Dr. Bella Shen Garnett discusses accelerating treatment for patients with Class II malocclusions
It’s been wonderful to see more adults than ever seeking orthodontics. With an increasingly competitive job market, increased use of social media and selfie postings, people are more aware of their smiles and want to look their best. Recently, Kelton Global conducted a national smile survey that found individuals with straight teeth are 57% more likely to be chosen for a first date. Harris Poll, another national survey, revealed nearly 1 in 5 adults attribute their straighter teeth to a promotion or career upgrade. These surveys prove the old adage, “putting your money where your mouth is,” can impact far more than oral health and one’s social life. Investing in a healthy smile can lead to advancements in one’s career, too.
Many challenges come parceled within this growing segment. The opportunity to guide skeletal growth is now far behind us. Beyond clinical challenges, the formula is compounded with high or, at times, even unrealistic expectations. These busy adults are often well-educated and possess strong personalities. Many have recently re-entered the job market, or are aiming for a promotion. They may be getting married, or just got divorced and urgently desire to reinvent themselves. I can recall some of my best experiences and most rewarding finishes have come from taking on these challenging cases.
Class II malocclusions among adults whom elect only to be treated with Invisalign®, certainly qualify as one of those clinical challenges. I have fully embraced accelerated treatment partly because my Class II consults typically end with patients asking, “And how long did you say it will take?” in addition to various other market pressures. I tell them it doesn’t take that long just to align the front teeth. What takes time, and what the specialty of orthodontics is based on, is correcting their bite. How about correcting the bite and aligning teeth in half the time?
Now that I’ve implemented both micro-osteoperforations (MOPs) and high-frequency vibration (HFV) from Propel® Orthodontics, I have become increasingly confident in quoting significantly abbreviated finish dates, using MOPs or HFV alone, or even in combination with each other. Bear in mind, anticipated treatment times must still account for patient participation. But patient compliance is another reason I have become quite fond of these two accelerated treatment options. Adhering to the prescribed orthodontic regimen is incredibly important for aligner patients, especially the Class II patient. Fortunately, my most impatient patients are among my most compliant with their regimen. They are highly motivated from the beginning, the finish is soon within sight, and burnout is a foreign concept. In my practice, these cases are without question delivering the highest revenue per visit despite any minimal adjunctive device costs.
Correcting a skeletal Class II in an adult is typically going to involve surgery or camouflage. The camouflage is typically achieved by extracting maxillary first premolars, or often a combination upper first premolars and mandibular first or second premolars. Extractions themselves can deliver a predictable form of accelerated treatment often referred to as the regional acceleration phenomenon (RAP).1 The RAP effect delivers quite remarkable speed at space closures or bringing a buccally displaced canine back into the arch. Delaying the extraction until after level and align is completed is a successful way to fully harness its potential. However, for the Class II patient requiring maxillary distalization, premolar extractions will not help get any closer to the desired Class I molar relationship. I have learned a great deal from Dr. Sam Daher about Class II correction using clear aligners. Years ago, he taught me that a ½ cusp (≤4 mm) can be corrected with clear aligners without extraction, whereas if it is ¾ cusp or more (>4 mm), I should consider extractions or surgical correction.
Then I discovered how effectively Propel’s Excellerator drivers deliver micro-osteoperforations (MOPs). These drivers allow precise targeting of that powerful RAP effect and can be activated at my discretion. What I love about MOPs is, now I don’t always need to extract and can even avoid surgery in many instances.2 I can truly distalize with MOPs and clear aligners. If patients have third molars, they will need to be extracted, but if they are at the oral surgeon getting thirds extracted, they can quickly, comfortably, and easily get the MOPs treatment at the same time. MOPs has been clinically proven in a university trial to increase bone remodeling markers and comfortably accelerate tooth movement by over 60%.3 I routinely provide the oral surgeon a sterile open tip with my original Excellerator RT manual driver for extraction cases such as Case 1. However, I prefer and now almost exclusively use the Excellerator PT motorized driver to easily deliver faster treatments in minutes myself.
Different cases can require different approaches. I have had tremendous success closing open bites with Invisalign® and high-frequency vibration from Propel®. I’ve tried other devices but prefer the 5-minute VPro based on my own willingness to tolerate almost anything for 5 minutes, while 20 minutes seems like an eternity. So I don’t subject my patients to something I wouldn’t want to do myself. I know Case 2 is going to require excellent aligner seating,4 and any discomfort could derail compliance. VPro 5-minute daily is non-negotiable for this case, or any case with moderate (blue), or advanced (black) movements staged. Additionally, with this implant placed 1 month prior, and no abutment or final restoration fabricated, the anabolic properties of high-frequency vibration in the absence of any orthodontic force can be utilized to improve bone density.5-7
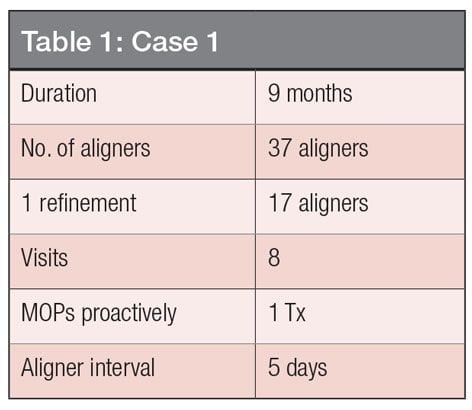
Case 1: Class II Division II
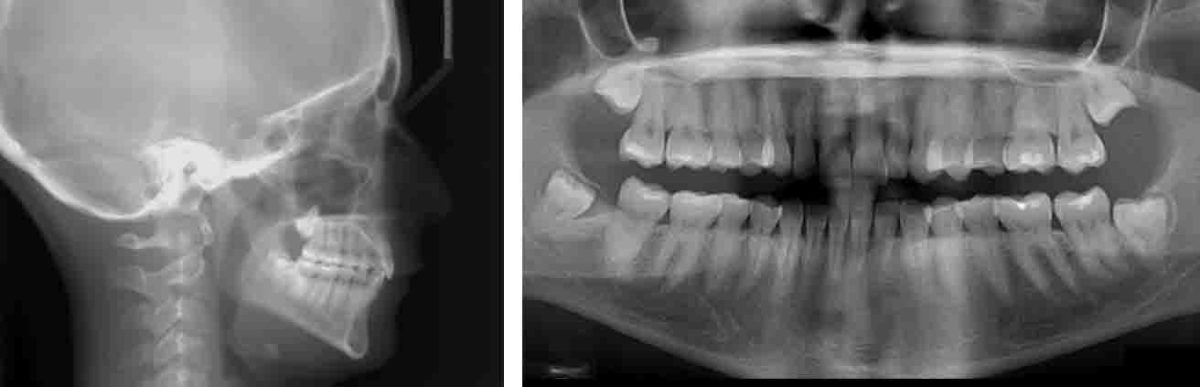
Patient is a 27-year-old female presenting with almost a full-cusp Class II. Canines are definitely a full-cusp Class II on the left (Figure 1A). All third molars are present (Figure 1B). Her chief complaint is, “I want to straighten my teeth and fix my bite.” Surgery would be required to advance the lower jaw, but she is satisfied with her profile. With no airway issues, we don’t require mandibular advancement. I can distalize this full-cusp Class II with with MOPs and aligners. Here’s how I set up my Invisalign® ClinCheck® for Class II correction: I used to put vertical attachments on the molars but tended to get posterior open bites. As I distalized and expanded, the molars sometimes began to tip. To get the back teeth to land when I finish, I now request horizontal attachments on molars and always level the curve of Spee. What I love about Class II Division II patients and targeted MOPs is, I can torque the anterior and tip them out using equal and opposite force to procline as I’m distalizing, so really I’m multi-tasking. Two maxillary MOPs were performed per interradicular space mesial of the second molar around to the mesial of the second molar. MOPs were not required distal to the second molar due to extractions. My MOPs case finishes look just like my ClinChecks and that’s what I love about MOPs. It makes my ClinChecks work like they are programmed, even at an accelerated 5-day interval with advanced movements. This adult Class II case has a great finish (Figures 1C, 1D, and Table 1) in 9 months with no bicuspid extractions and the stubborn space closures that come with them.



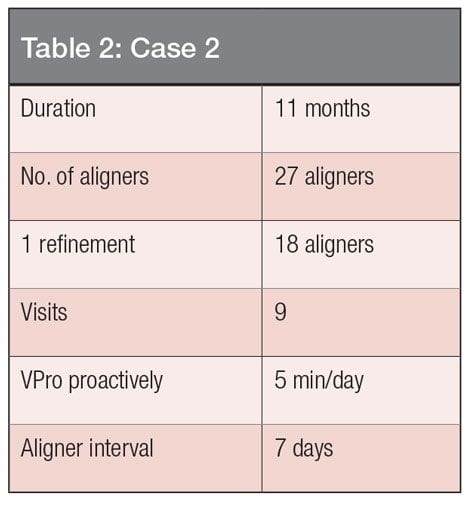
Case 2: Class II open bite with recent dental implant
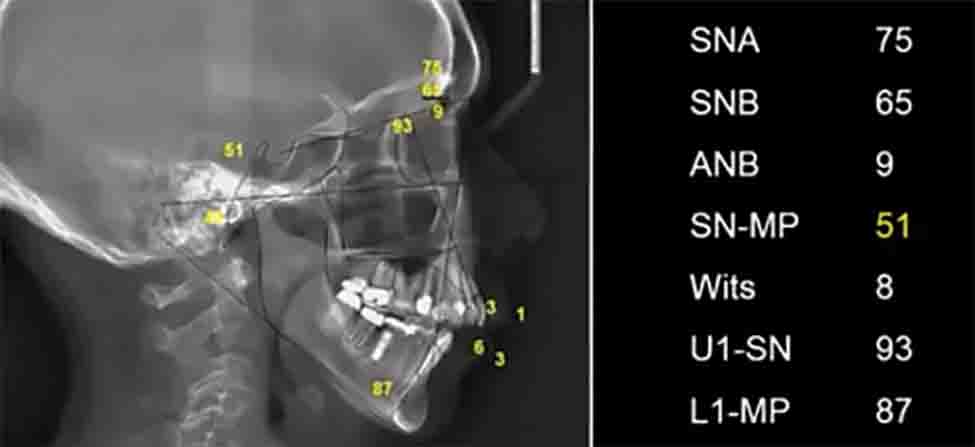
The patient is a 64-year-old female presenting with lower right tooth No. 6 extracted and implant placed (Figures 2A and 2B). Her chief complaint is, “I would really love to fix my teeth because my crowding has made it really tough to keep my teeth clean, and I just had an implant put in.” She is full-cusp Class II on the right, ½ cusp Class II on the left, and Class II canines, with a constricted maxillary arch, mandibular crowding, and open bite. She has a mandibular plane angle of 51 degrees, Wits of 8, and ANB of 9 (Figure 2C). This is a surgical case. When looking at the records on paper, many clinicians would be reluctant to treat this case, plus she has an implant. Treatment planning with fixed appliances would have been rather complex, and likely would have resulted in several additional visits to my office. However, with aligners I could simply program no movement on that space, or into that space. Additionally, the space being maintained for the abutment and crown would not look or feel as noticeable with aligners on for 22+ hours per day as it would with fixed appliances. I felt this served as a great compliance driver for this complex case. With the implant already placed, this case definitely presents a challenge. At 5 months, we can see significant progress on closing the open bite (Figure 2D). Upper molars intruded, upper incisors were extruded via IPR and relative extrusion, lower incisors were proclined 6 degrees, and the mandible was auto-rotated counter-clockwise. In addition, the lower molar came forward slightly, and the mandibular plane angle was improved by 2 degrees. Peri-implant bone density posttreatment appears healthy. This advanced case was completed with 7-day aligner interval clear aligner therapy and high-frequency VPro in 11 months and nine visits (Figures 2E, 2F, and Table 2). Typically, a case like this would require a minimum of 18 months and surgery. She is ecstatic and so happy that she can eat, smile, and keep her teeth clean. The patient said she has been waiting for this day for so many years and can’t believe there was almost no discomfort throughout her treatment. She attributes it to, and thanks me for, stressing the importance of her VPro device, which she maintains use of in retention,6-8 and to support the continued osseointegration of her dental implant.5-7





In summary, translational movements are difficult regardless of fixed or removable appliances but particularly for clear aligners. Excellerator® MOPs allow me to target the alveolar bone near the apex by making shallow perforations just above and below the mucogingival junction. The decreased bone density associated with the MOPs/RAP effect lasts for approximately 4 months1 and can be repeated if necessary.9 This simple tool provides me what I call “biological leverage” to truly distalize rather than just tip. High frequency VPro™ has clinically demonstrated faster, more predictable tooth movement, and the reduction of refinements.10 Dual, full-arch aligner seating, increased bone remodeling markers, and compliance driving immediate pain relief associated with orthodontic forces all come together to maximize treatment efficiency.4,6,10-11 High frequency was also recently shown to enhance and prolong the inflammatory response to orthodontic forces.7 This suggests their combined use may minimize the need to repeat the MOPs procedure, while supporting clinical control from crown to apex. The results of incorporating these simple and cost-effective treatment adjuncts have proven them to be invaluable skeleton keys. They are consistently unlocking some of my most profitable finishes, while delivering patients non-surgical solutions to Class II’s and doing it fast too.
Acknowledgment
The Excellerator® is the first and only device cleared by the US Food and Drug Administration (FDA) for micro-osteoperforation in orthodontic and dental operative procedures. Propel® Orthodontics markets the VPro™ series, the first and only high-frequency vibration aligner seater.
 Bella Shen Garnett, DMD, MMSc, is a graduate of Stanford University, the Harvard School of Dental Medicine, and is a Board Certified Orthodontist and an Angle’s Society Affiliate member. She runs two private practices in San Francisco and is a Diamond Plus Invisalign® provider. She lectures for both Align Technology and Propel.
Bella Shen Garnett, DMD, MMSc, is a graduate of Stanford University, the Harvard School of Dental Medicine, and is a Board Certified Orthodontist and an Angle’s Society Affiliate member. She runs two private practices in San Francisco and is a Diamond Plus Invisalign® provider. She lectures for both Align Technology and Propel.
Disclosure: Propel® Orthodontics provided support to the author.
- Kantarci A, Will L, Yen S, eds. Tooth Movement. Front Oral Biol. Basel, Switzerland: Karger Publishers; 2016.
- Raptis M. Micro-Osteoperforation as an Adjunct for the Correction of Negative Anterior Overjet in an Adolescent Patient with Missing Upper Lateral Incisors. J Clin Orthod. 2017;51(1)47-153.
- Alikhani M, Raptis M, Zoldan B, et al. Effect of micro-osteoperforations on the rate of tooth movement. Am J Orthod Dentofacial Orthop. 2013;144:639-648.
- Shipley T. VPro5™ —more efficient aligner seating with high-frequency vibration. Orthodontic Practice US. 2016;7:5.
- Alikhani M, Khoo E, Alyami B, et al. Osteogenic effect of high-frequency acceleration on alveolar bone. J Dent Res. 2012;91(4):413-419.
- Alikhani M, Sangsuwon C, Alansari S, Nervina JM, Teixeira CC. High Frequency Acceleration: A New Tool for Alveolar Bone Regeneration. JSM Dent Surg. 2017;2(4):1026.
- Alikhani M, Alansari S, Hamidaddin MA, et al. Vibration paradox in orthodontics: Anabolic and catabolic effects. PLoS One. 2018;13(5).
- McFarlane B. Manual osteoperforation and high-frequency vibration. Orthodontic Practice US. 2017.
- Nicozisis JL. Applications of controlled local inflammation in aligner treatment. Semin Orthod. 2017; 23:90-98.
- Shipley TS. Effects of High Frequency Acceleration Device on Aligner Treatment—A Pilot Study. Dent J. 2018;6(3):32.
- Brigham G. Accelerated treatment modalities in clear aligner treatment. Ortho. 2018;1:30-37
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
