Drs. Silmon and Cosse describe avoiding surgery and offering a patient alternatives that resulted in a successful outcome of treatment.
Drs. Jeffrey Silmon and Chris Cosse devise a treatment plan that avoided certain surgical disadvantages
Introduction

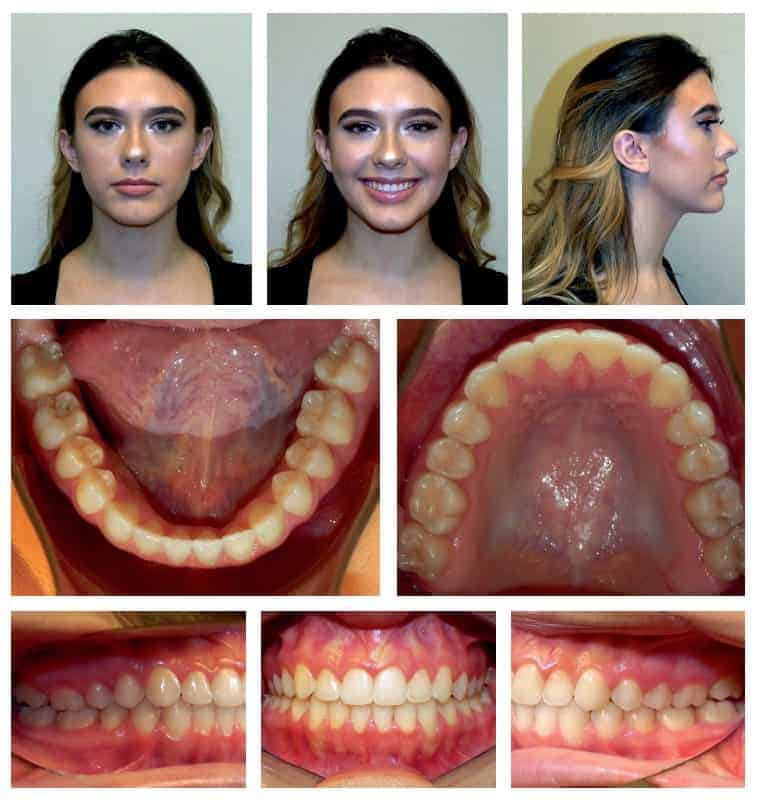
Several years ago, a 14-year 10-month-old female named Caroline presented to our office with a hypoplastic maxilla, a hyperplastic mandible, and a complete crossbite of her entire arch except for the lower right first and second molars. She had retained deciduous upper cuspids, and her permanent cuspids had erupted facially. Caroline was having clicking and popping bilaterally with occasional pain. She also presented with narrow buccal corridors. She was being teased because of her prominent chin and prognathic mandible. Although she did have a slight CR/CO slide, we felt that due to the severity of her AP discrepancy that a surgical plan would be ideal.
After a consultation with an oral surgeon, everyone agreed that a maxillary advancement and a mandibular setback was ideal. Then came the bill. The financial burden, required healing time, and potential surgical risks were too much to overcome, so her parents asked us to devise a nonsurgical plan. We used Braces Academy videos to educate her before treatment for informed consent and to explain different treatment plans. Braces Academy videos were used during treatment for compliance, turning the RPE, and brushing instructions; and after treatment they were used for retention instructions and for taking care of her retainers. These videos are unique because they are prescriptive, meaning they are sent from a library of content and sent to patients via email or text so that they receive exactly what they need, exactly when they need it, without having to search through vast amounts of extraneous information. The software also lets the orthodontist know if patients didn’t watch the content that the office sent.
Treatment
We elected to start with expansion using a Hyrax appliance to perform rapid palatal expansion due to her skeletal age, as determined by a hand/wrist radiograph. We determined one turn per day for a total of 6 weeks. As a result, we gained 8.5 mm of expansion at the maxillary first molars. At that point, we bonded the case using Ormco Damon® Q™ brackets. We used low torque for upper incisors and canines, standard torque for lower incisors, and high torque for lower canines. The torques were chosen to fight the inevitable upper incisor flaring and lower incisor retroclination that occurs with long term Class III elastic use.
Her bite opened significantly with the expander due to the change in contacts of the incline planes and the inevitable flaring from the expander. Additionally, we used posterior bite turbos to disarticulate the bite, regain control of the torque on the upper first molars, and help close it back down.

Early elastic protocol was used, and the patient was instructed to wear upper 4-6 to lower 3-4 Fox elastics for at least 20 hours per day, changing them regularly. She and her parents were told that her elastic wear was very important in the effort to avoid surgery. She was also warned that noncompliance would make her much more likely to need orthognathic surgery. The wire sequence we used was Ormco .014 Damon arch form Copper NiTi U/L, Ormco .014 x .025 Damon arch form Copper NiTi U/L, Ormco .018 x .025 Damon arch form Copper NiTi U/L, and Ormco .019 x .025 Damon arch form stainless steel U and .017 x .025 Damon arch form stainless steel L. Our alternative plan, if the patient was noncompliant with elastics, was one of the Class III extraction patterns.

Outcome
After 6 months of treatment, Caroline appeared to be compliant with elastics, and the AP molar and canine relationships were improving. We were able to finish her case without extractions and with elastic compliance alone. She wore her elastic so
well that her bite actually over-corrected at some point during treatment. Twenty-five months and 13 appointments after her initial bonding, we debonded and delivered U/L clear overlay retainers.
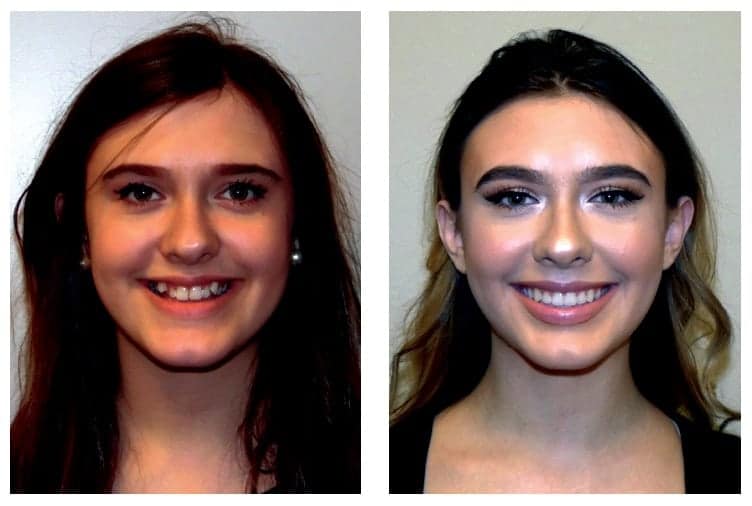
We were surprised at her results. We felt confident that we could make
her better, but the results turned out better than we expected. Looking back, our original surgical plan might not have turned out this successfully! We reached all of our goals for Caroline. We corrected her crossbite, filled her buccal corridors, and corrected her AP discrepancy, improved her smile arc, while improving her profile characteristics and overall esthetics. We guarantee that she isn’t being teased anymore. Her bite is stable, her clicking and popping has resolved, and she is compliant with her U/L clear overlay retainers. The final records are 2 years after debond. Caroline says, “I am much more confident with my new smile, and I’m happy with how nice my teeth look now.”


Avoiding surgery for correction of Class III malocclusions is the topic of this article by Dr. Suhail Khouri. Read about it here.
https://orthopracticeus.com/ce-articles/using-v-bends-niti-wires-nonsurgical-correction-class-iii-malocclusions.
 Dr. Jeffery Silmon, DDS, is a graduate of Louisiana State University School of Dentistry, and he completed his orthodontic training there as well. He is the past president of the Northwest Louisiana Dental Association (NWLDA), and is a Damon Premier Provider and Educator. Dr. Silmon is married and has two children. He is in private practice in Shreveport, Louisiana.
Dr. Jeffery Silmon, DDS, is a graduate of Louisiana State University School of Dentistry, and he completed his orthodontic training there as well. He is the past president of the Northwest Louisiana Dental Association (NWLDA), and is a Damon Premier Provider and Educator. Dr. Silmon is married and has two children. He is in private practice in Shreveport, Louisiana.
 Dr. Christopher Cosse, DDS, is a graduate of Louisiana State University School of Dentistry, and he completed his orthodontic training at Oregon Health Science in Portland. He is regularly invited to speak about orthodontics nationally and internationally. He is married and has four children. He is a Damon Premier Provider and Educator and is in private practice in Shreveport, Louisiana.
Dr. Christopher Cosse, DDS, is a graduate of Louisiana State University School of Dentistry, and he completed his orthodontic training at Oregon Health Science in Portland. He is regularly invited to speak about orthodontics nationally and internationally. He is married and has four children. He is a Damon Premier Provider and Educator and is in private practice in Shreveport, Louisiana.
Disclosure: Dr. Cosse is the founder of Braces Academy – The prescriptive patient education™ system
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
