Drs. Rohit C.L. Sachdeva and Takao Kubota discuss how suresmile works within the aligner production process
Introduction
Today, aligners are broadly accepted by the orthodontic community for use in orthodontic treatment. Treatment with aligners is generally restricted to a select group of patients. Factors affecting the use of aligners include:
- the patient’s desire
- the doctor’s skills in managing the appliance
- the nature of planned tooth movement
- the affordability
- the length of care
Historically, suresmile® technology has focused on providing customized therapeutic solutions for labial- and lingual-fixed appliance treatment.1,2 In recent years, suresmile has extended the functional range of its technology to enable the doctor to design aligners. As a result, the clinician may design a combined therapeutic solution comprising the use of both fixed and removable appliances (when indicated). Furthermore, the advantage of using a “unified” computer-aided design workstation provides the practice with superior ergonomics and cost-effectiveness and minimizes the burden of additional training in another system.
Figures 2A-2B: 2A. Therapeutic intraoral scan showing brackets 2B. Tooth surfaces have been digitally “conditioned” to prepare them for the design and fabrication of aligners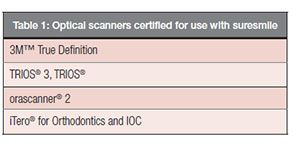
In this article, I discuss how suresmile facilitates the design of aligners, the process of producing the aligners, and a handful of use cases with patient histories. It is important to recognize that suresmile does not fabricate aligners. The following section briefly outlines the steps involved in designing and manufacturing aligners.
Step 1: Imaging
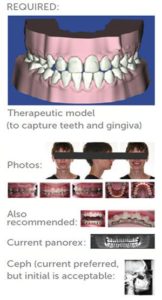
suresmile recommends an in vivo optical scanned image as input. The in vivo image of the dentition should be scanned to include the surrounding gingival tissue (a minimum of 5 mm in height on the labial/lingual surfaces of the teeth). A scanned image of the bite for interarch model registration is required. Also, current standard intraoral images — cephalometric and panoramic X-rays of the patient — are requested (Figure 1). Intraoral scans with brackets are acceptable; the suresmile laboratory can remove the brackets using digital erasers and condition the hidden surfaces of the tooth to approximate the original tooth anatomy (Figures 2A-2B).
A list of the certified scanners is provided in Table 1. The aligners may be designed at any stage in treatment — from the start of treatment, midtreatment, or the finishing and retention phases — to suit the doctor’s therapeutic protocol.
Step 2: Planning and appliance design

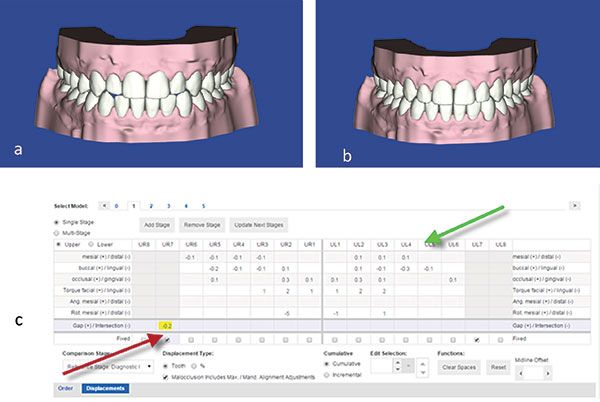
The processed 3D image is used to design the target setup. The doctor has the ability to move the teeth on the virtual working model in all three planes of space, measure tooth displacement, and also plan for interproximal reduction (Figure 3). Tools for measuring the quality of the target setup based on both the ABO and suresmile guidelines are available (Figure 4).
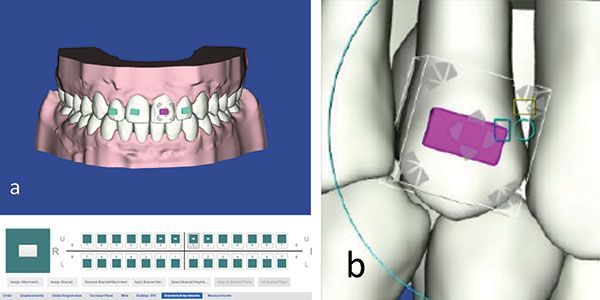
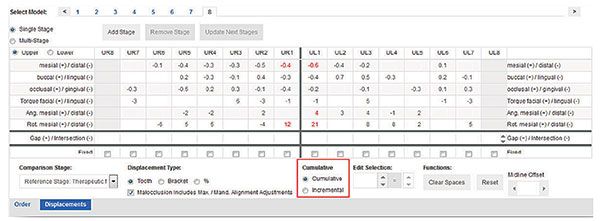
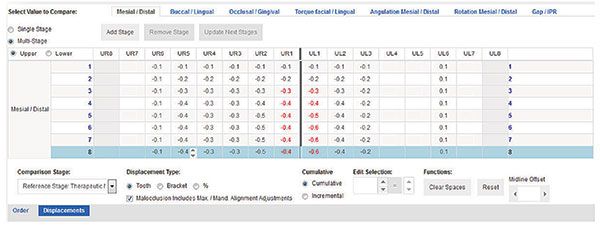
Once the target setup is completed, the doctor may apply attachments to the teeth to aid in better control of tooth movement (Figure 5). Next, the doctor applies her preferences to stage incremental tooth movements. (Note: These are preset by the doctor and applied in default mode.) See Figure 6A. The process of serially staging the models is automatic and driven by the preset values (Figure 6B). The operator can always override the default settings for the entire series of incremental tooth movements or for any single stage to affect the magnitude and nature of tooth displacement. In addition, the doctor has the choice to select the hardness of the aligner material and calibrate it to the nature and amount of the staged tooth movements. Staged movements may be observed both in a cumulative or incremental mode. The cumulative mode represents the aggregate of the tooth displacements for all the stages of tooth movement achieved up to the current stage. The incremental mode shows the amount of movement achieved between the previous stage and the current stage (Figure 7).
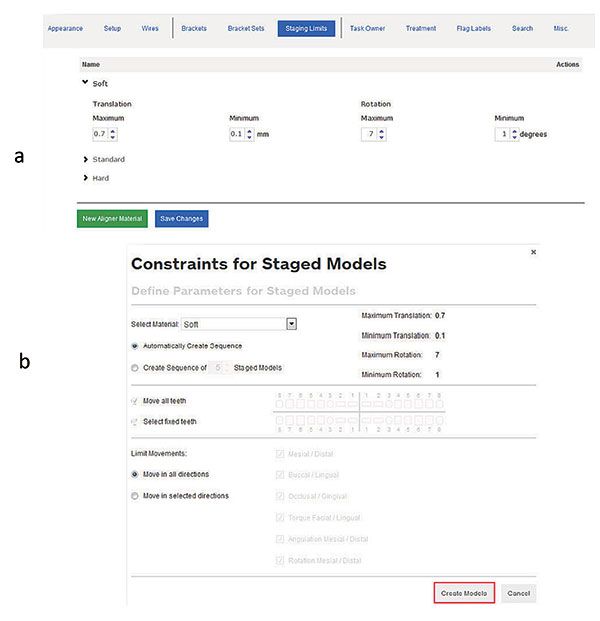
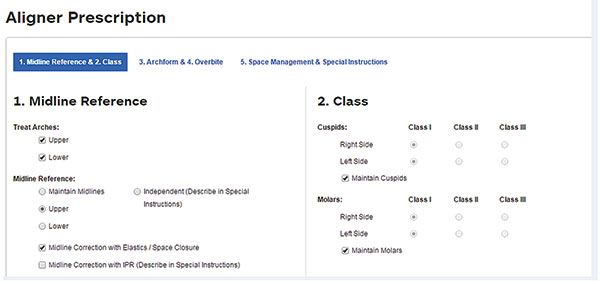
For an additional fee, suresmile will design the target setup based on the doctor’s prescription (Figure 8).
Step 3: Staging
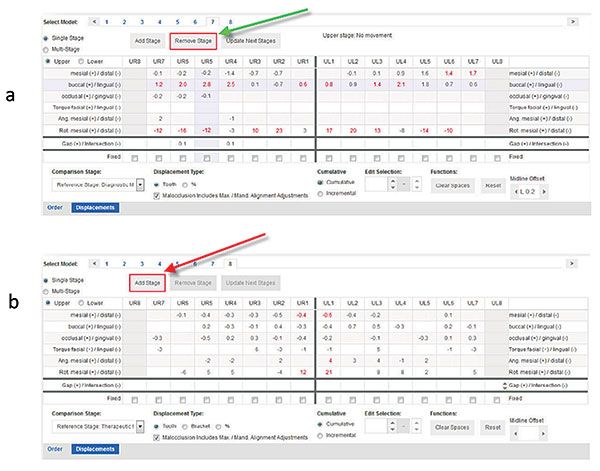
Once the target setup is accepted, the sequence of the automatically designed staged models are reviewed. The doctor has the ability to override any of the stages to suit the patient’s needs (Figures 9-10). The software automatically creates STL files of the staged models that can be saved on the desktop in a zip file for later use.
Step 4: Order and fabrication
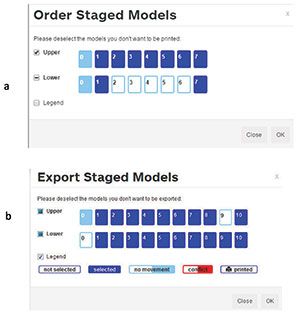
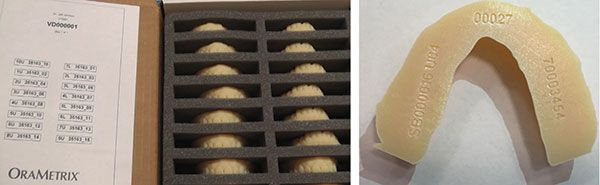
The operator can choose and print any stage of treatment (Figures 11A-11B) and has the option to order 3D hard copies of the models from suresmile (Figure 12) or from other sources. (Note: The virtual models can be automatically downloaded in STL format and subsequently exported.) The operator can then fabricate the aligners in-office using commonly accepted thermo-vacuum-forming techniques and materials.2
Three common clinical situations in which we have used suresmile aligners are described below:
Type 1
The concept of just-in-time retainer delivery is exemplified by this patient history. Two weeks prior to the patient’s debonding, the virtual target setup that was initially used to fabricate the suresmile finishing archwires was also used to design an Essix®-type retainer.3 The physical model (printed model) production was outsourced to an external laboratory, and the retainer was fabricated in-house and delivered on the day of debonding (i.e., just-in-time delivery) (Figure 13). This proactive approach to designing and fabricating the Essix-type retainer appliances has many advantages, including obviating the necessity of taking an additional scan or impression of the patient to design the appliance. This approach results in chairside time savings, which opens up chairside capacity and allows for more effective staff utilization and cost savings. Most importantly, this approach 1) adds to patient convenience by shortening the debonding visit and 2) minimizes the risk of immediate post-debonding minor rebound effects. Furthermore, the printed hard copy of the model is virtually indestructible, has a long shelf life, and may be used to fabricate additional replacement retainers.


Type 2
This patient was scheduled for debonding at her next visit. Unfortunately, the patient lost her lower anterior bracket, which resulted in rotational relapse of the lower left lateral incisor (Figure 14). Rather than rebond a bracket and add refinements to an archwire to correct the rotation (this would have added at least 6 to 8 weeks to treatment time), the initial virtual target setup was used to design active aligners to correct the relapse. To the patient’s delight, an earlier debonding appointment was scheduled (2 weeks later), and a series of aligners were delivered to facilitate the correction of the rotation (Figure 14). The approach toward this patient’s care had the obvious benefit of adding to her satisfaction and also minimized the additional care processes involved in managing fixed appliances, etc.
Type 3
Minor relapse was noted immediately posttreatment. The tooth positions were simulated on the virtual target setup to reflect the current tooth position. This model was then used as a reference model to stage the corrective tooth movements. Hard copies of the staged models were printed, and a series of aligners to correct the relapse were fabricated. Again, this approach to managing the patient obviated the necessity of taking an additional scan or impression of the patient (Figure 15).

In situations in which a substantial amount of relapse has occurred or significant interproximal reduction has been performed during fixed appliance therapy, it is recommended that a new scan be taken. It is difficult to judge and replicate the exact 3D positions of the teeth on the virtual model. A significant amount of interproximal reduction can drastically impact the shape of a tooth, making it difficult to fabricate accurate models and, in turn, aligners. A partial scan representing only the affected teeth may be taken; suresmile can then paste this scan into the original model. This process eliminates the need for a full scan, saving a considerable amount of chairside time.
Conclusions
It should be noted that no additional intraoral scans for the patients described above were taken, and the initial target setup was used to design and manufacture the aligners. For clinical situations in which the aligner is used as a removable retainer, or when no more than 10 aligners are required for correcting tooth position, suresmile provides a very viable, cost-effective solution.
Additionally, suresmile provides the doctor with enabling technology — specifically, a broad range of bundled diagnostic, communication, and therapeutic tools for total patient management. This bundling of tools avoids the issues associated with using multiple products from different vendors.
Successful care outcomes are driven by the orthodontist’s knowledge, skills, and commitment to excel within a cultural framework that practices the tenets of BioDigital orthodontics: patient-centered care, patient safety, and clinical effectiveness.4
Acknowledgment
We very much appreciate Nikita Sachdeva’s invaluable assistance in the editing and preparation of this article.
 Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com to access information.
Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com to access information.
Dr. Takao Kubota is in private practice in Yours Orthodontic Clinic, 378-6 Motomura Yame City, Fukuoka 834-0063 Japan. He is also the co-founder of the Institute of Orthodontic Care Improvement in Japan.
- Sachdeva R. BioDigital orthodontics: Planning care with Suresmile technology: part 1. Orthodontic Practice US. 2013;4(1):18-23.
- Sachdeva R. BioDigital orthodontics: Designing customized therapeutics and managing patient treatment with Suresmile technology: Part 2. Orthodontic Practice US. 2013;4(2):18-26.
- Sheridan JJ, LeDoux W, McMinn R. Essix retainers: fabrication and supervision for permanent retention. J Clin Orthod. 1993;27(1):37-45.
- Sachdeva R. Novus ordo seclorum: a manifesto for practicing quality care – part II. EJCO. 2015;3(1):2-14.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
