CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to direct the orthodontist through a diagnostic sequence of recognizing and treatment planning for congenitally missing second premolars.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions with the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize some diagnoses of missing mandibular premolars.
- Realize some treatment options for mandibular premolars.
- Identify critical factors to consider to avoid complications.
- Identify three different methods of space closure from the case studies presented.

Dr. Mark W. McDonough discusses recognition and treatment planning for congenitally missing second premolars
Introduction
The orthodontist often identifies missing second premolars in the mixed dentition using routine panoramic radiographs. The early decisions that orthodontists make for the congenitally missing teeth often have an impact on dental health for the rest of their patient’s life. Therefore, this finding should result in a comprehensive set of diagnostic records in order to evaluate the patient in all three planes of space and establish a problem list and treatment alternatives. These records often need to be shared with the restorative dentist and other specialists in order to consider all viable alternatives and formulate a proper treatment plan. The clinician must make the proper decision at the appropriate time regarding the maintenance of the primary molar, the prosthetic replacement of the missing second premolar, or the closure of the space from the missing premolar.
The objectives of this review are to direct the orthodontist through a diagnostic sequence of recognizing and treatment planning for congenitally missing second premolars. The emphasis of this article is the most appropriate time and cost-effective way for closing the space for the missing premolar. Three different methods of space closure will be highlighted.
General concepts about missing mandibular premolars
Diagnosis of missing mandibular premolars
Congenitally missing mandibular second premolars are the second-most frequent type of agenesis, after the third molar, with an incidence of 2.5% to 5% of the population in the United States and Europe.1 Agenesis of the second premolars can usually be reliably diagnosed around age 9 on a panorex, but there have been reports in the literature of slow development of this tooth. Alexander-Abt2 reported a case of a 12-year-old female whose panoramic radiographs revealed apparent agenesis of tooth No. 20. The progress panorex 13 months later revealed initial crown formation of tooth No. 20. Unilateral agenesis has been reported to consist in up to 60% of the agenesis cases.3 Missing second premolars are more common in the mandible than the maxilla.
Treatment options
Upon the diagnosis of agenesis, two main options are usually considered: extraction of the primary second molar or its maintenance in the arch. If the primary second molar is extracted, the goal is usually to mesialize the first permanent molar in conjunction with the orthodontic treatment. If the other three premolars can be extracted as well due to crowding or procumbent incisors, the agenesis is a minor finding. The more complex problem is if the patient would not normally require extractions. Since the introduction of temporary anchorage devices (TADs), the unilateral space closure without other extractions has become more popular since the midline can be maintained while the space is closed. If the primary second molar is to be maintained, the goal is to maintain the tooth with the alveolar bone for possible future implant and prosthetic reconstruction.
Critical factors to consider
1. Dental and skeletal age of the patient
Treatment to close the space before or close to the peak of the pubertal growth spurt will be more successful. Since definitive diagnosis of agenesis of the second premolar cannot be made until the patient is 9 years old, the question arises, When is it too late to close the space? It has been shown that if the primary molar is extracted prior to age 11, and the second molar has not erupted, about 80% of the space will be closed through “driftodontics” within 4 years, leaving a residual space of about 2 mm.4
2. Gender
Female facial growth is generally complete around age 17 and males not until around age 21.5 It is important to note that these ages are averages, and it is always best to confirm cessation of vertical facial growth with annual serial cephalometric radiographs prior to placement of implants. This is a critical role the orthodontist can provide to the interdisciplinary team since orthodontists are best able to evaluate cephalometric radiographs. These age differences between male and female patients make prosthetic replacement more favorable in females since it can often be completed prior to leaving for college or entering the workforce. For male patients who are away at college, it is often difficult to coordinate implant placement and prosthetic treatment. Many times, finances are limited upon completion of college, and the patients are often no longer covered by their parents’ insurance, further limiting the ability to have costly prosthetic replacement.
3. Ankylosis of the primary second molar
Percussion of the primary second molar is often used to diagnose ankylosis, but it can be inaccurate. The most reliable method to diagnose primary molar ankylosis is to evaluate the interproximal bone levels on a bitewing radiograph. Flat bone levels between the primary molar and the adjacent permanent teeth indicate the primary molar is erupting evenly with the adjacent teeth. If there is an oblique angle, the primary tooth is ankylosed.6
4. The condition of the primary second molar
Root resorption of the primary second molar or large restorations and/or decay often lead to the decision to extract the primary second molar. Once this decision is made to extract the primary second molar, care should be taken during the extraction to maintain the cortical plates, especially in cases of ankylosis. Following extraction, it has been shown that the ridge narrows by 25% during the first 4 years after extraction and another 5% during the next 3 years for a total loss of 30% after 7 years. The authors also found that the ridge narrows more on the buccal side than the lingual side, resulting in a more lingual placement of the implant.7 Due to this loss of ridge width, space maintainers are not recommended after extraction of second primary molars due to decay or root resorption even if implants are planned. The adjacent teeth will drift into the space and when the teeth are uprighted for creating space for the eventual implant, the ridge will largely be maintained, and there will be a more favorable bone for the implant.6 This may result in longer orthodontic treatment time but a better final result for the implant.
5. Maintaining the primary second molar
Primary molars are shorter than permanent molar crowns, and therefore a marginal ridge discrepancy is to be expected and is not an automatic indication of ankylosis. If the primary molars have healthy roots with no carious lesions or large restorations and are not ankylosed, the decision may be made to maintain these teeth into adulthood — many case reports of primary posterior teeth surviving until the patient attains 40 to 60 years of age.8 However, there is a lack of long-term studies for the survival rate of retained primary molars from adolescence to adulthood. Maintaining the primary molar can create an anteroposterior arch-length discrepancy since the primary molars are 2 mm-3 mm larger than their permanent successor and results in an “end-on” molar relationship when the canines are Class I. This has led to some clinicians to slenderize the primary molar mesially and distally. The key is to remove sufficient tooth structure to create space but not enough to cause pulpal necrosis. A bitewing radiograph is useful to determine the width of the pulp horns. In general, 2 mm per side can be removed resulting in a 7 mm-8mm-wide tooth. It is recommended that light-cured composite be placed over the exposed dentin to help minimize the risk of caries to the narrowed primary molar.6 There are no long-term studies to show the longevity of narrowed primary molars, but it has been observed that there is more root resorption following reduction, and this method is recommended when implant replacement is planned.
6. Presence of third molars
Unfortunately, agenesis of second premolars is often associated with the absence of other teeth, especially third molars in the same quadrant, which may be found in 48% of patients.9 Usually, third molars have their initial calcification at age 9 and would be considered missing only after age 14. This also creates a treatment planning dilemma in the mandibular arch since the decision to close the space may be made prior to definitive knowledge of the presence of the third molar. If the space is closed in the mandibular arch, the maxillary second molar may not have a vertical stop if the mandibular third molar is congenitally missing or does not erupt.
7. The overall malocclusion
In general, patients with minimal crowding, deep overbites, retrusive incisors, decreased lower facial heights, or flat mandibular planes may be best managed by nonextraction. These patients should maintain the primary molars for as long as possible. Patients with significant crowding, dental protrusion, minimal overbites or open bites, and increased facial heights often benefit from extraction and space closure.
8. Cost considerations
Orthodontics to close an edentulous premolar space is more cost-effective and is often more periodontally sound. When the space is closed, the patient incurs only the cost of orthodontic treatment. When the space is maintained, the patient incurs the cost of orthodontic treatment, possible pre-prosthetic bone grafting, implant placement, and prosthetic restoration costs. Then there are the future costs of maintenance of implants, which is much greater than the cost of maintaining healthy natural teeth. For the above reasons, priority should be given to space closure treatment whenever possible.
Case Reports
The following three cases were chosen to highlight three different methods of space closure. They all presented with different malocclusions but shared the diagnosis of congenitally missing mandibular
second premolars.
Case 1
 A 9-year 8-month-old female presented for an initial consultation. The panorex (Figure 1) revealed that the developing first premolars had resorbed the mesial root of the primary second molars on both sides and ectopic eruption of the LL3 and LL4. She had a Class I molar relationship, deep bite, and mandibular crowding (Figure 2). Full orthodontic records were completed with a Phase I case presentation. Since the long-term prognosis was poor for the primary molars, she was referred for extraction of the primary molars as well as the LLD to aid in the eruption of the ectopic LL3 and LL4. The LLC was maintained initially to help prevent shifting of the midline. The LLC was eventually extracted once the premolars fully erupted. At the initial case presentation, it was decided to reevaluate once she entered into the adult dentition if the missing teeth would be prosthetically replaced or the spaces closed. The decision would be based on future skeletal growth as well as the amount of space closure that was achieved. Remember that if the spaces close from the extraction of the mandibular primary second molars, and the decision to open them for prosthetic replacement is eventually made, the ridge width will be much healthier. Therefore, for this patient the initial decision was easy.
A 9-year 8-month-old female presented for an initial consultation. The panorex (Figure 1) revealed that the developing first premolars had resorbed the mesial root of the primary second molars on both sides and ectopic eruption of the LL3 and LL4. She had a Class I molar relationship, deep bite, and mandibular crowding (Figure 2). Full orthodontic records were completed with a Phase I case presentation. Since the long-term prognosis was poor for the primary molars, she was referred for extraction of the primary molars as well as the LLD to aid in the eruption of the ectopic LL3 and LL4. The LLC was maintained initially to help prevent shifting of the midline. The LLC was eventually extracted once the premolars fully erupted. At the initial case presentation, it was decided to reevaluate once she entered into the adult dentition if the missing teeth would be prosthetically replaced or the spaces closed. The decision would be based on future skeletal growth as well as the amount of space closure that was achieved. Remember that if the spaces close from the extraction of the mandibular primary second molars, and the decision to open them for prosthetic replacement is eventually made, the ridge width will be much healthier. Therefore, for this patient the initial decision was easy.
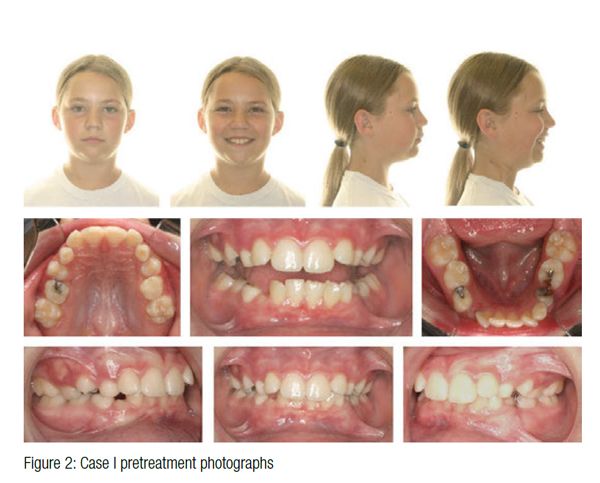
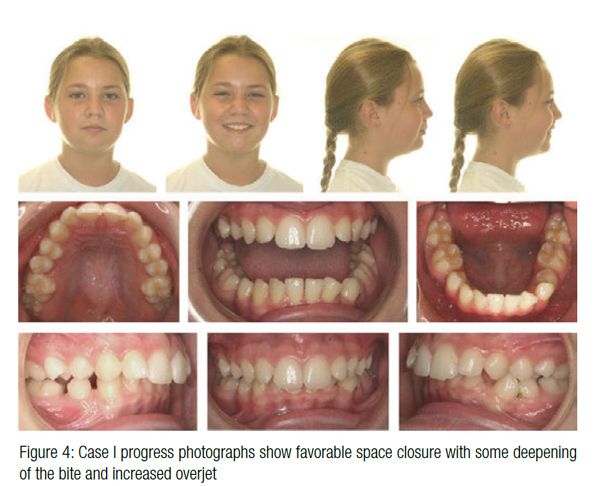
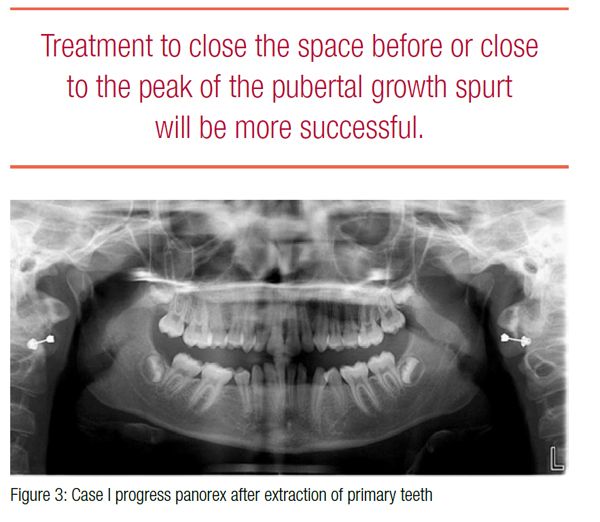 Her progress records at 11 years 1 month reveal favorable space closure (Figure 3), but only mild mesial drift of the first molars with some deepening of the bite with increased overjet (Figure 4). The Phase II consultation with the parents and patient included both space closure and space opening treatment plans. Ultimately, the decision was made to close the space due to the parents’ desire not to have prosthetic replacements with the additional cost and time required for the “final result.” The goal was to utilize Class II elastics, and if there was poor cooperation with elastics, a Forsus™ appliance would be utilized.
Her progress records at 11 years 1 month reveal favorable space closure (Figure 3), but only mild mesial drift of the first molars with some deepening of the bite with increased overjet (Figure 4). The Phase II consultation with the parents and patient included both space closure and space opening treatment plans. Ultimately, the decision was made to close the space due to the parents’ desire not to have prosthetic replacements with the additional cost and time required for the “final result.” The goal was to utilize Class II elastics, and if there was poor cooperation with elastics, a Forsus™ appliance would be utilized.
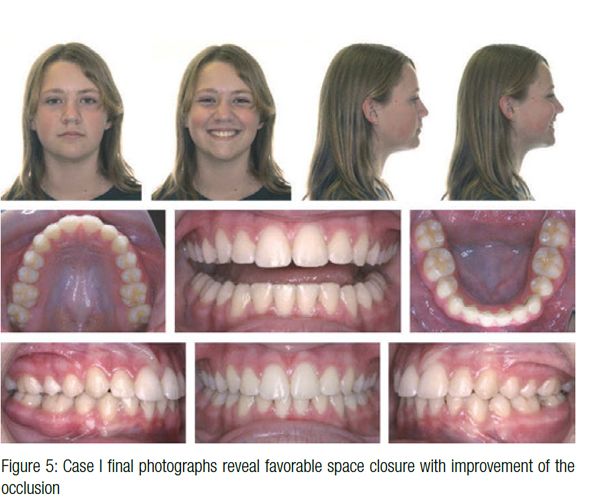
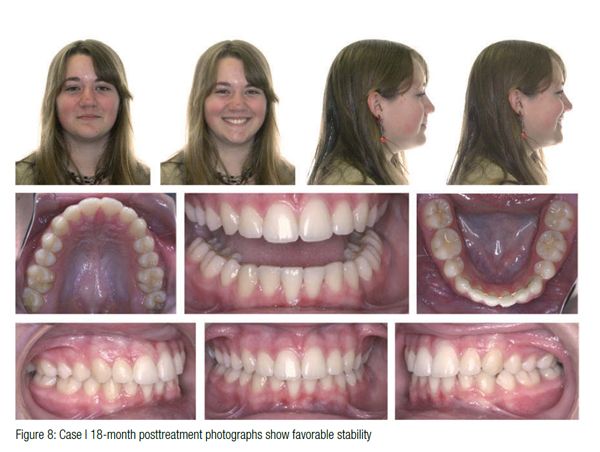
 The final result after 23 months of active treatment reveals a solid Class III molar with Class I canines and favorable facial esthetics (Figure 5). The patient wore Class II elastics for 5 months, and the panorex (Figure 6) revealed that the mandibular third molars have a mesial angulation but a good chance to erupt. These patients understand that it is critical to wear their maxillary Essix retainers until the mandibular third molars erupt to prevent supraeruption of the maxillary second molars. The cephalometric superimpositions (Figure 7) from initial presentation at age 9 to deband at age 13 shows maintenance of the mandibular incisor angulation and favorable mandibular growth, which was beneficial to improving the facial esthetics. The 18-month posttreatment photographs (Figure 8) show excellent stability.
The final result after 23 months of active treatment reveals a solid Class III molar with Class I canines and favorable facial esthetics (Figure 5). The patient wore Class II elastics for 5 months, and the panorex (Figure 6) revealed that the mandibular third molars have a mesial angulation but a good chance to erupt. These patients understand that it is critical to wear their maxillary Essix retainers until the mandibular third molars erupt to prevent supraeruption of the maxillary second molars. The cephalometric superimpositions (Figure 7) from initial presentation at age 9 to deband at age 13 shows maintenance of the mandibular incisor angulation and favorable mandibular growth, which was beneficial to improving the facial esthetics. The 18-month posttreatment photographs (Figure 8) show excellent stability.
This patient demonstrates that space closure can be achieved with early extraction of the primary second molars (age 9 years 8 months), drifting of the adjacent permanent teeth into the edentulous area, and excellent cooperation with Class II elastics for 5 months.
Case 2
A 13-year 1-month-old male presented for the first time, and his panorex (Figure 9) revealed congenitally missing mandibular second premolars and maxillary third molars. This is the most favorable combination of missing teeth for space closure. The retained primary molars had significant root resorption and were unlikely to be retained for very long. He had a Class I malocclusion with procumbent maxillary and mandibular incisors with minimal overjet and overbite (Figure 10). Due to the obtuse nasolabial angle, it was decided that the goal would be to maintain the upper incisor position (no extractions in the maxillary arch). The case presentation reviewed the options of prosthetic replacement of the missing teeth with narrowing of the primary molars so the mandibular crowding could be relieved and eventual prosthetic replacement would take place around age 19-21 when facial growth had been completed. It was anticipated the primary molars would be lost during orthodontic treatment. This would require fixed retention with a bonded heavy wire to maintain the space until growth is complete. The alternative plan was to extract the primary molars and protract the permanent molars into a Class III relationship. Given the high anchorage values of the mandibular molars and the relatively low anchorage of the incisors, there would be unfavorable lingual tipping and/or retraction of the incisors if conventional space closure was used. Therefore, temporary anchorage devices (TADs) were proposed to aid in anchorage for mesial movement of the mandibular first and second molars. The family decided to close the space primarily due to the shorter total treatment time and overall less financial costs even with the additional cost for TADs. They understood that space closure in this type of patient often adds 6-8 months to the orthodontic treatment.
 Six months into treatment, the TADs were placed between the L 3s and 4s (Figure 11) utilizing direct anchorage and sliding jigs to protract the first molars. These sliding jigs allow for a horizontal force to be applied to the molars through the approximate center of resistance which should result in faster space closure. However, the mechanical advantage seems to be negligible. A simpler set up of placing the TADs between the L 2s and 3s and utilizing indirect anchorage (Figure 12) seems to have less force on the TADs, which increases the percentage of TADs that survive to the end of treatment — this is my current preferred method of space closure. Historically, TADs have an 80% survival rate with the indirect anchorage set up having a slightly higher percentage of success. It is important not to band the second molars until after all space closure is achieved since they will generally follow the first molars, and banding them would increase the anchorage and friction on the space closure system. Even with the TADs, some minor increase in overjet was observed, and 5 months of sleep-time Class II elastics was necessary to achieve a full-cusp Class III molar with proper overjet.
Six months into treatment, the TADs were placed between the L 3s and 4s (Figure 11) utilizing direct anchorage and sliding jigs to protract the first molars. These sliding jigs allow for a horizontal force to be applied to the molars through the approximate center of resistance which should result in faster space closure. However, the mechanical advantage seems to be negligible. A simpler set up of placing the TADs between the L 2s and 3s and utilizing indirect anchorage (Figure 12) seems to have less force on the TADs, which increases the percentage of TADs that survive to the end of treatment — this is my current preferred method of space closure. Historically, TADs have an 80% survival rate with the indirect anchorage set up having a slightly higher percentage of success. It is important not to band the second molars until after all space closure is achieved since they will generally follow the first molars, and banding them would increase the anchorage and friction on the space closure system. Even with the TADs, some minor increase in overjet was observed, and 5 months of sleep-time Class II elastics was necessary to achieve a full-cusp Class III molar with proper overjet.
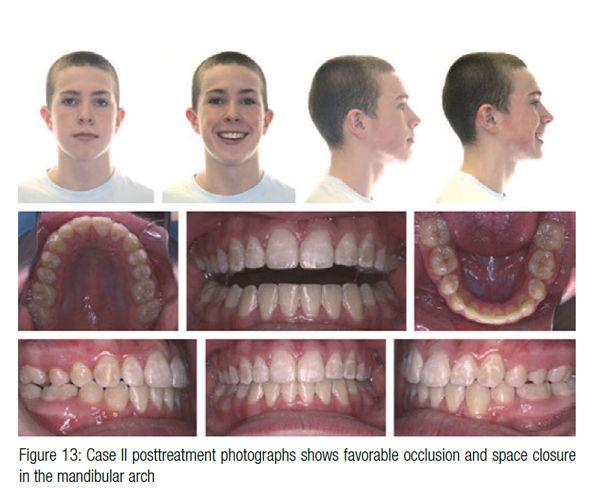 After 24 months of treatment, the appliances were removed (Figure 13) with a solid Class III molar and Class I canine. The posttreatment panorex (Figure 14) revealed favorable development of the mandibular third molars with anticipation that they would erupt into occlusion. The cephalometric superimpositions (Figure 15) reveal no significant change in the mandibular incisal angulation with significant mesial movement of the mandibular molars.
After 24 months of treatment, the appliances were removed (Figure 13) with a solid Class III molar and Class I canine. The posttreatment panorex (Figure 14) revealed favorable development of the mandibular third molars with anticipation that they would erupt into occlusion. The cephalometric superimpositions (Figure 15) reveal no significant change in the mandibular incisal angulation with significant mesial movement of the mandibular molars.
Case 3
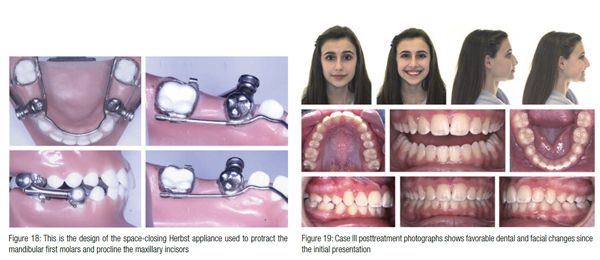
This patient presented at age 11 years 4 months of age with a full cusp Class II Division 2 malocclusion, incisal crowding, maxillary constriction, and congenitally missing mandibular second premolars (Figure 16 and 17). At the initial case presentation, it was decided to address the maxillary skeletal transverse deficiency first with a palatal expander and reevaluate the decision for the mandibular primary molars. The family was unable to commit to a preference of prosthetic replacement or space closure, and it was decided to consult with their restorative dentist and take progress records after expansion was completed. Seven months after the initial records, the family had discussed the treatment options with their restorative dentist, and the progress records revealed no significant skeletal change. The family decided that space closure for the missing premolars was their first choice. This option did not lend itself to utilizing TADs like the previous patient since there was a skeletal discrepancy and a deep bite. A space-closing Herbst appliance (Figure 18) was utilized to protract the mandibular first molar, procline the maxillary incisors, and help open the bite. A space-closing Herbst utilizes stainless steel crowns on the U 6s and L 4s with bands on the L 6s. A lingual sheath on the L 6s slides along the lingual holding arch. Nitinol closed-coil springs are used on the buccal with elastic thread on the lingual to protract the molar in a bodily fashion. After 12 months of Herbst treatment, the spaces were closed, and the patient had full bands and brackets for 13 months to complete her treatment. She finished with locked-in Class III molars, favorable facial changes, and a solid Class III molar with Class I canines (Figure 19). The panorex revealed favorable space closure with the third molars in a position to erupt (Figure 20). The cephalometric superimpositions revealed vertical changes with significant mesial movement of the mandibular first molar (Figure 21).
This patient had an extended treatment time due to the combination of skeletal discrepancies and a significant malocclusion with a lack of commitment to the decision to maintain or close the space at the initial treatment consultation. It demonstrated that patients and parents often need time to digest the problem list, and it is important to move forward with the initial step, which also allowed me to establish the patient’s level of cooperation. Clearly, this was the more complicated orthodontic plan as opposed to maintaining the primary molars, but it yielded the most benefit for the patient since no further treatment is necessary.
Conclusions
Congenitally missing mandibular second premolars are a common problem. The critical factors to consider in the decision to maintain the primary molar or close the space from the congenitally missing second premolar were reviewed. Maintenance of the primary molar is often appropriate if the tooth is not ankylosed, has good roots, and no decay or restorations. These teeth can often be maintained well into adulthood. Three different methods of space closure were presented, and each patient achieved a healthy, functional, and esthetic outcome. The key to each plan was that the lower incisor position was not compromised, and a solid Class III molar was achieved with a high probability that the mandibular third molar would erupt into occlusion. This type of treatment often takes longer than space maintenance, but the priority should be given to space closure treatment to maximize the overall periodontal health as well as the reduced overall long-term cost of treatment. The decisions the orthodontist makes for these patients will have a lifetime impact on the patients’ dental health.
References
- Fines CD, Rebellato J, Saiar M. Congenitally missing second premolar: treatment outcome with orthodontic space closure. AM J Orthod Dentofacial Orthop. 2003;123(6) 676-682.
- Alexander-Abt J. Apparent hypodontia: A case of misdiagnosis. Am J Orthod Dentofacial Orthop. 1999;116:321-323.Vastardis H.
- The genetics of human tooth agenesis: new discoveries for understanding dental anomalies. Am J Orthod Dentofacial Orthop. 2000;117(6):650-656.
- Mamopoulou A, Hagg U, Shrӧder U, Hansen K. Agenesis of mandibular second premolars. Spontaneous space closure after extraction therapy: a 4-year follow-up. Eur J Orthod. 1996; 18(6):589-600.
- Fudalej P, Kokich VG, Leroux B. Determining the cessation of vertical growth of the craniofacial structures to facilitate placement of single-tooth implants. Am J Orthod Dentofacial Orthop. 2007;131(suppl 4):59-67.
- Kokich VG, Kokich VO. Congenitally missing mandibular second premolars: clinical options. Am J Orthod Dentofacial Orthop. 2006;130(4):437-444.
- Ostler M, Kokich VG. Alveolar ridge changes in patients congenitally missing mandibular second premolars. J Prosthet Dent. 1994;71(2):144-149.
- Zimmer B, Schelper I, Seifi-Shirvandeh N. Localized orthodontic space closure for unilateral aplasia of lower second premolars. Eur J Orthod. 2007;29(2):210-216.
- Vastardis H. The genetics of human tooth agenesis: new discoveries for understanding dental anomalies. Am J Orthod Dentofacial Orthop. 2000;117(6):650-656.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
