Drs. Barry Raphael, Mark A. Cruz, Richard D. Roblee, and Ellen Crean-Binion discuss how airway problems affect structure, function, and behavior, and leads to unintended consequences.
Drs. Barry D. Raphael, Mark A. Cruz, Richard D. Roblee, and Ellen Crean-Binion discuss how structure, function, and behavior affect airflow
The wrong question
The amount of time orthodontists have wasted polarizing around issues such as extraction versus nonextraction, one-phase versus two-phase, and now around the issue of “airway orthodontics” attests to an overall lack of understanding of the bigger picture of a patient’s health. It’s like arguing over whether light is a particle or a wave.
The duality around airway that is causing so much consternation is whether the problem is 1) obstructive sleep apnea — a condition that causes momentary and repeated cessation of breathing throughout the night, or 2) airway flow limitation leading to sleep fragmentation, in which narrowing of the airway anywhere from the tip of the nose to the bottom of the throat makes it harder to breathe day or night.
Nobel-winning biochemist Albert Szent-Gyorgi said, “Science is built on the premise that nature answers intelligent questions intelligently; so if no answer exists, there must be something wrong with the question.”
So let’s take a look at the question surrounding airway orthodontics, and how changing our approach may lead us to some useful clinical guidelines.
Many orthodontic thought leaders, including the American Association of Orthodontists, frame the question of airway in terms of the teeth and malocclusion. They ask: Does sleep apnea cause malocclusion? Does malocclusion cause sleep apnea? Can orthodontics cause or cure sleep apnea?
Since the evidence is equivocal, many have stopped their questioning there and dismissed the issue of airway altogether. But perhaps there is something wrong with the questions.
Reframing the question
The question does not directly involve the teeth or malocclusion at all. And it only tangentially involves sleep. The question involves breathing and only breathing. The operant question is: What is a healthy, functioning airway? And what perturbs it?
Breathing, as we all know, is a biological imperative. Moment to moment, it is the most important behavior we do since it feeds every cell in our body with the oxygen it needs and helps to regulate blood pH, which controls the delivery of oxygen to the cells.
An optimal breathing pattern is done through the nose, where the air is conditioned before entering the lungs, powered by the diaphragm so as to fill the entire lung with little effort, and at just the right rate and volume, to get just what the body needs. Breathing should be easy, silent, and through the nose most of the time.1,18 These optimal behaviors, or competencies, have developed through evolution (or by creation, if you will) to allow us to survive.
If our breathing suddenly stops, we can’t go for more than a few seconds before our brains go into survival mode and activate the sympathetic nervous system. The hypothalamic-pituitary-adrenal (HPA) axis is extremely sensitive to blood oxygenation and will react immediately to protect the body in any way possible if breathing falters.2
Behaviors that are adopted by the body to protect or restore oxygen levels are necessary for our survival. If someone blocks your nose and mouth, for instance, you will immediately go into fight/flight/fix mode to change that condition. The same thing happens at night if the airway narrows. The response is immediate and sometimes extreme. In obstructive sleep apnea, there is a delayed response to this threat (hence the cessation of breathing), but eventually, the body will arouse itself and continue breathing if it is to survive.3,4
Frequently, however, there are chronic threats to the airway that don’t rise to the level of immediate survival but do challenge the level of blood oxygen and oxygen delivery on a chronic basis. Chronic threats to airflow include anything that narrows the airway and makes breathing more effortful, which is very pro-inflammatory. We will look more closely at these threats in a moment.
It is important to note that chronic threats to breathing require persistent, chronic behaviors to mitigate oxygen level over time. These suboptimal behaviors are called compensations, and they successfully overcome the chronic threat. When compensations need to be used habitually, they have side effects — unintended consequences — that become chronic problems themselves. It is important to look at both the compensations and their consequences in order to frame our questions about the airway properly.
Compensations and consequences
Both compensations and consequences can be characterized in three domains: structure, function, and behavior. Here is a brief description of how each relates to breathing.
Structure refers to the anatomy of the airway — specifically it’s size, shape, and contours. Ideally, air should flow from the tip of the nose to the bottom of the throat in an easy, laminar flow pattern.1 Even around the nasal turbinates that “turbulate” the air to spin particulate matter into the mucous for filtering, the air should flow easily.
Where there is a narrowing of the airway, the air will swirl and become turbulent. This creates a negative pressure gradient that pulls on the sides of the airway making it even more narrow. If the tissue is resilient, it might flutter (i.e., snoring), but if it is not, it might close up. In either case, it takes more physical effort to pull air through the narrow spot. (Try breathing through a drinking straw to feel it.) During the day, this leads to fatigue. During the night, it leads to fragmented sleep.5,6 Turbulence makes it all the more effortful to breathe and triggers compensations.
Structural malformations that cause turbulence include:
- collapsed or narrow nostrils
- a deviated nasal septum
- a narrow nasal aperture (as part of a narrow maxilla)
- a constricted pharynx (as a result of a deficient maxilla and/or retrognathic mandible)19,20
These anatomic distortions are primary risk factors for airway flow limitation.
Function refers to the physiology of the airway. Any soft tissue enlargement that narrows the airway with swelling, mucous, adipose tissue, and inflammation leads to more turbulence. Allergies and food sensitivities, frequent colds and infections, swollen lymph tissue, fat deposits at the base of the tongue, swollen mucosa around the turbinates, polyps, cysts, and tumors get in the way. Acid from reflux irritates the throat, nose, and sinuses, making them swell. Narrow airways can lead to eustachian tube stenosis, conductive hearing loss, recurrent otitis media, and dysfunction.7 Obstructions are risk factors for airway flow limitation.
Behavior is the most overlooked and misunderstood component of airway dysfunction. Orthodontists, in their quest for a perfect occlusion, do everything they can to eliminate cooperation from the equation of their treatment planning. Talking about “behavior” is anathema. Unfortunately, this resistance has blocked progress on this issue.
Airway-focused orthodontists, however, realize that compensations and behaviors lie at the root cause of breathing dysfunctions and, therefore, must be considered when trying to establish a long-term cure. Leaving compensations at play means leaving their consequences at play, including treatment instability. Dysfunctional breathing and poor tongue posture and function are risk factors for airway flow limitation.
Common examples of compensations at night include mouth breathing, faster breathing, a faster resting heart rate, short bursts of very rapid heart rate, heavy breathing, forward head posture, stomach sleeping, tossing and turning, frequent awakenings, nightmares, and more.8,9 Any time the lips are apart or any time you can hear breathing — snoring or not — that person is in airway distress.
The unintended consequence of airway dysfunction is a distortion of the shape of the face and a suboptimal face that worsens airway function.10 Poor airway function can lead to chronic intermittent hypoxia that can affect any and all systems of the body. In children, it can damage the growing brain, interfere with sleep, and aggravate neurocognitive and behavioral development.11 In adults, it can lead to comorbidities in any system of the body, along with global pain and dysfunction. It is a vicious cycle of compensation and consequence that must be interrupted if a patient is to have their distress relieved.
Another unintended consequence of poor skeletal form is malocclusion. Teeth cannot fit into a container that is misshapen. The symptom of malocclusion is completely independent of the symptom of air flow limitation. Malocclusion and flow limitation may have a common origin in skeletal distortion, but there is no direct connection. This is why the research is equivocal. Studies that look to prove a connection (or lack thereof) between two things that are not connected are looking in the wrong place.
The role of the orthodontist: breaking the cycle
All orthodontists are familiar with the term “adenoid faces.” It is a condition that has been described in the literature for over a hundred years and has been researched extensively. We know that this phenotype (the final expression of the genes) produces a particular dental malocclusion — the high angle open bite — that is particularly difficult to correct. This phenotype did not exist in our ancestors. 21-25, 27
The adenoid face is not the only phenotype that occurs with airway dysfunction. Various compensations can lead to a variety of phenotypes, including open bites, deep bites, vertical excess, and the full range of angle classifications.12-16 This phenomenon was amply demonstrated by Egil Harvold’s monkey studies where each monkey developed a different facial distortion from the one experimental etiology: complete nasal obstruction. We also see this in humans who have mouth breathing and open mouth posture. How can it be that one etiology can lead to so many different facial phenotypes?
To solve this dilemma, we must revise yet another concept that orthodontists have been polarizing about since the profession began: nature vs. nurture.
While there are genetic influences to facial shape, the modern study of epigenetics only describes how genes are expressed based on their interaction with the environment, making this duality moot. As stated by Susan Herring, the idea that “bone genes’’ determine a person’s facial shape is not only simplistic but also, for the most part, false. Both genetic and environmental factors are at play.17
We cannot control the genetics, but we can control the environmental input to the genes. The role of the orthodontist must focus on optimizing facial growth by changing the inputs that influence it. That is, by reducing the need for compensations and by guiding the behaviors that stimulate growth and its vector, we can change the way the entire face grows. Another way of saying the same thing is that there are no genes that code for crooked teeth or dental crowding per se.
The teeth are just innocent bystanders of a form/function/behavior cycle. The way teeth settle into place is just an unintended consequence of the way the jaws take form; the way the jaws take form is an unintended consequence of poor function; and poor function is most often a consequence of a struggle to breathe easily from very early on in life. Malocclusion is just a symptom of this process.
Interrupting the form/function/behavior cycle is the most important thing an orthodontist can do for people’s health, no matter their age or stage of dental development; but the earlier the problem or trend is recognized, the better. No longer can we polarize around the form versus function issue. To get a child on a trajectory toward an optimal airway, we must address both form (by reshaping anatomy toward ideal) and function (by improving physiology and behavior).
When the American Dental Association says that we must help children “develop an optimal physiologic airway and breathing pattern,” we have to lessen constriction of the airway anatomy, mitigate harmful physiological challenges, and teach appropriate behaviors for optimal wellness not only when we treat malocclusion, but throughout life. This is how the cycle is broken and redirected toward health.
Yes, creating a beautiful smile and a pretty yearbook picture has its value, but it can no longer be a justification for ignoring other matters. Good structure can be beautiful, but straight teeth in a deficient structure is itself a compensation and prone to relapse over time. Focusing on optimizing the airway gives the orthodontist a better foundation for a beautiful smile and optimal facial balance beyond the dental component/teeth.
Seeing the problem
Once we learn to see the compensations and consequences of poor breathing, we never look at a growing face in quite the same way. Instead of seeing a child’s face as a static phenotype, we now see the dynamic process a child is going through. We don’t just see what a child is but what they are becoming (and will continue to become if nothing is done).
The tools for assessment focus not on the teeth, but on anything that causes turbulence in the airway.
Structure (Figure 1)
The CBCT allows us a better view of the midfacial collapse that so often occurs in orthodontic cases. We are able to see the nasal fossa from front to back and visualize obstructions. The shape and size of the airway is now readily apparent.
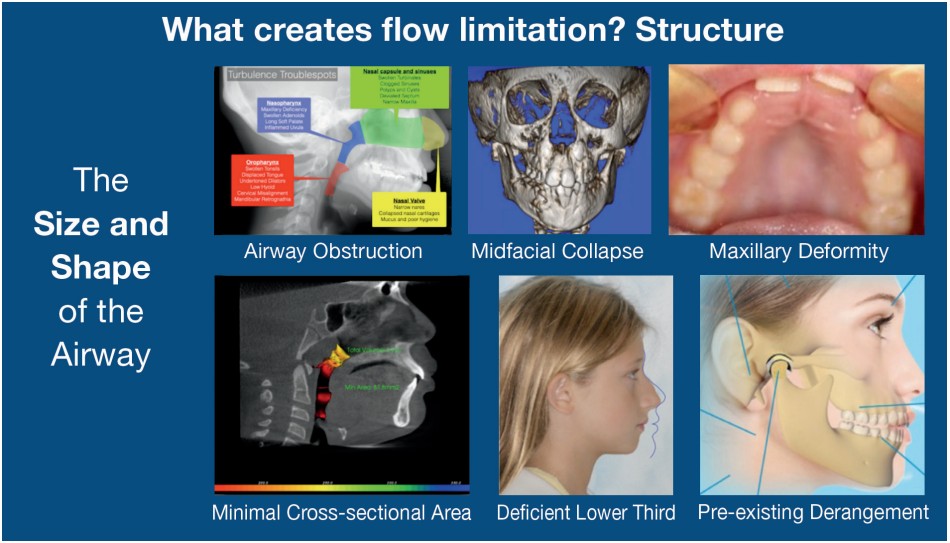
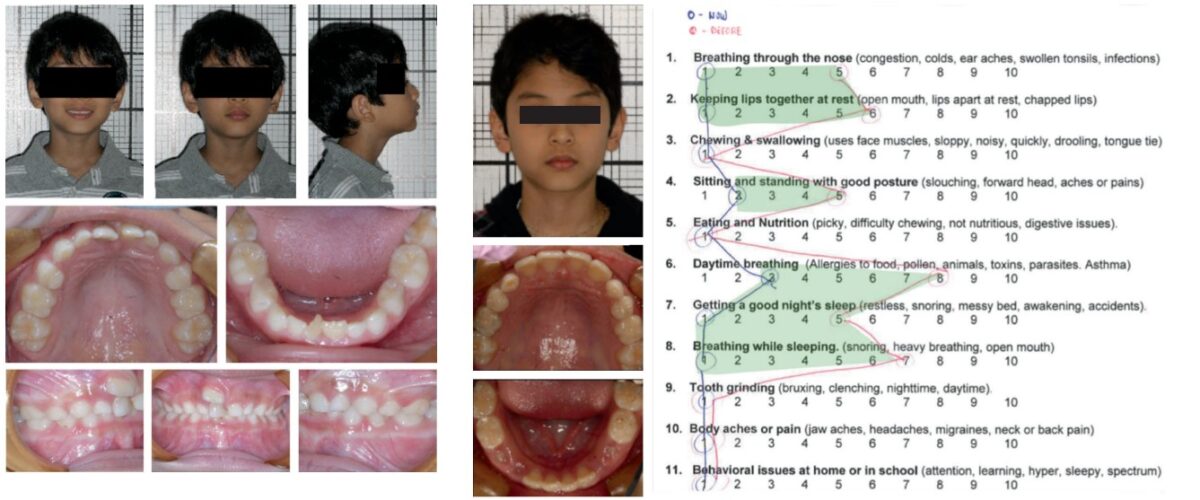
Many orthodontists that “do airway” talk about a “narrow palate,” as if that’s the key to the airway. It is an important finding, but we have to realize that the narrow palate is just one aspect of the collapse of the entire maxilla. The two photos on the upper right of Figure 2 are from the same boy. This is a deformity of the entire maxilla, not just the palate.
We now pay more attention to the overall shape of the face, comparing it to not just a random sample of peers, but to pre-industrial skeletal samples when there was very little malocclusion in the population, or to samples of children that grew up with naturally straight teeth from the Bolton-Brush database. Now we see just how deficient the lower third of the face has become in more modern times.
Function (Figure 2)
The collapse of the airway happens most easily at night, so we need to be able to measure fragmented sleep (pulse oximetry), audible breathing (snore recording), and how airway collapse affects daytime and nighttime experience (sleep inventory).
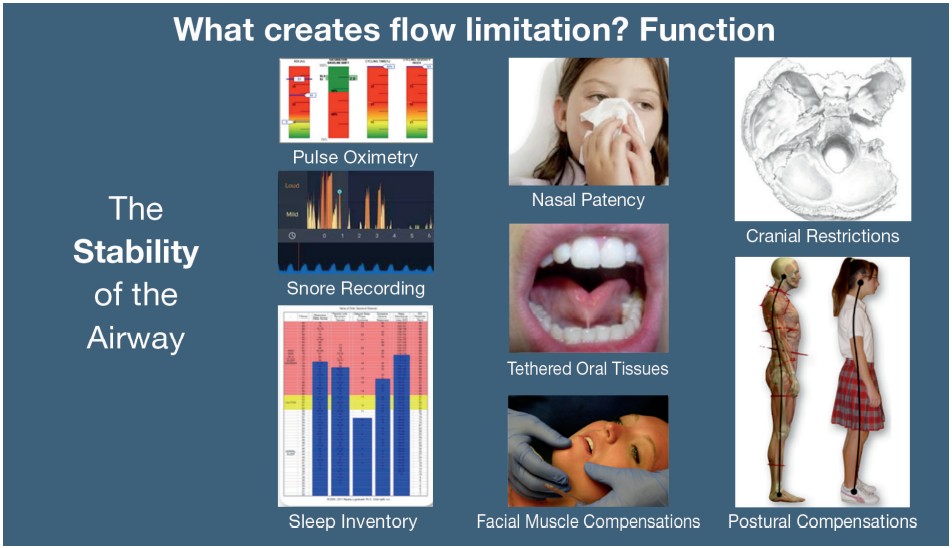
History focuses on inflammation, swelling, allergy, mucous, or irritation in the airway. We need to know if a child has difficulty with nasal breathing at all. We look at the tongue as an airway dilator muscle and measure its function with pressure sensors. We record and measure how the lips, chin, and cheeks are used for swallowing, and how they affect the balance of forces in the mouth. We look at not just the maxilla and mandible, but all 22 bones of the skull to be sure they work in concert to provide good development. We understand there is a body attached to the teeth, and that they mutually influence each.
Behavior (Figure 3)
If behavior is the cause of the problem, you have to be able to spot and measure the cause as well as the outcomes of the treatment. Outcomes are not just dental terms. They are quality of life terms. How are patients breathing, feeling, sleeping, and performing in life? More than being symptom-free, are they optimally well?
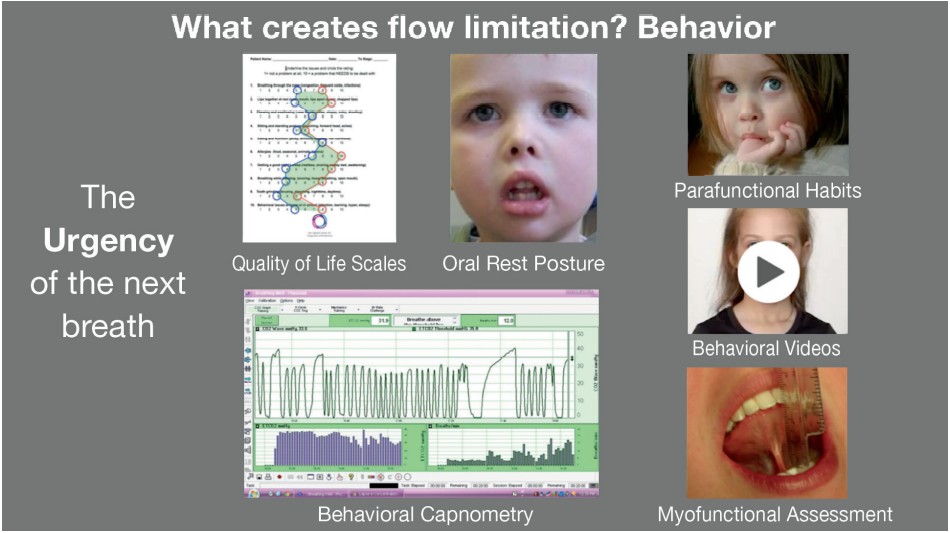
We measure the way they breathe during the day as well as at night and understand the compensations they have adopted (behavioral capnometry). We have to be able to spot open mouth posture from across the room. We try to figure out why they adopted their compensations, and why their habits linger. We understand the pervasive influence of soft tissue dysfunction on the entire system. Videos help us learn to read the face for clues about what’s going on inside.
And like it or not, we have to make peace with the tongue. The tongue is more than just something that makes the teeth wet, while we try to do our work. It guards and guides the airway and breathing. We learn its every move and train it to guide growth.
What would you do?
Here are three case examples for you to consider. If you were concerned about the airway and a child’s health, would you approach these cases any differently than you do now? In this limited space, we can only provide snippets of these real case examples, but we hope they stimulate further thinking about the topic for your patients.
Case No. 1: Bimaxillary protrusion
Even for those of us that don’t use extraction protocols as much as we used to, bimaxillary expansion seems to be one lingering application for it. The protrusion of the lips and the difficulty keeping the lips closed seems a perfect indication for retraction of the anteriors.
A 10 year-old boy’s story is illustrated in Figure 4. His airway history is significant from an early age. Figure 5 shows his pharyngeal anatomy.
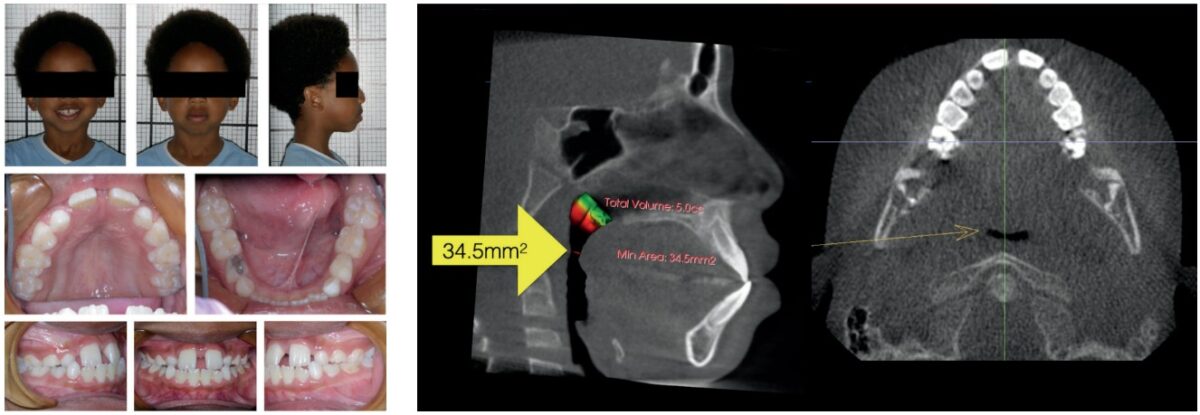
Would retraction of the teeth be appropriate here? Would expansion be appropriate here? When weighing the priorities of facial appearance against an optimal airway, how do you make that decision? Would you feel comfortable decreasing available tongue space in this case knowing that the tongue has to go backward if it can’t be placed in the front of the face? Would extractions cause an airway problem here? Absolutely not. There is already an airway problem here, and it has been here for a long time. Would extraction and retraction ignore an airway problem here? Of course. Let us ask you this: If this was your child, what would you do?
Case No. 2: An easy expansion case
The mom of a 6-year-old boy (Figure 6) brought him in “early” for the ectopic upper central incisor. He’s just beginning his transition, so even if you favor two-phase treatment, would you wait for more “growth and development” before starting? If you are confident in your nonextraction skills, would you wait for the permanent dentition? Or is it wise to start removing deciduous teeth to guide eruption?
Looking a little deeper may give you some clues. Even though his lips look competent, his mom, a nurse, sees that his mouth is often open as a compensation for his asthma and allergies. She is surprised to learn that the crowding of the two permanent incisors (and surely more to follow) is related to that oral rest and breathing posture. So now what?
More significant than his teeth, his breathing pattern was exacerbating his allergies and asthma (Figure 7). We used a myofunctional training protocol to slow down his breathing and correct his tongue posture. Since then, the mom says there have been no more visits to the hospital, and he only uses his inhalers during the worst of pollen seasons. Look at the quality of life changes he achieved. The fact that we set up his occlusion for optimal development is just icing on the cake.
Case No. 3: Are aligners enough?
This young woman (Figure 8) said she came in to “straighten my lower teeth.” Her narrow maxilla, history of snoring, and constricted airway begged for a closer look. She blamed her history of fatigue on her age and college curriculum.
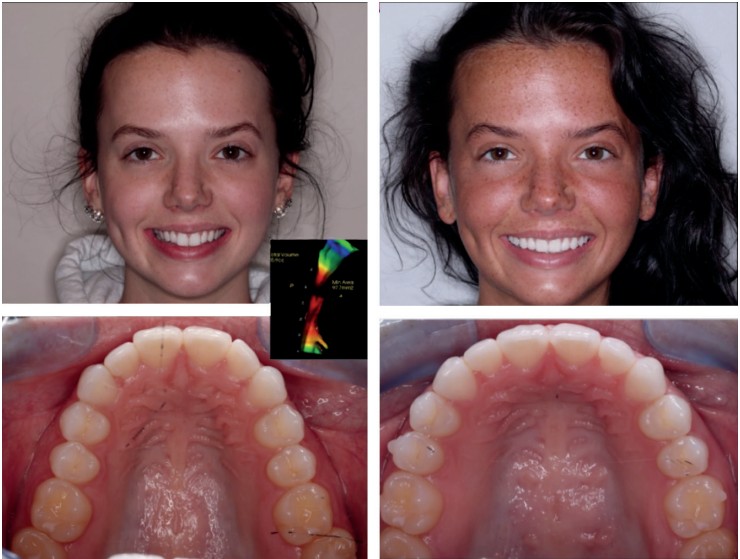
Would aligners and IPR be enough to satisfy her chief complaint? Probably. But if you could offer her something more, would you do it? Mini-screw expansion along with aligners may seem like overkill in this case, but it overcame her flow limitation dramatically. And if needed, those limitations could be further improved with Surgically Facilitated Orthodontic Therapy (SFOT).28
While the difference in her facial appearance and broad smile were reward enough, she calls her treatment a “life-changing experience.” Now she is no longer fatigued, sleeps quietly, and wakes up refreshed. Here, form and function improvements complement each other.
In summary: the real question
You cannot adequately treat airway problems without correcting the behaviors that caused them. This is a painful reality for mechanically-minded orthodontists who think perfection lies in our hands, our wires, or our aligners. Nonetheless, the imperative to give our patients “an optimal physiologic airway and breathing pattern” begs us as orthodontists to expand our thinking and expand our range of services to include structure, function, and behavior. Our efforts must include interdisciplinary collaboration with many practitioners in the wellness and medical communities as well.
Our questions must expand from “do we affect the airway?” to “how can we help the airway?” While we cannot treat OSA on our own, we can treat flow limitation better than anyone else. We must stop dithering about this subject because we are wasting precious time while many of our patients are needlessly suffering — now and into their futures — unless we do something about it.
Dr. Raphael offers the basics of airway orthodontics in his article, “Airway orthodontics the new paradigm: part 1, addressing the airway.” Read it here: https://orthopracticeus.com/ce-articles/airway-orthodontics-new-paradigm-part-1-addressing-airway/
- Fitzpatrick MF, McLean H, Urton AM, et al. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur Respir J. 2003;22:827-832
- Balbo M, Leproult R, Van Cauter E. Impact of sleep and its disturbances on hypothalamus-pituitary-adrenal axis activiy. Int J Endocrinol.
- Edwards BA, Eckert DJ, McSharry DG, et al. Clinical predictors of the respiratory arousal threshold in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2014;190(11):1293-300.
- Eckert DJ, Younes MK. Arousal from sleep: implications for obstructive sleep apnea pathogenesis and treatment. J Appl Physiol. (1985); 2014;116(3):274-278.
- de Godoy LB, Palombini LO, Martinho Haddad FL, et al. New insights on the pathophysiology of inspiratory flow limitation during sleep. 2015;193(3):387-392.
- Gold AR, Dipalo F, Gold MS, Broderick J. Inspiratory airflow dynamics during sleep in women with fibromyalgia. 2004;27(3):459-466.
- Eichenberger M, Baumgartner S. The impact of rapid palatal expansion on children’s general health: a literature review. Eur J Paediatr Dent. 2014;15(1):67-71
- Guilleminault C, Chowduri S. Upper Airway Resistance Syndrome is a Distinct Syndrome; Am J Respir Crit Care Med. 2000;161(5):1412-1413.
- Guilleminault C, Poyares D, Palombini L, et al. Variability of respiratory effort in relation to sleep stages in normal controls and upper airway resistance syndrome patients. Sleep Med. 2001;2(5):397-405.
- Stupak HD, Park SY. Gravitational forces, negative pressure and facial structure in the genesis of airway dysfunction during sleep: a review of the paradigm. Sleep Med. 2018;51:125-132.
- Horne RSC, Roy B, Walter LM, et al. Regional brain tissue changes and associations with disease severity in children with sleep-disordered breathing. 2018;41(2).
- Banabilh SM, Samsudin AR, Suzina AH, Dinsuhaimi S. Facial profile shape, malocclusion and palatal morphology in Malay obstructive sleep apnea patients. Angle Orthod. 2010;80(1):37-42.
- Kerr WJ, McWilliam JS, Linder-Aronson S. Mandibular form and position related to changed mode of breathing – a five year longitudinal study. Angle Orthod. 1989;59(2):91-96.
- Peltomäki T. The effect of mode of breathing on craniofacial growth — revisited. Eur J Orthod. 2007;29(5):426-429.
- Kim YJ, Hong JS, Hwang YI, Park YH. Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop. 2010;137(3):306.e1-e11
- de Freitas MR, Alcazar NM, Janson G, et al.Upper and lower pharyngeal airways in subjects with Class I and Class II maloclussions and different growth patterns. Am J Orthod Dentofacial Orthop. 2006;130(6):742-745
- Moss ML. The functional matrix hypothesis of mechanotransduction revisited. 1. The role of mechanotransduction. Am J Orthod Dentofacial Orthop. 1997;112(1):8-11.
- D’Ascanio L, Lancione C, Pompa G, et al. Craniofacial Growth in children with nasal septum deviation: A cephalometric comparative study. Int J Pediatr Otorhinolaryngol. 2010;74(10):1180-1183.
- Yoon A, Abdelwahab M, Liu S, et al. Impact of rapid palatal expansion on the internal nasal valve and obstructive nasal symptoms in children. A Yoon, M Abdelwahab, S Liu, et al. Sleep Breath. 2021;25(2):1019-1027.
- G Felisati, C Meazzini, F Messina, MG Tavecchia, G Farronato. Orthopedic palatal expansion in the treatment of bilateral congenital choanal atresia: an additional tool in the long term follow up of patients? J Pediatr Otorhinolaryngol. 2010;74(1):99-103.
- Galland M, Van Gerven DP, Von Cramon-Taubadel N, Pinhasi R 11,000 years of craniofacial and mandibular variation in Lower Nubia. Sci Rep. 2016;9;6:31040.
- Armelagos GJ, Van Gerven DP, Martin D, Huss-Ashmore R. (1984). Effects of nutritional change on the skeletal biology of Northeast African (Sudanese Nubian) populations. Clark J, Brandt S, eds. In: Hunters to farmers: the causes and consequences of food production in Africa. Berkeley, CA: University of California Press;1984.
- Carlson DS, Van Gerven DP. Masticatory function and post-Pleistocene evolution in Nubia. Am J Phys Anthropol. 1977;46(3 PT 1):495-506.
- Carlson DS. Temporal variation in prehistoric Nubian crania. Am J Phys Anthropol. 1976;45(3):467-484.
- Festa F, Capasso L, D’Anastasio R, et al. Maxillary and mandibular base size in ancient skulls and of modern humans from Opi, Abruzzi, Italy: a cross-sectional study. World J Orthod. 2010;11:e1-e4.
- The Role of the Dentist in the treatment of Sleep-Related Breathing Disorders. Adopted by the American Dental Association’s House of Delegates, 2017
- Rose JC, Roblee RD. Origins of dental crowding and malocclusions: An anthropological perspective. Compend Contin Educ Dent. 2009;30:292-300.
- Roblee RD, Bolding SL, Landers JM. Surgically Facilitated Orthodontic Therapy: A New Tool for Optimal Interdisciplinary Results. Compend Contin Educ Dent. 2009;30(5):264-275.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
