CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This clinical article aims to discuss the application of several three-dimensional maxillary expander appliance variations and benefits in the initial stage of maxillary arch development with arch-length gains using each of these designs.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article.
Take the quiz by clicking here.
Correctly answering the questions will demonstrate the reader can:
- Recognize how this modernized 3-Way maxillary arch expander can accomplish differential molar distalization, intrusion/extrusion and rotational movements.
- Recognize how this device can facilitate molar root uprighting distally.
- Realize the device’s molar extrusion/intrusion capabilities.
- Identify the asymmetric movement capabilities within each quadrant.
- Realize this expanders’ capabilities to individualize movements, so each quadrant can differentially move in three dimensions to correct transverse, Class II, midline, and occlusal plane variations.

Dr. Duane Grummons discusses naso-maxillary orthopedic 3-dimensional expander techniques to overcome structural form discrepancies of the maxillae, having dentoalveolar compensations

The objectives of this article are to share several clinical design innovations with key clinical information for the effective and successful implementation of the selected 3-Way expander appliance design in various maxillary arch conditions. This article shows the application of several appliance variations and their three-dimensional benefits in the initial stage of maxillary arch development with arch-length gains.
These 3-Way maxillary orthopedic appliances overcome structural form discrepancies1 having dentoalveolar compensations. The 3-Way appliance began in the 1980s with the G-Rax expander (Bevins Lab, Leone Orthodontics, AOA Lab, Space Maintainers Lab), which matured into today’s 3-Way 3-dimensional Smart Click appliance (Great Lakes Orthodontic Dental Technologies).
Any discussion regarding noncompliance fixed jaw (orthopedic) or arch development (dentoalveolar expansion) therapeutic approaches must credit and hugely acknowledge the long-standing appliance contributions by Dr. James Hilgers (i.e., Pendulum, T-Rex, Pendex)2,3 and others.4,5,6 Earlier versions of the 3-Way appliances appeared in my nonextraction noncompliance publications.4 The 3-Way can also be a key maxillary orthopedic appliance therapy for pediatric breathing disorders/functional airway issues.
Initially, the 3-Way appliance is placed in the mouth passively to confirm ease and accuracy of fit and then sealed into position. The appliance molar springs are mildly activated 15 degrees distally as expansion turns begin. These turns are slow, so sutural regions are stimulated over a longer time for best orthopedic benefits and with less buccal and distal tipping of posterior teeth. This longer time achieves the molar distalization with uprighting movements. Typically, the expansion turns are one turn every 2 days (slow expansion protocol) for approximately the first 20 turns. Thereafter, the turn rate slows to one or two turns per week until expansion target is reached. Five or more turns can be added for width overcorrection at a pace of one turn per week while the molar roots continue derotating with distal molar root uprighting to the treatment objective.
3-Way capabilities include:
- transverse gains in maxillary basal structure and intemolar widths
- molar derotation with distal translation
- occlusal plane improvement by molar extrusion or intrusion
- asymmetric movements possible with differential activations of the molar loops/springs
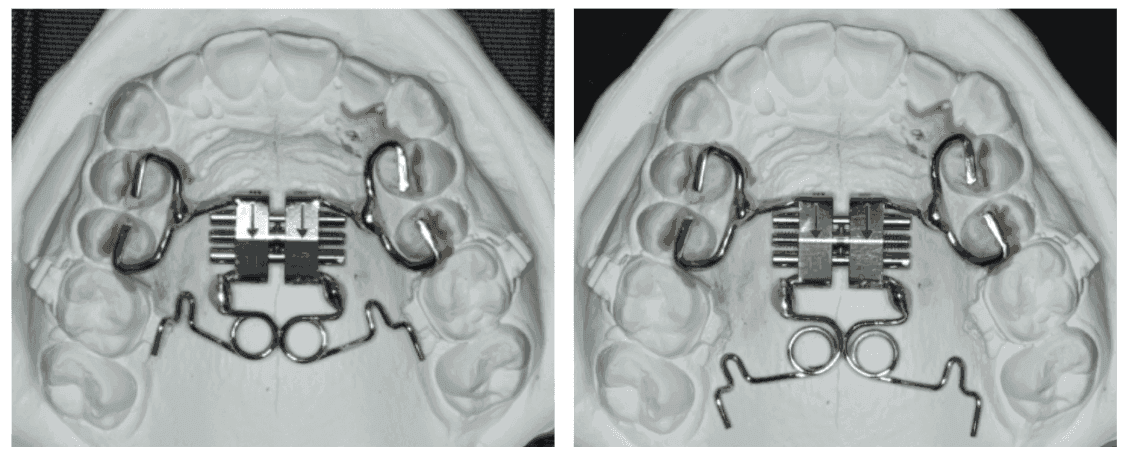
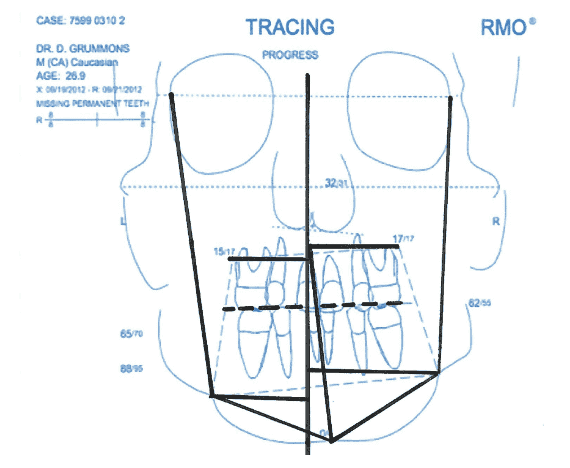
These springs can be soldered or laser-welded to the screw and molar bands. At the screw, the soldered design can be used, though high heat could affect the screw mechanism, so laser-weld-to-screw is preferred. The .032-inch spring can either be soldered to the lingual region of the molar bands or be inserted into an .036-inch welded sheath. This sheath method is preferred at the screw and molars, so the spring can be disengaged and activated for first molars’ distal (de)rotation, distal movement, differential expansion or constriction, molar eruption or intrusion (occlusal plane leveling), and/or for distal tip/uprighting of molar roots. The frontal analysis specifies these treatment objectives.12,13

To reactivate at the molars, the spring is disengaged, and the helix is gripped with either a Howe/Weingart plier or a heavy-locking hemostat plier. The spring arm is bent and (re)activated distally by 20-30 degrees beyond the molar sheath and re-engaged into the molar sheath — less activation when the appliance is first inserted. Subsequent activations can be applied unilaterally to one first molar, and the next visit for the opposite first molar. This approach is more anchorage-efficient (a less reciprocal effect) and accomplishes more molar distal rotational movement with true molar translation distally. The spring activations are intentionally light (approximately 120 gm per molar), which is consistent with the root ratings forces to accomplish molar derotation and distal root relocation/translation with root uprighting. Overactivation of springs will result in some undesired mesial movement of premolars. The solution is to apply lighter molar spring activations.
Asymmetric movements of molars are possible with specific derotation, differential extrusion or intrusion (occlusal plane leveling), distal root translation with molar uprighting achieved based upon bends placed in loops, and sheath arms of molar spring wires. Think in three planes of space like aeronautics: tip, yaw, and roll.
Maxillary first molars become distalized with root apices of first molars/second premolars distinctly moved apart from each other, indicating true molar distal rotation/relocation/uprighting. The 3-Way appliance is left in place for 2-3 months after final turns or spring activations to accomplish stabilized maxillary orthopedic changes in three dimensions with effective molar root uprighting and stability as confirmed by research.4, 7, 8, 9, 14
The horizontal loop by molars is directed anteriorly and can be widened to cause that molar to extrude or be shaped smaller/narrower to cause that molar to become intruded. This is done to level the occlusal plane. It is preferred to activate only one molar vertically (alternate right and left side) for efficiency of extrusion or intrusion movement. Extrusion of a molar (1 mm-3 mm) is more predictable than intrusion. Light forces over time are indicated to achieve the desired occlusal plane changes. When more intrusion (3 mm-4 mm) of maxillary first molars are planned, it becomes indicated to place a buccal TAD in maxillary first molar region and tied to the first molar being intruded. For a maxillary first molar to be extruded (3 mm-4 mm) significantly, a TAD can be placed in the lower molar region to connect this TAD to the maxillary molar needing extrusion to achieve the treatment objective for occlusal plane change.
This 3-Way appliance provides benefits before fixed brackets or clear aligners to first unlock the malocclusion10,11 by transverse/width and arch-length gains with transverse structural and arch space-gaining procedures.
Arch-length analysis should be recomputed after the maxillary orthopedic and arch development are completed, so less deficiency will be evident, and visualized treatment plan (VTP) will reflect improved conditions and case requirements to convert a crowded arch into nonextraction status.
3-Way pre-aligner: Unlocking before clear aligners
After 3-Way appliance influences, the arch shows transverse/perimeter expansion, molars distalized and derotated, arch length gained to accommodate crowded/rotated teeth, with a nonextraction orthodontic approach with efficient and predictably successful clear aligner treatment. This stage of progess represents an excellent transition stage when the 3-Way is removed, and the case is intraorally scanned to initiate the aligners process to complete the orthodontic correction.
Asymmetric 3-Way Maxillary appliance
Each half of the maxillary arch requires diagnosis12,13 for specific and differential movements to create and establish bilateral symmetry with arch uniformity. As a clinician views/inspects the maxillae and upper arch morphology, it becomes obvious that the buccal segment on one side of this arch may require more expansion or more distal molar rotation. Thus, asymmetric first molar activations achieve arch perimeter and intra-arch changes until both halves of this arch become symmetrically aligned.4,12,13
3-Way sideways screw maxillary space-gainer
The palatal screw (Smart Click) is placed sideways, with an acrylic Nance Button added directly in the mouth utilizing light-cure Triad® (Dentsply Sirona) or similar adhesive material.
Incisors can be bracketed with a utility arch to position the upper incisors in place during 3-Way appliance therapy to locate upper anteriors optimally for best smile display and lip/smile relationship prior to clear aligners. The esthetic and functional outcome is superior when upper molar(s) position(s) and optimal incisors placement are established reasonably well prior to the clear aligners for optimally finishing the case.
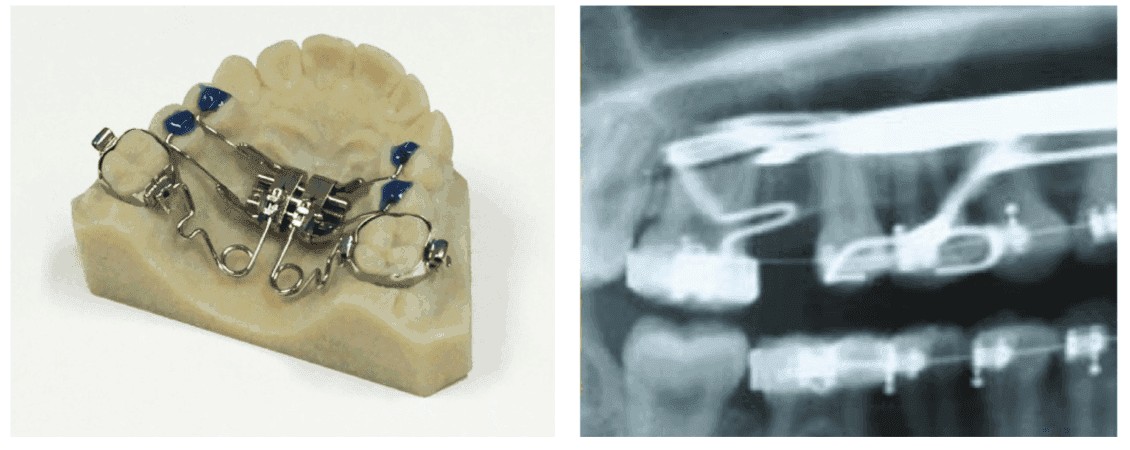
Figure 6: The 3-Way appliance is used in initial stage of full-fixed orthodontics, with a utility arch next to locate upper incisors in smile (left), Figure 7: Utilizing 3-Way appliances for 4-6 months will accomplish important sutural, dento-alveolar, and/or arch changes so that subsequent clear aligners for finishing are made routine with an exceptional clinical outcome (right)
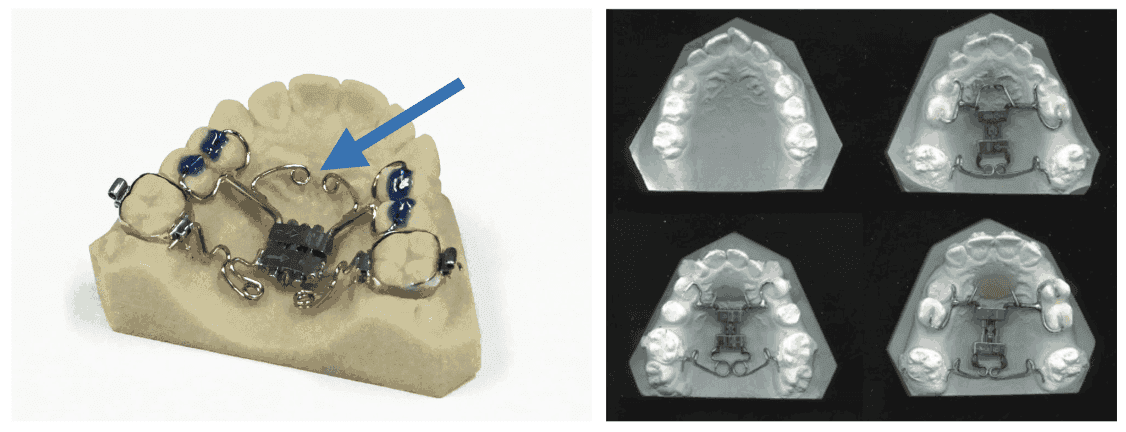
Figure 8: Optimal expansion and first molars distal movements accomplished. This is good stage to convert to clear aligners (left) and Figure 9: 3-Way appliance with unilateral arch development features (right)
Quad-Helix follows 3-Way Expander phase
A pre-formed quad-helix (Ricketts, Rocky Mountain Orthodontics) is placed upon removal of the 3-Way appliance. This quad is removed from packaging, shaped directly in the mouth using lingual arch forming pliers (2 beaks grip the quad-helix on molar insertion arms to maintain form and torque) and while viewing the upper occlusal photo to match the existing molar rotation, width, and palatal morphology.15 This quad-helix requires .072 molar sheaths and can hold the molar A-P, vertical and lateral molar positions and arch form. Also, this quad-helix can be activated to accompish further desired changes in maxillary arch form, molar positions in 3 dimensions, and serve as orthodontic anchorage for the ongoing treatment process.


Concluding remarks
The patient should triumph after treatment with optimized function, elevated self-confidence, optimal facial structural harmonies, optimized breathing/sleep conditions, with a wide radiant smile.
This 3-Way appliance achieves significant maxillary structural and dentoalveolar improvements on the pathway to efficient fixed orthodontic appliances, or full treatment with synchronized clear aligners to completion. Wisdom is knowing these 3-Way game-changers and what to do with them.
Author’s note: This article is not intended to be a case study. Case studies require many photos, X-rays with superimpositions, and appliance pictures through each stage of treatment from start through finish. These would greatly expand the article without adding benefits about the advantages of utilizing these 3-Way pre-aligners appliances initially. This article shows various appliance designs and their effectiveness.
After reading about the 3-Way maxillae expander appliance, read Dr. Larry White’s article on the vertical dimension of the maxilla and mandible and remedies for controlling the effects of too much vertical dimension. Read the article here.
Author Info
 Duane Grummons, DDS, MSD, is board-certified in facial orthopedics and orthodontics and has authored and lectured for over 35 years. His Facial Frontal Analysis and facemask orthopedic appliance innovations are extensively utilized. He is a leader in adolescent airway analyses and “earlier” (ages 2-8 years) facial orthopedic interventions for breathing/airway with life-changing benefits. His individualized pre-aligner therapy approaches and nonextraction methods are widely applied. Dr. Grummons is Associate Professor of Orthodontics at The Loma Linda University Medical Center Orthodontic Department, San Bernardino, California. He developed two efficient and productive practices — first in Marina del Rey, California, and again in Spokane, Washington. He has appeared before orthodontic, dental, and medical conferences, and made radio and TV appearances. Dr. Grummons can be reached at grummons@me.com, or visit drgrummons.com.
Duane Grummons, DDS, MSD, is board-certified in facial orthopedics and orthodontics and has authored and lectured for over 35 years. His Facial Frontal Analysis and facemask orthopedic appliance innovations are extensively utilized. He is a leader in adolescent airway analyses and “earlier” (ages 2-8 years) facial orthopedic interventions for breathing/airway with life-changing benefits. His individualized pre-aligner therapy approaches and nonextraction methods are widely applied. Dr. Grummons is Associate Professor of Orthodontics at The Loma Linda University Medical Center Orthodontic Department, San Bernardino, California. He developed two efficient and productive practices — first in Marina del Rey, California, and again in Spokane, Washington. He has appeared before orthodontic, dental, and medical conferences, and made radio and TV appearances. Dr. Grummons can be reached at grummons@me.com, or visit drgrummons.com.
Disclosure: Dr. Grummons has neither financial interests nor conflicts regarding the appliances mentioned in this article. He lectures at conferences sponsored by Great Lakes Dental Technologies and for Rocky Mountain Seminars, and he receives an honorarium for these.
References
- Haas AJ. The treatment of maxillary deficiency by opening the midpalatal suture. Angle Orthod. 1965;35:200-217.
- Hilgers J. The pendulum appliance for class II non-compliance therapy. J Clin Orthod. 1992;26(11):706-714.
- Hilgers J, Tracey S. The mini-distalizing appliance: the third dimension in maxillary expansion. J Clin Orthod. 2003;37(9):467-479.
- Grummons D. Nonextraction emphasis: space gaining efficiencies, parts 1 and 2. World J Orthod. 2003:3:21-32, 177-189.
- McNamara JA Jr, Lione R, Franchi L, et al. The role of rapid maxillary expansion in the promotion of oral and general health. Prog Orthod. 2015;16:33.
- Lione R, Ballanti F, Franchi T, Baccetti T, Cozza P. Treatment and posttreatment skeletal effects of rapid maxillary expansion studied with low-dose computed tomography in growing subjects. Am J Orthod Dentofacial Orthop. 2008;134(3):389-392.
- Chung CH, Font B. Skeletal and dental changes in the sagittal, vertical, and transverse dimensions after rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2004;126(5):569-575.
- Corbridge JK, Campbell PM, Taylor R, Ceen RF, Buschang PH. Transverse dentoalveolar changes after slow maxillary expansion. Am J Orthod Dentofacial Orthop. 2011;140(3):317-325.
- Marshall SD, Southard KA, Southard TE. Early transverse treatment. Semin Orthod. 2005;11:130-139.
- Hilgers J. Bioprogressive simplified. J Clin Orthod. 1988;12:48-69.
- Rocky Mountain Orthodontics RMDS. 2017. “RMO Data Services Syllabus.” https://www.rmortho.com/wp-content/themes/rmo/rmods/rmods_syllabus.pdf. Accessed September 13, 2019.
- Ricketts RM, Grummosns D. Frontal cephalometrics: practical applications, part I. World J Orthod. 2003;4:297-316.
- Grummons D, Ricketts RM. Frontal cephalometrics: practical applications part 2. World J Orthod 2004; 5:99-119.
- Akkaya S, Lorenzon S, Uçem TT. Comparison of dental arch and arch perimeter changes between bonded rapid and slow maxillary expansion procedures. Eur J Orthod. 1998;20(3):255-261.
- Grummons D. Quad helix innovations: pocket aces. Rocky Mountain Orthodontic Clinical Review. 2014;1-7.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
