Dr. Edward Lin discusses efficient and effective digital innovations
Earlier this year, I followed the groundbreaking thought leadership that came out of the Davos World Economic Forum in Switzerland, and I found that the theme of the event, “Mastering the Fourth Industrial Revolution,” was an accurate description of my treatment philosophy. The fourth industrial revolution is the notion of blurring the boundaries that separate physical, digital, and biological spheres.
[userloggedin]
Typically, patients want orthodontic treatment because they are seeking the perfect smile or long-term relief from health challenges such as sleep apnea, TMJ pathology, occlusal breakdown, or worn dentition as a result of patients living longer. It’s obvious that these scenarios touch on the biological and physical spheres, and now we have digital innovations that enable orthodontists to better deliver quality results efficiently and effectively.
I practice alongside three orthodontists at two practices in Wisconsin — Orthodontic Specialists in Green Bay and Apple Creek Orthodontics in Appleton. Together we’ve beta tested and have been early adopters of innovative, disruptive, and transformative technologies that have changed our profession. My passion for technology stems from my enthusiasm to create healthy and beautiful smiles for patients and to far exceed their expectations of orthodontic treatment. The key to this is constantly evaluating new technologies that are introduced to orthodontics on the basis of safety, effectiveness, and how seamlessly they integrate into my current standard of care in clinical practice.
These two case studies highlight technologies that have had a major imprint on delivering more predictable and desirable results. Technologies such as AcceleDent®, i-CAT™ FLX, 3D printers, temporary anchorage devices (TADs), and the suresmile® digital software have evolved the way that I practice orthodontics. I’ve studied each of these individually and how they work in tandem with each other to deliver precise results the first time.
CBCT
Precision starts with having a very clear picture at the beginning that dictates where you want and need to end. Without a doubt the i-CAT FLX has revolutionized digital treatment planning through cone beam computed tomography (CBCT) that involves the shortest scan time and lowest radiation dose. CBCT 3D imaging gives us the most comprehensive views for evaluating airway, TMJ imaging, eruption paths, bone and nerve anatomy, and root positions that we just cannot see and evaluate with 2D imaging. In my opinion, I believe that 3D imaging should be the standard of care, especially with the availability of low-dose CBCT scanners.
Cone beam technology is invaluable when evaluating patients who have the risk for obstructive sleep apnea syndrome (OSA) as is the case with Patient 1. Orthodontists are seeing an increase in patients who have potential airway restriction. An American Journal of Orthodontics and Dentofacial Orthopedics article detailed how CBCT can assess the dimensional changes of the upper airway in patients whose maxillary constrictions are being treated with rapid palatal expansion appliances (RPE).1 The study demonstrates from the CBCT that the cross-sectional area of the upper airway at the posterior nasal spine to basion level significantly gains a moderate increase after RPE. Orthodontists are in a unique position with having the opportunity to evaluate younger patients who may be at a higher risk for OSA. Treatment for airway restrictions is much more effective when patients are diagnosed and treated at an early age, so I encourage orthodontists to leverage this advanced CBCT technology and collaborate with their local pediatricians and dentists.
Digital impressions and 3D printing
My colleagues and I have been striving toward 100% digital-impression dentistry. It’s better for patient comfort, there’s no powder, and it’s not messy. With our intraoral scanner (3Shape TRIOS®), there’s never a need for retakes, which creates efficiencies by saving chair time. It also offers enhanced precision. Patient 2 in this case study was one of our aligner patients who benefitted from this efficiency and precision. Since we have our own EnvisionTEC Perfactory® Micro and Perfactory® Vida 3D printers, we upload the digital intraoral scan to the suresmile cloud, create the virtual digital occlusal treatment plan, and then send to our in-house lab to 3D print the aligner trays. This all happens in-house. It’s a major efficiency that allows us to save on shipping costs, lab material, and payroll expenses, and it also helps ensure continuous patient engagement and motivation from the consult to their start date.
Accelerated treatment
When we talk to patients about all of the technologies that we use in our office for their orthodontic treatment, they are impressed, but they still want to know how long is it going to take, and if it’s going to hurt. They are intrigued and excited when we tell them about AcceleDent and how the device’s SoftPulse Technology® has been clinically proven to speed up orthodontic treatment by as much as 50% while also relieving discomfort.2,3 I’ve researched other accelerated treatment technologies, but ultimately decided to continue offering AcceleDent because patients say it makes their teeth feel better.2 The reduction in discomfort that AcceleDent gives patients is the differentiator among the current accelerated technologies.
Since we’re putting AcceleDent into the hands of the patients and asking them to use it for 20 minutes a day throughout treatment, it’s important that orthodontists explain to patients the science of how it works. We underscore that AcceleDent is the first and only FDA-cleared vibratory orthodontic device that uses gentle vibrations to accelerate bone remodeling at the cellular level. The prescription-only device is cleared for use in conjunction with brackets or aligners. We also explain to patients that the SoftPulse Technology employs 25 grams of force at 30 Hz, which is 200 times less force than ordinary chewing.
We evaluate compliance throughout treatment with our accelerated patients by asking them to bring their AcceleDent units with them to appointments, so that we can view the FastTrac Usage Report that’s available via the USB charging port. Compliance is a non-issue for these patients because they want to complete treatment as fast as possible with no pain.
Blending technologies in practice
The following case studies illustrate how patients treated with the latest advancements in orthodontic technologies can achieve quality finishes with an accelerated treatment plan.

Patient 1
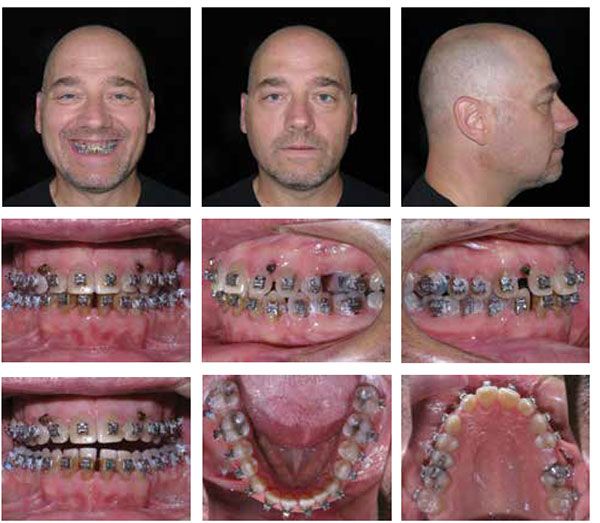
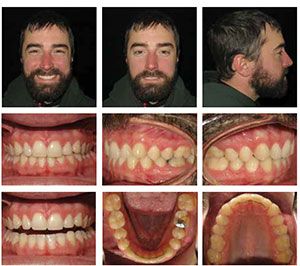
The patient presented at his new patient examination on December 4, 2012, as a 47-year 3-month-old adult male. He was referred to our office by his dentist due to concerns with a Class III malocclusion, gingival recession, and incisal wear, which had developed as a result of a dental sleep appliance that had been made by his sleep specialist. The patient’s sleep apnea was diagnosed 10 years prior. For the first 2 years, the patient’s sleep apnea was being treated with continuous positive airway pressure (CPAP) therapy, which he was not tolerating well. The patient was concerned about his “uncomfortable” bite and that his teeth were beginning to chip. His diagnosis in my office determined that he was a Class III with generalized maxillary and mandibular spacing (Figure 1).
Treatment plan
The patient was given two options for treatment. The first and ideal option consisted of treatment with full-fixed orthodontic appliances in combination with two-jaw maxillary and mandibular advancement surgery for Class III correction and to increase his airway volume for correction of his OSA. The second option consisted of treatment with full-fixed orthodontic appliances in combination with temporary anchorage devices (TADs). I use TADs for all of my nonsurgical Class II and Class III cases because they provide us with control that we previously did not have in orthodontics. TADs give us skeletal anchorage instead of dental anchorage with excellent control of the direction and vectors of forces utilized with them.



I estimated treatment time of 36 months due to the complexity of his case, but suggested his treatment length could be closer to 24 months if he used AcceleDent. The patient chose AcceleDent to minimize the length of treatment. His treatment was actually completed in 21 months.
Treatment summary
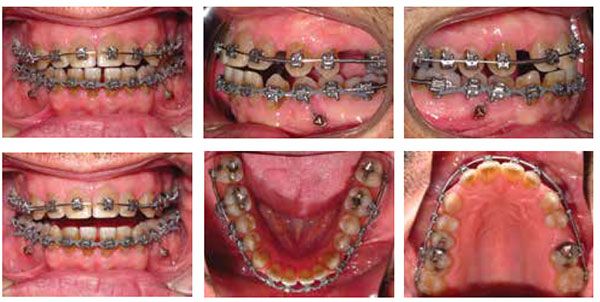
On the patient’s full-bonding appointment, we placed labial brackets 7-7 and bilateral TADs (8 x 1.4 mm) in the mandibular arch distal to the first bicuspids. The TAD was tied with a steel ligature tie to his lower first bicuspids for anchorage in distalizing the L7s only not the L5s and L6s (Figure 2). Active open coil springs were placed distal to the upper laterals and distal to the lower first molars. A closed coil spring was placed distal of UL5. The patient was instructed to wear Class III elastics full time and use his AcceleDent unit for 20 minutes daily.
Since the patient was using AcceleDent, I let the wire express for about 8 weeks before I brought him in for his second appointment. Before accelerated treatment, I would have to wait 10 weeks before checking on hygiene, elastic wear, and bracket placement and then wait another 10 weeks for the wires and open coil springs to fully express themselves.
As space was redistributed in the maxillary arch, I placed TADs distal to the upper laterals to help protract his posterior teeth forward in the maxillary arch (Figure 3). Ten weeks later, I repositioned his mandibular TADs so they were mesial to the lower second molars and continued to facilitate retraction in combination with elastics. Approximately 15 weeks later and 12 months from starting treatment, we removed all TADs and submitted a supplemental scan of all four quadrants to suresmile (Figures 4 and 6). There’s a noticeable difference with AcceleDent that allows me to do the virtual wire bends in the suresmile software sooner, eliminating an appointment and overall completing the case faster.
On January 27, 2015, and 18 months into total treatment time, we ordered his final finishing wire through the suresmile software with virtual bends for space closure and overjet.
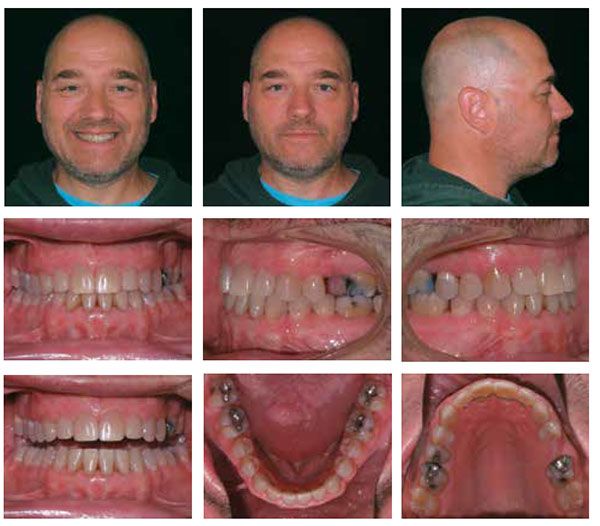
On April 21, 2015, we debonded his brackets and placed bonded lingual retainers upper 2×2 and lower 3×3 (Figure 5). Total treatment time for this patient was 21 months with a total of 15 appointments from the initial bonding appointment to his debond appointment (Figure 7).
Understanding he chose to pursue treatment nonsurgically and that it wasn’t treating his OSA, the patient elected to resume CPAP therapy.
Patient 2
The patient was first seen in our office on March 15, 2014, as a healthy 30-year 5-month-old adult male who was about to get married in September. Prompted by his fiancée, he wanted straighter teeth and needed treatment to be completed in time for their wedding photos. Upon exam, he presented as Class I with mild spacing (Figure 8). He had been treated prior with orthodontia, but hadn’t worn his retainers.

Treatment plan
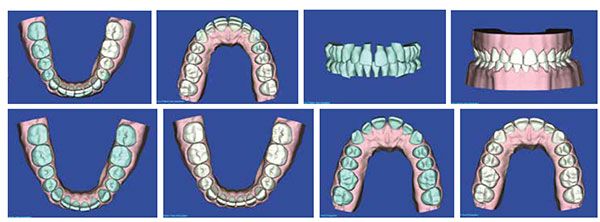
The patient was interested in only aligners for treatment, so we planned and created his aligner trays virtually using suresmile’s aligner design software. Prior to finalizing his aligner treatment plan, I did a minor amount of IPR in the lower arch from L5-5 to address his mandibular excess as seen through the software in his Bolton analysis.
His initial set of trays was planned for 14 aligners in the maxillary arch and nine aligners for the mandibular arch (Figure 11). Without AcceleDent, I have my aligner patients changing aligner stages every 2 weeks, putting his estimated duration for treatment in the 7-month range and beyond his goal for completion. With a significant milestone to complete treatment in 5 months or less, the patient was highly motivated to use AcceleDent and changed aligner stages every 7 days, which is my general protocol for aligner change frequency for my AcceleDent patients.

Treatment summary
Approximately 1 month after being seen for his initial exam, the patient was seen for his first aligner delivery appointment. At this time, we seated stage 1 of his upper and lower aligners and gave the patient aligners 2-6 (Figure 9). When I fit patients for the aligners, I trim them a little longer past the gingival margins so that there is better retention or a natural undercut of the cemento-enamel junction (CAJ). The patient was instructed to change aligners to the next sequential stage every 7 days and use his AcceleDent unit for 20 minutes daily. His next appointment was scheduled for 6 weeks to check progress.

In the patient’s second appointment 6 weeks later, we checked the progress of his stage 6 aligners, and being satisfied with the progress, gave him the remaining aligners planned for his initial phase prior to any refinement, which included aligners 7-14 for the upper arch and 7-9 for the lower arch. The patient was instructed to continue to change aligners to the next sequential stage every 7 days and use his AcceleDent unit for 20 minutes daily.
In the patient’s third appointment 4 weeks later, we checked the progress of his upper arch and evaluated the results in his lower arch as he was on his final stage (Figure 10) in the initial aligners planned for that arch. We created a refinement aligner for the lower arch to place the lower centrals 0.2 mm lingually and to tighten spaces by 0.2 mm, and this could be done through the software and without additional scans or impressions. The patient was instructed to continue to use his AcceleDent unit for 20 minutes daily and to change aligners to the next sequential stage every 7 days for the upper arch and to continue to wear stage No. 9 in the lower arch until his next appointment.
At his fourth appointment on July 29, 2014, we delivered his refinement aligner for the lower arch and determined his upper arch on stage 13 was tracking nicely. His next appointment was scheduled for 2 weeks to evaluate final aligner stage results.
Two weeks later on August 12, 2014, and less than 4 months from starting treatment, the patient’s treatment was complete, and we finished a month ahead of his goal to be done by his September wedding! I did some re-contouring of his anterior teeth for esthetics at this appointment. I generally do any reshaping of teeth after the aligners have been worn to completion so that I have as much surface area possible for the aligners to grasp during the treatment period.
I’ve noticed that AcceleDent has enhanced the quality of my aligner therapy patients because the bone remodeling caused by the SoftPulse Technology helps better seat the teeth into the aligner trays. In addition to acceleration, AcceleDent offers enhanced predictability and precision.
With AcceleDent, this patient finished treatment in 3 months and 3 weeks. We used direct bond lingual retainers for the U 2-2 and L 3-3 for retention (Figure 12). Our total treatment costs for this aligner treatment approach was approximately $350. suresmile’saligner design software also gives us complete control throughout the treatment period to make modifications as needed.
Conclusion
Accelerated orthodontics, 3D imaging, and 3D digital orthodontics are the future of our profession, and these technologies are at our fingertips. The goal is to embrace technologies that make sense for your practice. For us it’s CBCT, suresmile, TADs, and AcceleDent. Technology should be unique to each individual practice and orthodontist based on treatment philosophy, standard of care for that practice, and the typical cases that are referred. Orthodontists are sought after as the premier leaders in the dental field, so the burden is on us to investigate orthodontic advancements. We have to collaborate as we evaluate technologies on the basis of safety, effectiveness, and how well they integrate into our practices.
I know I’m a better orthodontist because of the technologies that we’ve integrated into our practice, and I’m confident that my clinical results prove that these innovations yield a much higher quality of care, a more efficient practice, and increased patient satisfaction. The bonus is that I also find greater enjoyment practicing orthodontics because of them.
[/userloggedin]
[userloggedout][/userloggedout]
 Edward Lin, DDS, MS, is a respected orthodontic lecturer who practices at Orthodontic Specialists in Green Bay, Wisconsin, and at Apple Creek Orthodontics in Appleton, Wisconsin. A member of the American Dental Association, the American Association of Orthodontists, and the World Federation of Orthodontists, Dr. Lin is passionate about orthodontics and being an early adopter of technology that makes treatment more enjoyable for patients and orthodontists. He completed dental school and orthodontic residency at Northwestern University and has been in private practice since 1999.
Edward Lin, DDS, MS, is a respected orthodontic lecturer who practices at Orthodontic Specialists in Green Bay, Wisconsin, and at Apple Creek Orthodontics in Appleton, Wisconsin. A member of the American Dental Association, the American Association of Orthodontists, and the World Federation of Orthodontists, Dr. Lin is passionate about orthodontics and being an early adopter of technology that makes treatment more enjoyable for patients and orthodontists. He completed dental school and orthodontic residency at Northwestern University and has been in private practice since 1999.
Disclosure: Dr. Lin has no conflicts of interest to report.
- Chang Y, Koenig LJ, Pruszynski JE, Bradley TG, Bosio JA, Liu D. Dimensional changes of upper airway after rapid maxillary expansion: a prospective cone-beam computed tomography study. Am J Orthod Dentofacial Orthop. 2013 Apr;143(4):462-270.
- Pavlin D, Anthony R, Raj V, Gakunga PT. Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A double-blind, randomized controlled trial. Seminars in Orthodontics. 2015;21(3):187 –194.
- Lobre WD, Callegari BJ, Gardner G, Marsh CM, Bush AC, Dunn WJ. Pain control in orthodontics using a micropulse vibration device: A randomized clinical trial. Angle Orthod. 2106;86(4)625-630
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
