Drs. Rohit C.L. Sachdeva, Takao Kubota, Eric Howard, and Kazuo Hayashi illustrate how suresmile expands orthodontists’ esthetic appliance options
Introduction
In previous articles,1-18 the versatility of suresmile® technology in enabling the orthodontist to manage a broad range of mal-occlusions using customized target prescription archwires with fixed labial edgewise brackets has been discussed comprehensively. Suresmile provides the orthodontist unprecedented versatility to control ortho-dontic tooth movement by choosing the appropriate timing for customized therapeutics. In addition, it enables the orthodontist to preferentially affect the expression of the prescription archwire (staging subtractive or additive bends) based upon the patient’s needs and bracket system employed.
Suresmile also expands the abilities of the orthodontist to fulfill the patient’s desire for esthetic appliance systems. These include both lingual fixed appliances and aligners.
The purpose of this article is to discuss two patient histories that demonstrate the treatment of a patient with suresmile Lingual.
Patient S.N.
(suresmile Lingual appliance)
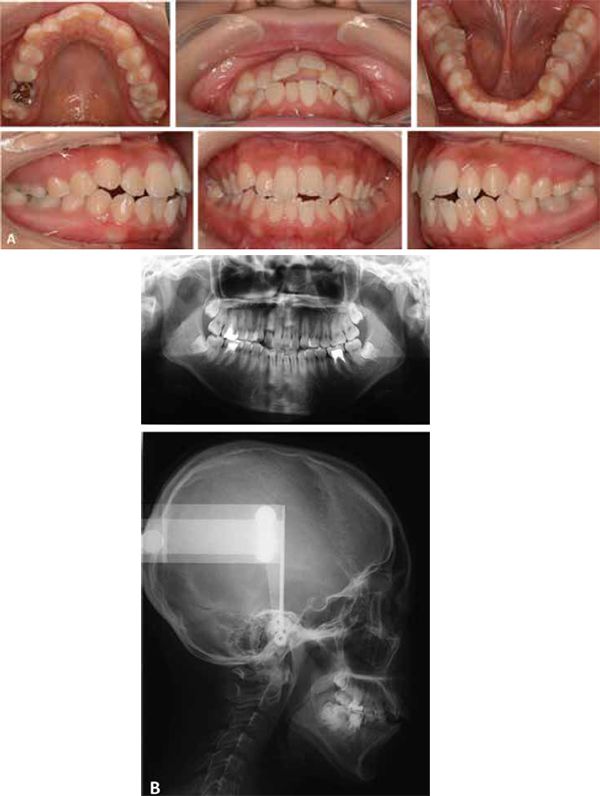
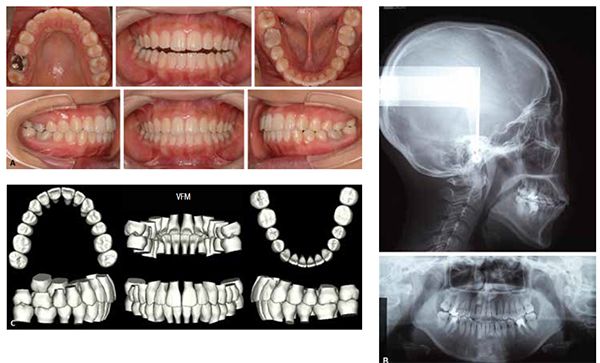
Patient S.N., a 21-year-old female patient presented with a chief complaint of “I do not like the appearance of my teeth” and very much insisted on having hidden braces.
Her clinical and cephalometric findings suggested that she had a skeletal Class II pattern and a long lower facial height. She presented with a Class 1 dental malocclusion with an anterior openbite. There were no signs of TMJ symptoms. Her lower first molars were restored with crowns and a pulpotomy. Her upper-right first molar was heavily restored. Her oral health was good. Her initial records are shown in Figure 1.
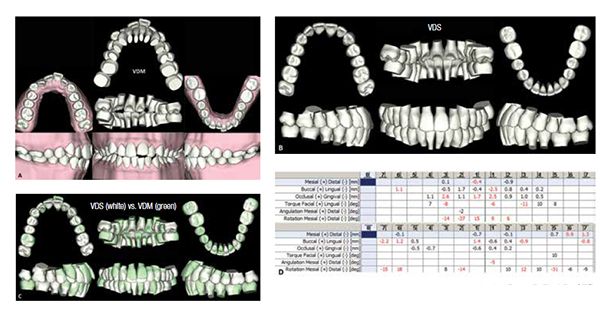
It was decided to treat Patient S.N. in a non-extraction manner with minor dental expansion in both the upper and lower arches. Lower arch crowding was corrected with minor interproximal reduction. Figure 2 shows the Virtual Diagnostic Simulation (VDS) demonstrating the treatment plan.


Indirect bonding (IDB) jigs for the patient were designed in the following manner. First, the Virtual Diagnostic Simulation that represented the setup (target occlusion) was converted to an STL file, which enabled its 3D printing (Figure 3A). Next, an impression of the 3D printed setup was taken and the impression poured in plaster (Figures 3B-3C). Brackets were bonded on the plaster model. Indirect individual tooth bracket jigs were then fabricated (Figures 3D-3E). It should be noted that with suresmile Lingual, the clinician may bond the patient directly and circumvent the use of IDB. This requires appropriate adjustments be designed in the archwire based upon a target setup designed from a virtual therapeutic scan. This approach is best considered in patients presenting with minimal crowding. Recently, suresmile has developed technology to directly print an IDB tray for both lingual and labial indirect bonding of fixed appliances. This enables the doctor to initiate orthodontic treatment with indirect bonding and circumvents the need for a therapeutic scan. The entire design of the target setup and the accompanying IDB trays with the complementary archwires (if needed) is based upon an initial diagnostic scan. A future article will discuss the design and clinical use of the suresmile IDB system.
Initially, a Quadhelix was used in both lower and upper arches to gain minimal uprighting of the buccal segments though expansion (Figure 4).

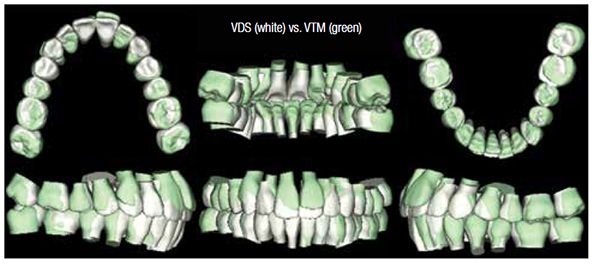
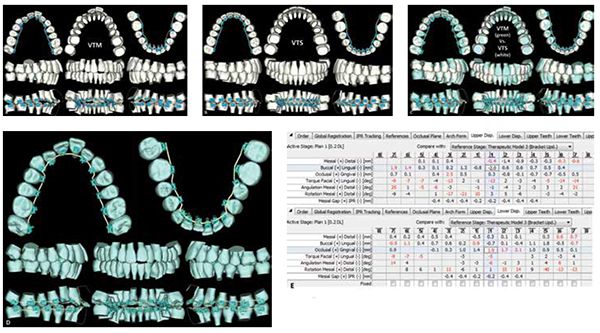
Eight weeks later, the patient was bonded using the customized jigs. The teeth were bonded with DENTSPLY GAC In-Ovation® L (www.gac inovation.com) brackets with 0.018″ slot width. At this appointment, a therapeutic scan of the patient was taken (Figure 5). Super-imposition of the VTM against the VDS shows that the planned archwidth was achieved with Quadhelix appliances in both the upper and lower arch (Figure 6). The Virtual Target Setup (VTS) is shown in Figure 7B. Superimposition of the Virtual Target Setup against the Virtual Therapeutic Model (VTM) is shown in Figure 7C. The archwire designed against the VTM is shown in Figure 7D.
No interim archwires were placed. Upper and lower .016″ CuNiTi AF 35°C suresmile precision archwires were installed 1 month post therapeutic scan (Figure 8). One month later, both upper and lower .016″ x .016″ CuNiTi AF 35°C suresmile square precision archwires were inserted (Figure 9). Six weeks later, both upper and lower .016″ x .022″ CuNiTi AF 35°C suresmile precision archwires were placed (Figure 10).
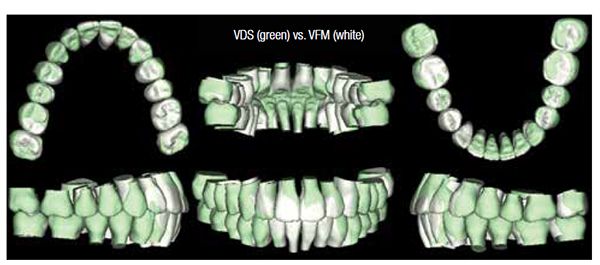
The patient was next seen a month later. At this stage in treatment, it was decided to have the patient wear up-and-down elastics to settle down the canines. Buttons were bonded on the right buccal segment on the upper and lower canines and the lower premolar to attach the elastics (Figure 11). The canines settled within 2 weeks (Figure 12), and the patient was debonded 1 week later. The final records are shown in Figure 13. The total active treatment time for patient was 7 months. The Virtual Final Model (VFM) is superimposed on the Virtual Diagnostic Simulation (VDS). Note how closely the outcome matches the plan (Figure 14).


Hybrid Lingual appliance
Patient KEH
It is common to see patients who are accepting of a treatment regimen that involves upper lingual fixed appliances coupled with a lower labial appliances. This approach to care addresses their primary concern of not displaying upper fixed appliances. Moreover, it also provides a more cost-effective solution for the patient as compared to a total lingual fixed appliance approach. Figure 15 provides a brief overview of a patient history (KEH) using a hybrid lingual appliance approach in managing extraction therapy.
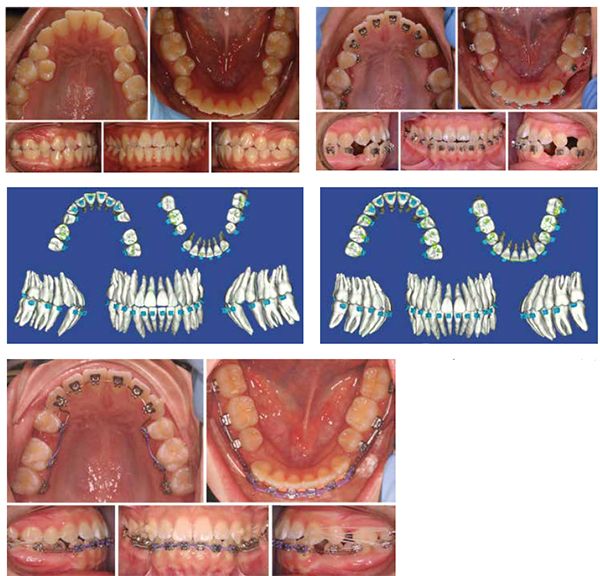
were extracted and the patient bonded using indirect bonding. Note upper lingual and lower labial fixed appliances were used. 15C. Immediately post bonding a therapeutic scan of the patient was taken to design the target setup and the appropriate 3D customized prescription archwires. 15D. The virtual 3D target setup. 15E. After initial alignment space closure using sliding mechanics accompanied with the use of intermaxillary elatics to control anchorage was initiated.
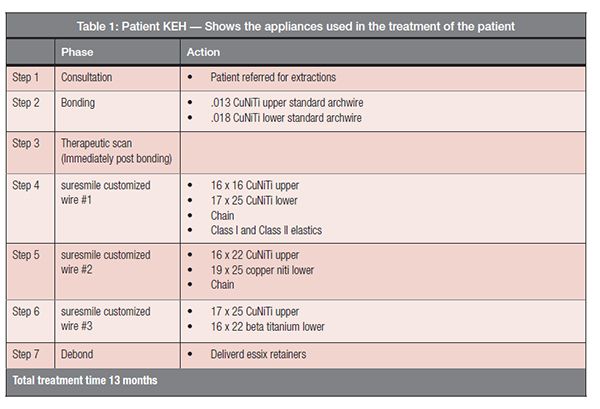
Table 1 shows the archwires used.

Discussion and conclusions
Both patients S.N. and K.E.H. demonstrate the broad capabilities of suresmile technology in enabling the orthodontist to address patients’ needs for an esthetic-appliance solution involving lingual fixed appliance treatment. And equally important is not sacrificing the doctor’s ability to achieve complete control of orthodontic tooth movement with lingual therapy. Future articles will discuss the use of both suresmile IDB and aligner solutions for the orthodontic professional.
Acknowledgment
The authors wish to express their gratitude to Nikita Sachdeva for her assistance in the preparation of this manuscript.
 Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com to access information.
Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com to access information.
Takao Kubota, DDS, PhD, is in private practice at the Yours Orthodontic Clinic, 378-6 Motomura Yame City, Fukuoka 834-0063 Japan. He is also the co-founder of the Institute of Orthodontic Care Improvement in Japan, and Associate Professor in the Department of Orthodontics, Kanagawa Dental College, Yokosuka, Japan.
Dr. Eric Howard, DDS, PhD, is in private practice at Long Orthodontic Associates, 519 E. Main Street, Lititz, Pennsylvania.
Dr. Kazuo Hayashi practices at the Hokkaido Health Sciences Center, Tobetsu, Japan.
- Sachdeva R. BioDigital orthodontics: Planning care with Suresmile technology: part 1 Orthodontic Practice US. 2013;4(1):18-23.
- Sachdeva R. BioDigital orthodontics: Designing customized therapeutics and managing patient treatment with Suresmile technology: Part 2. Orthodontic Practice US. 2013;4(2):18-26.
- Sachdeva R. BioDigital Orthodontics: Diagnopeutics with Suresmile technology (Part 3). Orthodontic Practice US. 2013;4(3):22-30.
- Sachdeva R. BioDigital orthodontics: Outcome evaluation with Suresmile technology: part 4. Orthodontic Practice US. 2013;4(4):28-33.
- Sachdeva R. BioDigital orthodontics. Management of Class 1 non–extraction patient with “Fast–Track”©– six month protocol: Part 5. Orthodontic Practice US. 2013;4(5):18-27.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of Class 1 non–extraction patient with “Standard–Track”©– nine month protocol: Part 6. Orthodontic Practice US. 2013;4(6):16-26.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of space closure in Class I extraction patients with Suresmile: Part 7. Orthodontic Practice US. 2014;5(1):14-23.
- Sachdeva R, Kubota T, Moravec S. BioDigital orthodontics. Part 1-Management of Class 2 non–extraction patients: Part 8. Orthodontic Practice US. 2014;5(2):11-16.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Part 2-Management of patient with Class 2 malocclusion non–extraction: Part 9. Orthodontic Practice US. 2014;5(3):29-41.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Part 3- Management of patients with Class 2 malocclusion extraction: Part 10. Orthodontic Practice US. 2014;5(4):27-36
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of patients with class 3 malocclusion: Part 11. Orthodontic Practice US. 2014;5(5):28-38.
- Sachdeva RCL, Kubota T. BioDigital orthodontics. Part 1 – Management of patients with openbite (1): Part 12. Orthodontic Practice US. 2014;5(6):22-31.
- achdeva RCL, Kubota T,Lohse.J. BioDigital orthodontics. Management of patients with openbite (2): Part 13. Orthodontic Practice US. 2015;6(1):13-23.
- Sachdeva RCL, Kubota T, Hayashi K, Uechi J, Hasuda M. BioDigital orthodontics: Management of patients with transverse (midline) discrepancies: Part 14. Orthodontic Practice US. 2015;6(2):25-36.
- Sachdeva RCL, Kubota T, Hayashi K, . BioDigital Orthodontics: Management of Patients with Transverse (Midline) Discrepancies (2):part 15. Orthodontic Practice US. 2015;6(3):28-44.
- Sachdeva RCL, Kubota T, Hayashi K, Uechi J, . BioDigital Orthodontics. Management of skeletal deformities with orthognathic Surgery-fusion model (part 1). Orthodontic Practice US. 2015;6(4):26-32.
- Sachdeva RCL, Moravec S, Kubota T, Uechi J. BioDigital orthodontics. Management of skeletal deformities with orthognathic surgery — Direct (CBCT) (2): part 17. Orthodontic Practice US. 2015;6(5):28-35
- Sachdeva RCL, Kubota T, Uechi J. Management of skeletal deformities with orthognathic surgery (OraScan) (3): part 18. Orthodontic Practice US. 2015;6(6):30-36.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
