Dr. Patrik Zachrisson describes a tooth-colored milled bonded retainer in PEEK
Abstract
Following all types of active orthodontic treatment, a period of retention is advised in order to prevent relapse and the natural movement of teeth as they wear and shift as we get older. As there are many types of retainers, the one recommended by the orthodontist will be chosen to fit a specific treatment situation. The period of retention varies from usually 12 months to life retention. Retainers are usually removable Essix- or Hawley-type retainers or fixed-wire retention. A new type of retainer, digitally manufactured in PEEK material, can now be bonded onto teeth using conventional composite resin cement techniques to create a strong, durable, tooth-colored flexible, biocompatible, and more anatomically adapted retainer.
Introduction
The use of clear retainers or wire retainers following orthodontic treatment is widely accepted. A change in the alignment of lower incisors during the second, third, and fourth decades of life has been widely reported in studies of both who have undergone previous orthodontic treatment followed by retention as well as in untreated patients (Little, et al., 1988, Little 1990).
A number of choices are now available to the orthodontist following a course of active treatment. On the National Health Service (NHS in England), the orthodontist is responsible for the retention for 12 months, but in many cases, longer retention is needed, and in some cases, patients continue with retainers for life (Clark, et al., 1997).
The removable retainers are usually used at nighttime. A common type of retainer is the clear thermoformed Essix retainer, which is made to fit on a plaster cast of the teeth. The Essix is a polpropylene or polyvinylchloride (PVC) plastic material, usually in .20 or .30 thickness. It will cover the whole arch and normally extend onto the gum line. There is some evidence that the use of a clear retainer is preferred by patients (Hichens, et al., 2007).
We can also make Vivera-type retainers from Invisalign®, based on the position of a specific aligner or from a new impression or digital scan. They also provide full-arch coverage but are trimmed like the active aligners so are comfortable to wear.
A durable alternative is the Nimrod-Retainer milled from a flexible but hard-wearing material, which is thinner than a typical vacuum-formed retainer. Sometimes a Hawley- or Begg-type retainer is prescribed, using a clear or metal wire on the anterior surface of the teeth. The advantage with this type is that it allows a degree of adjustments and occlusal contact between the upper and lower teeth (Sauget, et al., 1997).
A fixed retainer is bonded onto the lingual or palatal surface of the teeth and provides around-the-clock support for the teeth. The retainers may consist of a single or multistranded wire, usually a 0.0215 inch multistranded wire or 0.030-0.032-inch sandblasted round stainless steel wire or a reinforced fiber. Most wire retainers are of the multistranded type and bonded to every tooth using acid-etch composite bonding techniques. Occasionally, a wire-bonded canine-to-canine may be used. The fiber retainer has a following but is considered more prone to fracturing (Heier 1997, Zachrisson 1995).
It is essential that fixed wire retainers are fitted completely passively, or else ortho-dontic movement is likely to occur. The fixed wires cannot be removed by the patient so compliance in good oral hygiene is essential to prevent buildup of scale on the lingual or palatal areas where the wire is fitted.
When fitting an upper bonded retainer, special care should be taken to make sure that the lower teeth do not bite on the retainer as it can cause it to debond. There are risks of wire debonding, especially in the upper anterior area due to the bite (Lumsden, et al., 1999; Artun and Urbye 1988).
Reasons for orthodontic relapse
A multitude of factors may affect the long-term stability of the completed orthodontic treatment. As the structures supporting the teeth stabilize, the risk of relapse reduces but will remain to a degree and will always be present. Teeth tend to want to relapse into the original passive position, but other factors may play a role. Delayed growth, known as latent jaw growth, may occur in the lower jaw up to the age of 21 in women and up to age of 25 in men.
Temporomandibular dysfunction, grinding, and clenching may affect the strain on the teeth, contacts in occlusion, and the repeated tension in the arches may cause misalignment. The ADA estimates up to 95% of Americans have a grinding or clenching habit. It is widely accepted that aging affects the dentition as enamel wears, teeth weaken, and we may get further restorations. This can lead to a change in the occlusion and the balance between teeth. It is not unusual to see lower anterior overcrowding as we age. If a tooth is lost, and the space is not restored, mesial drift may cause teeth to migrate anteriorly or tip into a gap. There are also genetic factors to account for (Johnston and Littlewood 2015; Hegde, et al., 2011).
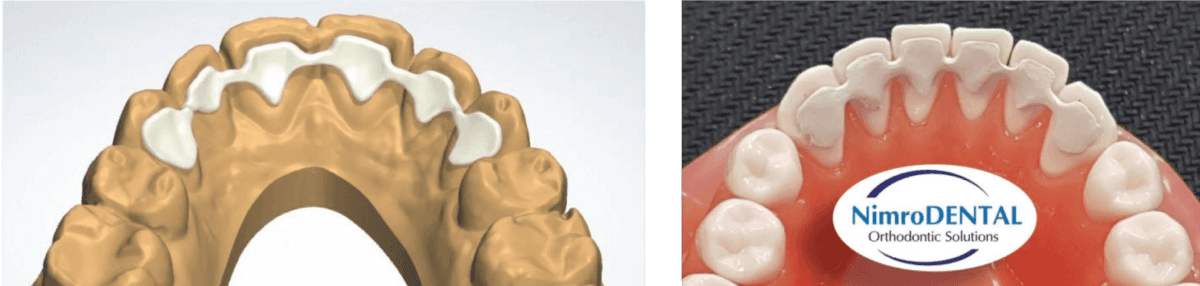
Figure 1: Design of a PEEK wire retainer on a digital model at lab and Figure 2: PEEK wire on a lab model
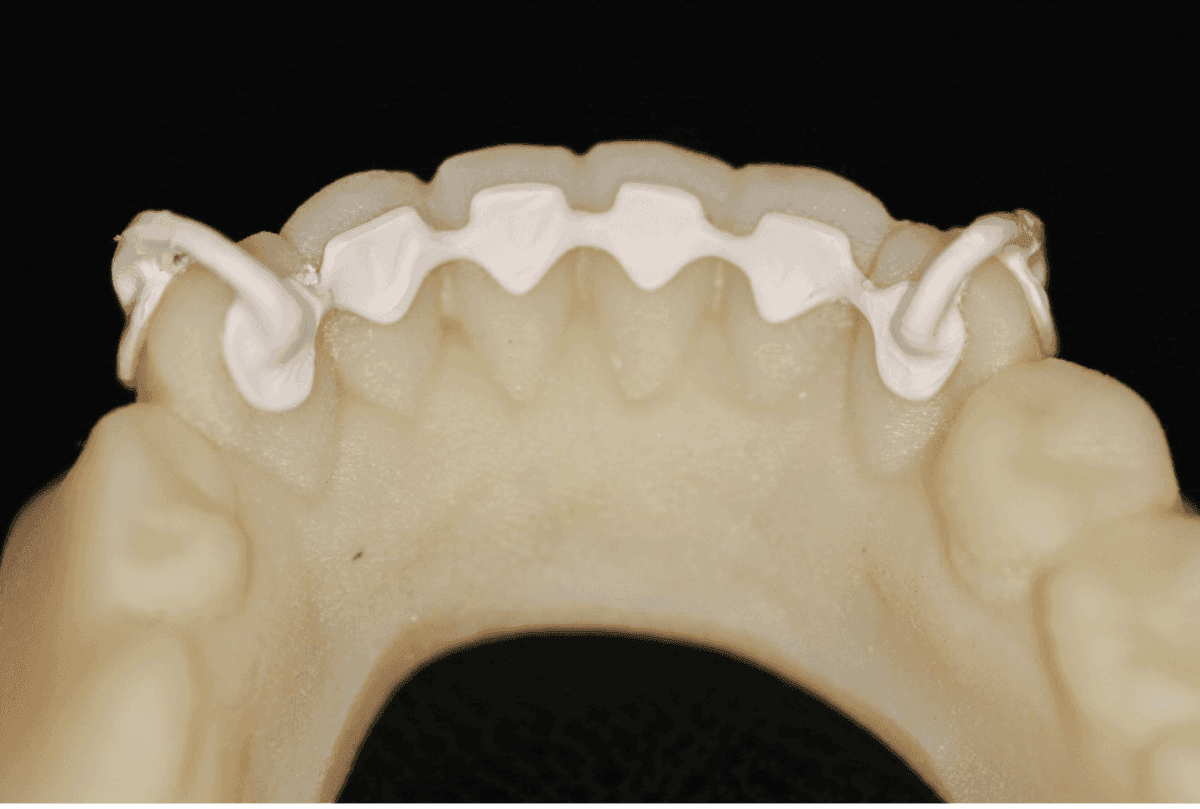
Figure 3: A 3D-printed model is made showing the fit of the wire and planned alignment using the integrated PEEK spurs that rest on the anterior aspect of the canines

Figure 4: Occlusal aspect of wire showing extension of supports labially with wire seated on 3D-printed model and Figure 5: The passive position of the PEEK wire retainer is verified in the mouth using the milled supports
PEEK material and physical properties
The organic thermopressed polymer known as PEEK, polyetheretherketone, is a colorless material now widely used in engineering and technology. PEEK has excellent chemical and mechanical resistance properties, even at higher temperature. It has a melting point around 340 degrees centigrade, so can safely be sterilized using autoclaves. It shows a high resistance to biodegradation and damage in organic and aqueous environments. It has a high tensile strength at 90 to 100 MPa with an elastic modulus of 3.6 MPa (Parker, et al., 2012).
PEEK is now commonly used in a number of medical applications such as in medical implants, MRI imaging and neurosurgery, and many more, and in industrial applications like pumps, piston parts, and valves. It is now used in aerospace technology and chemical industries where, because of its unique properties, it can work well under load and high temperatures.
In 2016, a PEEK filament was made available for the production of 3D-printed parts, using fused deposition modeling (FDM) technology (Surgical Technologies 2016, Design News 2016). Three-dimensional printing has opened up an entire new field of applications for PEEK including orthodontic appliances, partial denture frameworks, clasps, and many more. To make it even more exciting, it is possible to mill PEEK using precision milling in a five-axis CNC machine. PEEK is not seen as a shape-memory polymer, but recent developments mean this can be achieved, which has opened up even further medical applications (Surgical Technologies 2009).
Results and discussion
The recent developments in PEEK have allowed us to develop a new type of retainer using digital scanning of the dentition and then CAD design of the appliance. We are able to produce a milled PEEK retainer wire from NimroDental in London. This exciting material is giving us a high-strength appliance in white shades to allow passive retention of anterior teeth. The thickness of the wire can be set depending on the situation, but a thickness of 0.8 mm seems to be adequate, allowing us to have a thin and comfortable appliance and still have some physiological movement of the teeth. The PEEK retainer wire can be cemented using conventional acid-etch techniques, allowing us to use a familiar method.
Case presentation introduction and presenting situation
A woman, age 45, presented with a completed Invisalign treatment. She was currently using a Vivera-type clear retainer; however, she found it bulky and requested a permanent retainer wire to prevent relapse in the lower anterior segment.
Her treatment options were discussed, including a new Vivera, Essix retainer, NimrodRetainer, conventional bonded lingual wire, or the PEEK fixed retainer. She chose the PEEK wire.
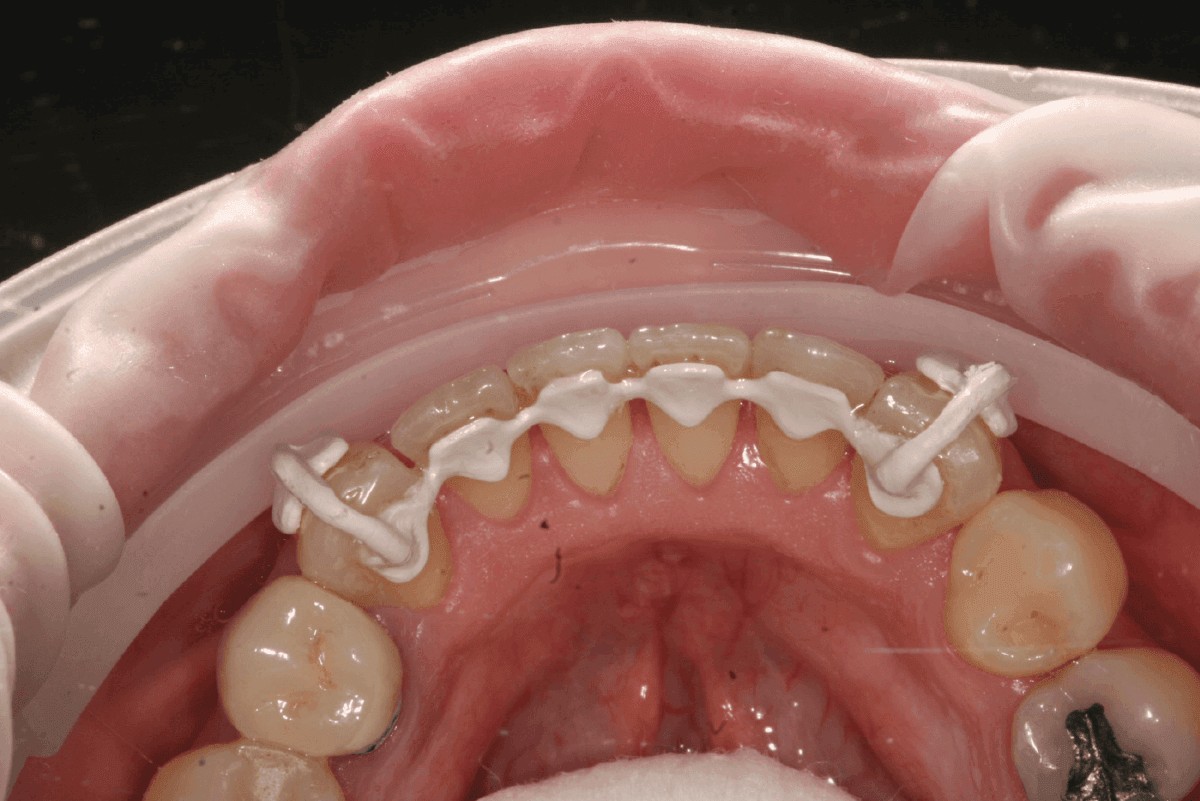
Figure 6: Cementation using conventional acid-etch techniques and flowable resin or warm composite
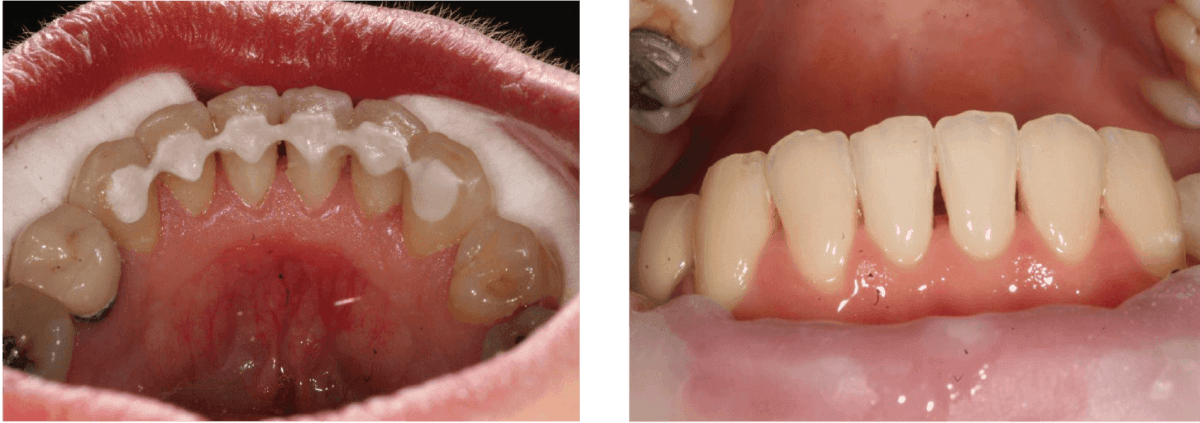
Figure 7: Removal of the PEEK supports after cementation and Figure 8: The appearance after cementation and removal of supports is very discreet in the anterior view
Treatment carried out
The patient was assessed and found to be suitable for the PEEK wire. A digital intraoral scan was carried out using Sirona Cerec Omnicam CEREC Ortho software. The file was uploaded to NimroDental London Dental laboratory where the plan was applied to a digital model.
A 3D-printed model was manufactured, and a PEEK wire was milled. The wire was made with supports on the labial surfaces of LR3 and LL3 in order to allow an easier seating of the wire. It is essential that the wire is fitted passively. The teeth were isolated, etched with 37% phosphoric acid etch gel, and rinsed and bonded using Adhese® Universal VivaPen® from Ivoclar Vivadent® using standard protocol as recommended by the manufacturer.
Adhese Universal VivaPen contains a single-component, light-cured universal adhesive for direct and indirect bonding procedures and is compatible with all etching techniques: self-etch, selective enamel-etch, and total-etch. A total-etch technique rather than self-etch was preferred.
Flowable composite resin Venus® Flow from Kulzer was applied to the labial surfaces of the teeth, and the wire was seated. The resin was light cured from all sides. The lingual supports were removed, and any excess was polished. Articulation was checked for any interferences, and good oral hygiene routines were demonstrated.
Materials used:
- PEEK wire from NimroDental
- Cerec Ortho software was used on a Cerec a/c Omnicam
- Venus Flow from Kulzer
- Adhese Universal VivaPen from Ivoclar Vivadent
Conclusion
NimroDental’s expertise and high-tech machinery make it possible to provide patients with a cost-effective, high-strength, tooth-colored retainer made in biocompatible PEEK that can easily be cemented using standard techniques. It can be produced from an impression or even better completely digitally using intraoral scan techniques. It allows a limited amount of flexibility to maintain normal tooth function.
 Patrik Zachrisson, CertDentImp, FICOI, is a dental surgeon and partner of The Wensleydale Dental Practice (Huntingdon, Cambridgeshire) and the Wensleydale Dental laboratory. He qualified at the Karolinska Institute Sweden in 1996. He provides general dental care for a broad patient base, focusing mainly on digital dentistry, Invisalign® since 2008, implantology, restorative, and preventive dentistry. He is a keen CEREC user and is a Member of the British Dental Association, Member of the International Team of Implantology, Member of the British Academy of Cosmetic Dentistry, and Fellowship status in the International Congress of Oral Implantologists (FICOI).
Patrik Zachrisson, CertDentImp, FICOI, is a dental surgeon and partner of The Wensleydale Dental Practice (Huntingdon, Cambridgeshire) and the Wensleydale Dental laboratory. He qualified at the Karolinska Institute Sweden in 1996. He provides general dental care for a broad patient base, focusing mainly on digital dentistry, Invisalign® since 2008, implantology, restorative, and preventive dentistry. He is a keen CEREC user and is a Member of the British Dental Association, Member of the International Team of Implantology, Member of the British Academy of Cosmetic Dentistry, and Fellowship status in the International Congress of Oral Implantologists (FICOI).
- Arevo Labs announces carbon fiber- and nanotube-reinforced high-performance materials for 3D printing process [news release]. Solvay; March 24, 2014. https://www.solvay.com/en/media/press_releases/20140324-Arevo.html. Accessed February 28, 2018.
- Artun J, Urbye KS. The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. Am J Orthod Dentofacial Orthop. 1988; 93(2):143-148.
- Clark JD, Kerr WJ, Davis MH. CASES — clinical audit; scenarios for evaluation and study. Br Dent J. 1997;183(3):108-111.
- Hegde N, Reddy G, Reddy VP, Handa A. Bonded retainers in orthodontics: a review. Int J Dental Clin. 2011:3(3):53-54
- Heier EE, De Smit AA, Wijgaerts IA, Adriaens PA. Periodontal implications of bonded versus removable retainers. Am J Orthod Dentofacial Orthop. 1997; 112(6):607- 616.
- Hichens L, Rowland H, Williams A, et al. Cost-effectiveness and patient satisfaction: Hawley and vacuum-formed retainers. Eur J Orthod. 2007:29(4):372-378.
- Johnston CD, Littlewood SJ. Retention in orthodontics. Br Dent J. 2015;16;218(3):119-212.
- Kurtza SM, Devine JN. Peek biomaterials in trauma, orthopedic, and spinal implants. Biomaterials. 2007; 28(3): 4845-4869.
- Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop. 1988; 93(5):423- 428.
- Little RM. Stability and relapse of dental arch alignment. Br J Orthod. 1990;17(3):235-241.
- Lumsden KW, Saidler G, McColl JH. Breakage incidence with direct-bonded lingual retainers. Br J Orthod. 1999; 26(3):191-194.
- Parker D, Bussink J, Hendrik T, et al. Polymers, High-Temperature Ullmann’s Encyclopedia of Industrial Chemistry. Weinheim, Germany: Wiley-VCH; April 15, 2012. https://docslide.us/documents/ullmanns-encyclopedia-of-industrial-chemistry-polymers-high-temperature.html. Accessed February 28, 2018
- Sauget E, Covell DA Jr, Boero RP, Lieber WS. Comparison of occlusal contacts with use of Hawley and clear overlay retainers. Angle Orthod. 1997; 67(3):223-230.
- Surgical Technologies; MedShape Solutions, Inc. announces first FDA-cleared shape memory PEEK device [news release]. Medshape; September 23, 2009. https://www.medshape.com/news-events/40-medshape-solutions,-inc-announces-first-fda-cleared-shape-memory-peek-device-closing-of-$10m-equity-offering.html. Accessed February 28, 2018.
- 3D printing high-strength carbon composites using PEEK, PAEK [news release]. Design News; April 14, 2014. https://www.designnews.com/design-hardware-software/3d-printing-high-strength-carbon-composites-using-peek-paek/143795958032579. Accessed February 28, 2018.
- Zachrisson BJ. Third-generation mandibular bonded lingual 3-3 retainer. J Clin Orthod. 1995;29(1):39-48
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
