless-steel base arch, and it is inserted either from the incisal or gingival to exert the appropriate direction of torque. You can control the amount of torque by the selection of the appropriately sized rectangular wire. For example, if a 17 X 25 wire is used in a .022 bracket, there is .05 of play in the bracket. Each .01 of play allows ~4 degrees of rotation in the slot. If you multiply .05 by 4 degrees, this will allow for 20 degrees of torque. If the patient misses an appointment, no further torque is expressed. If you wanted only 12 degrees of torque, use a 19 X 25 base wire. TP recommends using round wires, but I do not feel this is wise, since unintended excessive torque can be expressed if the patient does not return at the appropriate time.
Power arms
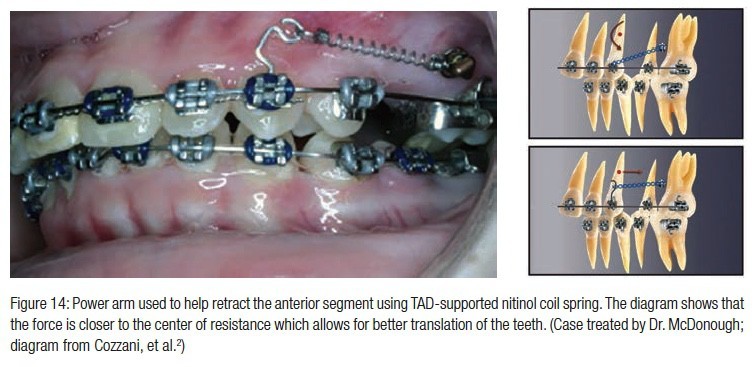
Power arms inserted into the vertical slot are used to exert a force closer to the center of resistance of a tooth. They come in a short and long size depending on the desired place you want to exert a force. This can be especially useful if a temporary anchorage device (TAD) is placed in order to retract an anterior segment using maximum anchorage (Figure 14). The diagram shows the unfavorable rotation of the anterior segment if the force is directed from the TAD to the canine. When a power arm is used, a more favorable bodily movement is possible without the unwanted rotation of the anterior segment.
Transposition patient utilizing vertical slot mechanics
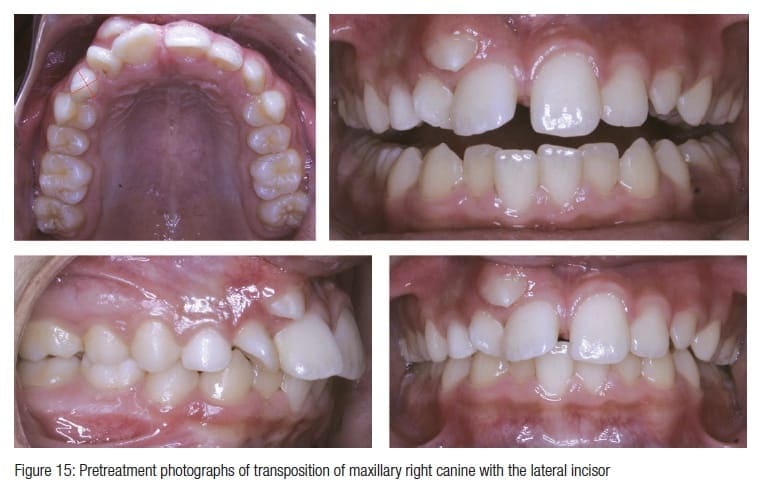
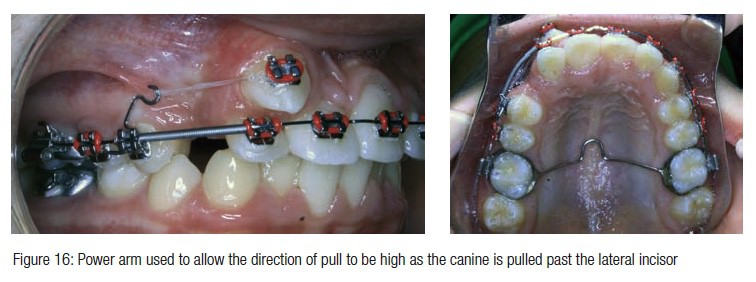
This 12-year-old presented with a transposition of the upper right canine between the lateral and central incisor (Figure 15). A transpalatal arch was used for anchorage, and a power arm was used to pull the tooth distal and keep it high in the buccal vestibule until it passed the root of the lateral incisor (Figure 16).
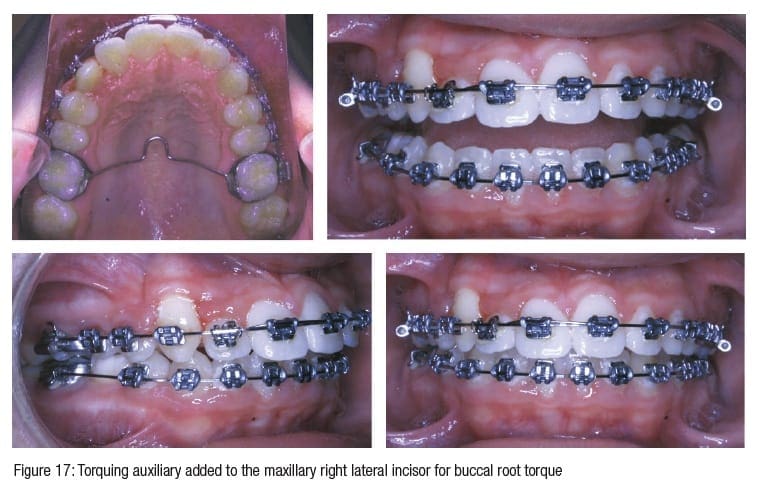
Once the canine was brought into the arch, a Torquing Auxiliary was added to the maxillary lateral incisor to add buccal root torque (Figure 17).
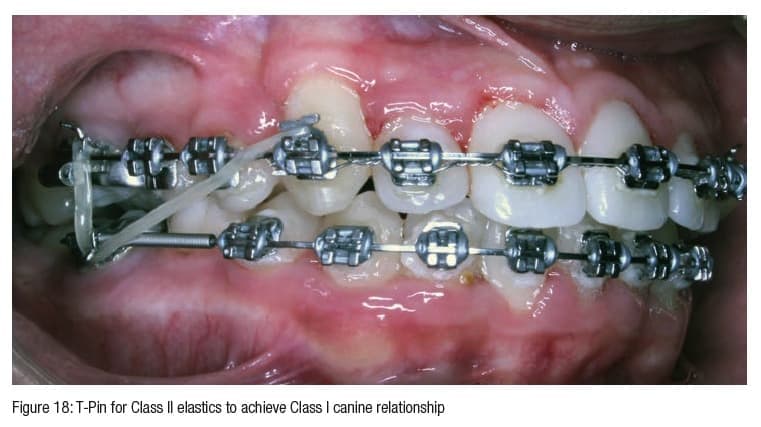
Toward the end of treatment, Class II check elastics were used to T-Pins in the maxillary canines to achieve Class I canine and lock in the molar (Figure 18).
The total treatment time up to this point is 18 months, and the patient is now in finishing. Without a vertical slot, this patient could not have had such efficient tooth movement in as short of time.
Conclusion
The vertical slot is the “swiss army knife” of fixed orthodontic treatment. It is used on just about every patient we treat to make the treatment more efficient while increasing patient comfort. The vertical slot is most useful on the most challenging cases, and there is no additional cost for brackets with a vertical slot. I can easily understand the advantages and disadvantages of many of the brackets produced today, but there is no reason all brackets used should not have a vertical slot. It is always available and useful in so many ways, and it is free.
Besides his CE on vertical slot brackets, Dr. McDonough has also written a CE about treatment options for space closure of congenitally missing mandibular premolars. Read it here.
https://orthopracticeus.com/ce-articles/congenitally-missing-mandibular-premolars-treatment-options-space-closure
Author Info
 Mark W. McDonough, DMD, is an orthodontist who has been practicing in Pennington, New Jersey, since 1994. He earned his dental degree from the University of Pennsylvania, completed a General Practice Residency at Lenox Hill Hospital, New York, New York, and his Certificate in Orthodontics from Albert Einstein Medical Center in Philadelphia, Pennsylvania. He has also been a part-time clinical instructor at Albert Einstein Medical Center in Philadelphia since 1995. He is a Diplomate of the American Board of Orthodontics and past President of The Greater Philadelphia Society of Orthodontics and the Mercer Dental Society.
Mark W. McDonough, DMD, is an orthodontist who has been practicing in Pennington, New Jersey, since 1994. He earned his dental degree from the University of Pennsylvania, completed a General Practice Residency at Lenox Hill Hospital, New York, New York, and his Certificate in Orthodontics from Albert Einstein Medical Center in Philadelphia, Pennsylvania. He has also been a part-time clinical instructor at Albert Einstein Medical Center in Philadelphia since 1995. He is a Diplomate of the American Board of Orthodontics and past President of The Greater Philadelphia Society of Orthodontics and the Mercer Dental Society.
Disclosure: Dr. McDonough is in no way affiliated with any company, nor is he a paid speaker for any company mentioned in this article.
References
- Kesling, PC. Begg theory and technique: Past, present and future, In: Johnston LE, ed. New Vistas in Orthodontics. Philadelphia, PA: Lea and Febiger; 1985.
- Cozzana M, Mazzotta L, Bowman SJ, Rinchuse DJ. Use of the Vertical Slot in Orthodontic Brackets, J. Clin. Orthod. 2015;49(9):574-581.
