CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to establish a thorough understanding of the recent advancements in data
capture for sequential aligner therapy and its impact upon tooth movement predictability.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize the burgeoning demand for sequential aligner therapy, particularly esthetically biased adult orthodontics.
- Recognize recent advancements in data capture concepts and techniques.Identify ways of optimizing fit, movement, and speed with aligner deslippage devices.

Dr. David Penn examines the accuracy and precision of the traditional versus digital impression techniques
Abstract
As the demand and sophistication for sequential aligner therapy continues to grow, orthodontists are treating patients, (especially esthetically biased cases) with an expectation of the shortest possible treatment period.
This paper examines the accuracy and precision of the traditional versus digital impression techniques for full-arch capture and presents an improved technique using the conventional methodology.
The conclusion, which needs further investigation, is that more accurate initial data will produce more intimate fitting aligners, greater accuracy of force propagation, and hence more predictable outcomes.
Clear aligner therapy
Clear aligner therapy is an orthodontic treatment in which the patient wears a series of clear, removable aligners that gradually move the teeth to improve the occlusion, function, and/or esthetic appearance. Much of its success depends upon the understanding, cooperation, and compliance of the patient.
The idea of an invisible appliance was first introduced by Kesling in 1945.1 As an alternative to the bracket system, the invisible method of orthodontic tooth movement was introduced commercially in 1999 by Align Technology with the trade name of Invisalign®. This invisible appliance uses the principles of Kesling setup through virtual digital models and computer-aided design and manufacturing process (CAD-CAM). Since Invisalign was first introduced, Align Technology has widened its range of products to now include treatment of minor tooth movements, esthetically biased cases, and comprehensive orthodontics involving 3D tooth movement.
Subsequently, a plethora of competing clear aligner manufacturers have come to the market invoking different manufacturing processes, aligner materials, clinical protocols, and treatment plans.
The introduction of clear aligner therapy was treated with significant skepticism by orthodontists in its early days. The predictability of individual tooth movement varied significantly, and the degree of complexity of suitable cases was somewhat limited.
Within the last decade in particular, considerable investment in the research and development has taken place in almost every aspect of clear aligner therapy. Demand continues to grow significantly, with Align Technology alone claiming to have treated more than 3.4 million cases since its inception and more than a 23% increase in cases for the same quarter (119.6K cases versus 147.5K cases in Q3 of 2015).2
While logic would suggest that the more precise the capturing of the original tooth morphology, then the more intimate will be the fit of the aligners and the force application more accurate, is this necessarily true? Given that there are both variations and limitations to the manufacturing process (vacuum formed and pressure formed), the materials employed, and the fact that the aligners are not permanently affixed to the tooth surface, we need to ensure that the data that we record initially gives us every possible advantage in order to apply forces as efficaciously as practicable. Given that the environment is wet, the teeth are generally smooth, and the aligners are shaped so that removal is possible and, indeed, relatively easy, we have many factors to overcome.
As a new aligner is placed in situ, a force or multiple force systems are applied to one or more teeth. Given that the three fundamentals required for tooth movement are in place — force, space, and time — then the movement should occur. Assuming that the patient is compliant and the “time” element is assured, the key issue then becomes the accurate application of these “force” systems.
Effective data capture concepts
Two methods of capturing initial data for sequential aligner therapy remain popular: the use of conventional impression materials and, more recently, the use of intraoral scanners. Both options are highly material/device- and technique-employed sensitive, and a broad range of clinical outcomes are produced that impact on aligner fit.
However, the concept of digital impressioning being more accurate, faster, and more cost-effective than conventional PVSE/ PVS impressions remains controversial, especially in full-arch capture for sequential aligner therapy.
Since first being introduced in the 1990s, the expectation that every practice would be exclusively digital within 5-10 years has not eventuated.3 With the increase in the use of CAD/CAM, not only in restorative dentistry but also in surgery, orthodontics, diagnostics, and treatment planning, digital impressioning must meet a high level of accuracy if it is to be accepted as a viable alternative.
Ender and colleagues compared the precision of conventional and digital methods for complete arch impressions.4 The purpose of this study was to assess the accuracy of both techniques in vivo.
In order to supersede the capabilities of conventional impressions, digital impressions must perform at least at the same level of quality and accuracy as current conventional techniques. On the basis of the results of the in vivo study listed earlier, the null hypo-thesis that conventional and digital impression systems are equally accurate must be rejected.
This study revealed significant differences in precision according to the method used to obtain the complete-arch impression.4 Large differences were visible in the conventional impression materials and in the digital impression techniques. Conventional impressions using vinylsiloxanether material showed the highest precision, while those using the irreversible hydrocolloid showed the lowest precision (as shown in Table 1).4
The digital intraoral impression systems resided in between these extremes; the digital systems were significantly less precise than the highly precise conventional impression materials.4
The precision achieved across the complete arch scans did not differ significantly among the various digital impression systems. All of the digital systems showed a larger standard deviation compared with the high-precision conventional impression materials.
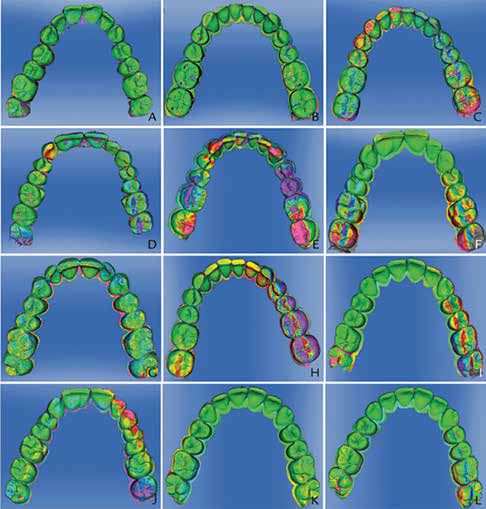
The anterior region has little geometric information and was particularly difficult to scan with the digital intraoral cameras (Figure 1).4 Significantly, in relation to clear aligner therapy and where forces need to be applied most accurately, error propagation in this region leads to increased deformation toward the distal end of the dental arch.
Figure 1 shows the typical deviation pattern between repeated complete-arch scans within the test groups. The conventional impressions in the VSE and VSES groups showed minimal deviation (≤40 µm) across the incisal edges of the anterior teeth and at the buccal surface of the premolars, which has critical clinical manifestations given that is where attachments are placed and that much of the specific force application and tooth movement is expected to occur.4
In general, the digital impression systems with high frame rates (video-based systems and the OC, LAV, T-Def, TRI, and TRC groups) began to deform distal to the anterior region of the dental arch. Single images based on the digital impression system (CER, ITE) primarily showed local deviation with increasing deformation toward the distal end of the cast. In contrast, while the conventional impressions showed local deviation, the deviation did not increase in magnitude toward the distal arch.4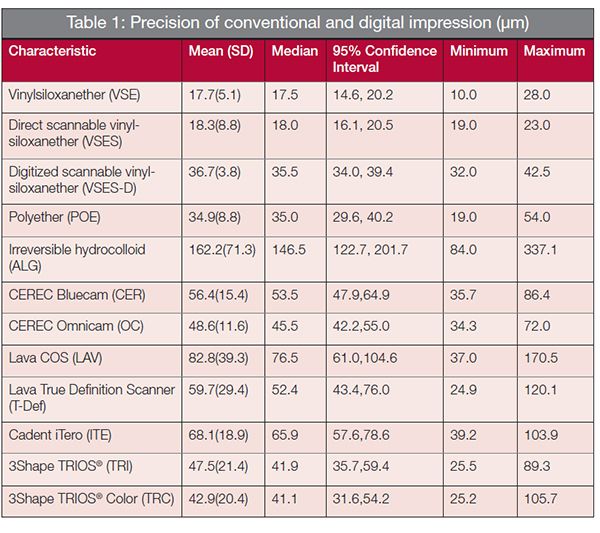
What are the clinical implications of a 25 to 40 micron difference in accuracy between a precision conventional impression and a quality digital scan?
Given that sequential aligners generally program movements of between 125 to 250 microns per aligner over each 2-week period, this differential may have significant clinical impact. Further research needs to be conducted in this area. Additionally, concerns over larger distortion in particular segments of the arch need to be investigated closely.
While the use of PVSE and PVS impressions are still fraught with the drawbacks of drags, tears, voids, tray-to-tooth contact, temperature sensitivity, limited working time, and material shrinkage, this technique should not be readily discarded lightly from orthodontic practice.5
The principal advantage of digital impressions would be that they are less stressful and uncomfortable for many patients, and additionally, there is no need to select a tray, apply tray adhesive, clean impression trays, assemble impression guns and tips, or dis-infect impressions. Digital impressions with a deficient area can also be rescanned rather than retaking the entire impression.
For the orthodontist, the obvious advantages of digital scanning include accelerated diagnosis and treatment planning, rapid submission to aligner manufacturers, minimal retakes, and a reduced impression material inventory expenditure and storage. Open and trusted connections with orthodontic laboratories, merging of CBCT and DICOM files, increasing file transfer among manufacturers, and in-practice 3D printing will open a myriad of possibilities for this technology, but only when a consistent degree of uniform accuracy can be demonstrated.
However, given that their remains doubt that digital impressioning may be more accurate, faster, and more economical, do the supposed benefits justify the large initial capital investment that needs to be made? Although most manufacturers claim that the scanning procedure requires roughly the same amount of time as traditional impression materials’ setting time, the experience of the scanner operator, technique employed, and the scanning technology employed by each machine impinge significantly on the efficiency and accuracy of the process.6
Considerable investment in the research and development has taken place in almost every aspect of clear aligner therapy
Not all orthodontic staff are trained with all scanners, and the learning curve to master the use of new technology can be lengthy and expensive. Alternatively, proficiency with traditional impression techniques is common to all orthodontic staff, and the process is generally highly predictable.
Many orthodontists still struggle to decide whether intraoral scanning technology is actually worth the investment. Although digital scanners currently range from around $10,000 to the mid-$30,000 range, this cost may be recovered in reduced overheads and increased practice efficiency if the machine is used regularly and staff turnover is minimal (especially if the practice is prescribing a large volume of clear aligner cases).
Optimizing traditional impression techniques
The process of taking impressions is simply to transfer 3D physical data from the patient’s mouth as accurately and comfortably as possible. In theory, the greater the transfer accuracy, the more intimate the aligners will fit, thus increasing the chance of tooth movement being expressed completely and heightening the predictability of the treatment plan.
Traditional impression materials are used with a wide range of clinical techniques for accurate capture of the critical elements for successful clear aligner therapy. Hence they all require excellent material property predictability and can cope with a broad spectrum of clinical applications. Most practitioners do not have the time to address the science and technology that goes into the development of a clinically successful impression material and the behind-the-scenes work that facilitates and optimizes chairside procedures.
The ideal impression material reflects all the hard- and soft-tissue details, including their static relationship in the mouth. This data is transferred during the relatively short working time (30 to 90 seconds) and fixed (polymerized) into the impression material memory during the setting time (60 to 240 seconds). The shape of the impression is unalterable after this: impressions should work perfectly the first time, every time. Given the degree of discomfort and the time-consuming and expensive nature of capturing dual full arches for clear aligner treatments, the importance of utilizing the most efficacious materials and technique is paramount.7
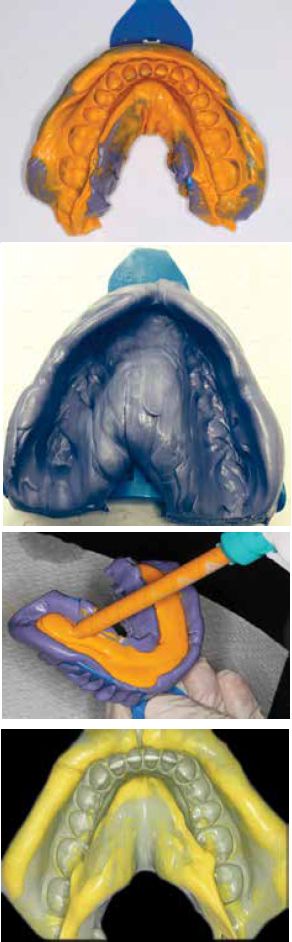
The 2013 study by Dugal and colleagues demonstrated that the two-step light body/putty technique with a 1.0 mm spacer (for light body capture of critical data) delivered the most accurate results with polyvinyl siloxane impression materials.8 This technique has been designed and taught by the School of Aesthetic Orthodontics, Postgraduate School of Dentistry (Sydney, Australia) (Figure 2).
This technique relies on the following material properties and clinical protocols:
- The putty material should be softer and exhibit flow characteristics that allow for capture of the sulcular regions 4 mm-5 mm beyond the margins of the teeth (low viscosity).
- The correctly selected impression tray (adequate width and length, no contact with tooth structure, and with sufficient retentive elements to ensure delamination or debonding will not occur) should be firmly seated, with adequate putty in situ, especially in the posterior segments, briefly muscle trimmed, and removed after 45 seconds. Flow into sulcular areas is mandatory.
- The occlusal anatomy captured should be partially obliterated using a mirror handle or light finger pressure, with great care taken not to distort the periphery. The aim is to create an even distribution for 1.0 mm of light body material and for it all to be supported by the correctly extended putty (Figure 3).
- Additional putty can be added in areas of under-extension, and over-extended areas can be trimmed with a scalpel or scissors.
- The putty is left to cure completely, and then the copious addition of light body occurs, ensuring that the mixing tip is completely embedded in the light body at all times to ensure no introduction of air bubbles (Figure 4).
- The loaded tray is seated completely, anchored with one hand, and muscle trimming is performed, driving the light body toward the gingival margins to minimize voids.
- Upon setting, the tray is removed rapidly. Slow, teasing removal increases the likelihood of tearing, especially in black triangular embrasures in the lower anterior segments.
- The impression is inspected carefully, particularly on the axial walls where attachments may be placed. A minimum of 2 mm gingiva should be captured and as much data recorded in light body as possible.
- The one-stage technique is not suitable for full-arch orthodontic recordings as the hydraulic forces created by the simultaneous loading of putty and light body drives the light body away from the critical areas to be captured. Typically, when this technique is employed, the operator will see the sulcular areas captured in light body and too much critical data recorded in the less accurate putty base. (Figure 5)
Enhancing the delivery of forces from the aligners
If the most accurate data can be recorded, and the aligner manufacturer can supply devices with optimal physical characteristics to deliver these forces, it would be essential then that the aligners are correctly anchored and placed, especially immediately after removal and replacement.
Devices to aid in the seating of aligners have been employed since aligner therapy commenced. The aim is to promote a more intimate fit of the aligner against the tooth.
Aligner “Chewies™” from Dentsply Raintree Essix are a rubber material that were introduced to help close any spaces between the teeth and aligners. As expected, the insertion of a new aligner should have a small allowance for programmed tooth movement, and the concept of the device was to minimize the space by forcing the aligner to interact with the tooth surface more effectively.
The primary drawback from this design is that it acts upon only one point of the incisal edge of the anterior teeth, which can aid in seating, but also causes distortion of this area of the aligner with repeated use.9
Munchies® are an anatomically enhanced orthodontic enhancement device designed to accelerate aligner therapy by maximizing the accuracy of fit of each aligner. Using a series of differing Shore Hardness medical-grade silicones and capturing up to 30% of the clinical crown, these visco-elastic devices deform momentarily to grab the aligner and aid in complete seating.10
The patient engages his/her upper or lower anterior teeth into anatomically designed grooves on each Munchies device and applies apical pressure from the opposing arch (Figures 6 and 7). The device deforms as pressure is increased to encase the aligner and drive it into the most intimate fit.
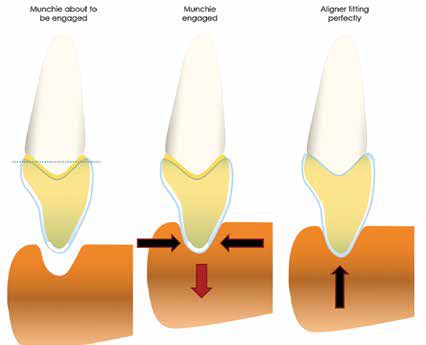
In a pilot study by Sharp A and Dove E in 2015, 100% of patients reported significantly improved seating of their aligners when Munchies were used immediately after reinsertion.11 In addition, 70% of patients also reported pain relief during all stages of orthodontic treatment by inducing the “bite wafer” effect.12

Conclusion
The demand for sequential aligner therapy continues to grow. In order to achieve optimal outcomes and shortest treatment times, the accurate recording of initial data is paramount. This paper examined the variable nature of the results from traditional and digital impression techniques. Traditional impression techniques, employing superior materials and approved protocols produce the most accurate initial data.
Author Info
 Dr. David Penn is Head of the School of Aesthetic Orthodontics, Postgraduate School of Dentistry in Sydney, Australia.
Dr. David Penn is Head of the School of Aesthetic Orthodontics, Postgraduate School of Dentistry in Sydney, Australia.
References
- Phulari BS. History of Invisalign. In: History of Orthodontics. New Delhi, India: JayPee Brothers Medical Publishers; 2013: 226-237.
- Aligner Technology, Inc. website. Invisalign Corporate Fact Sheet. website. aligntech.com/documents/Align Technology Corp Fact Sheet 2015 Q1_F.pdf. Accessed December 14, 2015.
- Kim SY, Lee SH, Cho SK, Jeong CM, Jeon YC, Yun MJ, Huh JB. Comparison of the accuracy of digitally fabricated polyurethane model and conventional gypsum model. J Adv Prosthodont. 2014;6(1):1-7.
- Ender A, Attin T, Mehl A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J Prosthet Dent. 2015;Nov 6.
- Ender A, Mehl A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015;46(1):9-17.
- Ender A, Mehl A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int J Comput Dent. 2013;16(1):11-21.
- German MJ, Carrick TE, McCabe JF. Surface detail reproduction of elastomeric impression materials related to rheological properties. Dent Mater. 2008; 24(7):951-956.
- Dugal R, Railkar B, Musani S. Comparative evaluation of dimensional accuracy of different polyvinyl siloxane putty-wash impression techniques-in vitro study. J Int Oral Health. 2013;5(5):85-94.
- DENTSPLY Raintree Essix website. Chewies™ Aligner Tray Seater. https://www.essix.com/orstore/downloads/DFU/Chewies_DFU.pdf. Accessed December 10, 2015.
- Ortho Munchies website. All about Munchies®. https://www.orthomunchies.com/all-about-munchies/overview. Accessed December 10, 2015.
- Sharp A, Dove E. Pilot study on aligner acceleration and seating device. Paper presented to: NSW Government Dept. of Innovation 2015.
- Farzanegan F, Zebarjad SM, Alizadeh S, Ahrari F. Pain reduction after initial archwire placement in orthodontic patients: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2012;141(2):169-173.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
