Drs. Jamie Y. Kim, Chung How Kau, and Ahmet A. Celebi show a patient’s progress through treatment
The presentation of a unilateral posterior crossbite is usually accompanied by a mandibular shift producing a lower midline deviation toward the crossbite side.1,2 Bilateral posterior crossbites often involve true basal skeletal discrepancies in the transverse relationships of the maxilla to the mandible that usually reflect a severe maxillary skeletal constriction rather than mandibular enlargement.
[userloggedin]
Generally, there are no dental midline and facial midline discrepancies in full-occlusion and at-rest positions with any obvious functional deviations observed upon closure in bilateral posterior crossbites.3 Mandibular asymmetries have been the source of multiple debates and significant research. A question frequently addressed in the literature is the source of the asymmetry: Is it predominantly skeletal, dento-alveolar, or a combination of both? Many causes of facial asymmetry have been reported in the literature, as genetics, condylar fractures, condylar hyperplasia or hypoplasia, tumors or ankylosis in the temporomandibular region, prepubertal asymmetries, and asymmetric condylar positioning.4
Asymmetric condylar positioning and asymmetric mandibular growth
Many studies have reported that asymmetric condylar positioning associated with mandibular shifts can be demonstrated on tomograms and transcranial radiographs in the majority of posterior crossbite patterns that present in children.5,6
In the skeletally immature patient with severe asymmetry, the option to treat with maxillary expansion appliances might be the most appropriate choice. In a study, 22 children with a functional posterior crossbite were corrected with maxillary expansion at a mean age of 8.5 years. The condyle on the non-crossbite side was positioned more anterior prior to treatment and moved posteriorly and superiorly after treatment.7 In another study, authors compared condylar and ramal asymmetries in 81 patients with unilateral posterior crossbites to 75 normal occlusive subjects. The results showed patients with unilateral posterior crossbites had more asymmetric condylar positions than the controls. Moreover, the condylar, ramal, and condylar-ramal heights on the crossbite side were smaller than the non-crossbite side.7
 Asymmetric malocclusions can be complicated and challenging to correct, especially when there is an underlying skeletal component.4 Orthodontic treatment alone is a difficult choice in this situation.8 The treatment of patients with an asymmetry that is moderate to severe and with no significant functional limitations may be delayed until skeletal maturity is reached for a definitive orthodontic and/or surgical correction. Despite this, an attempt can be made to control and modify asymmetric growth in patients with active growing time.9 An attempt at early treatment is always the choice as functional shifts establish mal-occlusions and musculo-skeletal function. Often, the latter is difficult to unestablish.
Asymmetric malocclusions can be complicated and challenging to correct, especially when there is an underlying skeletal component.4 Orthodontic treatment alone is a difficult choice in this situation.8 The treatment of patients with an asymmetry that is moderate to severe and with no significant functional limitations may be delayed until skeletal maturity is reached for a definitive orthodontic and/or surgical correction. Despite this, an attempt can be made to control and modify asymmetric growth in patients with active growing time.9 An attempt at early treatment is always the choice as functional shifts establish mal-occlusions and musculo-skeletal function. Often, the latter is difficult to unestablish.
 In this report, we present the orthopedic and orthodontic treatment of a facial asymmetry and unilateral posterior crossbite with severe midline discrepancy in a growing patient.
In this report, we present the orthopedic and orthodontic treatment of a facial asymmetry and unilateral posterior crossbite with severe midline discrepancy in a growing patient.
Case report
Diagnosis and etiology
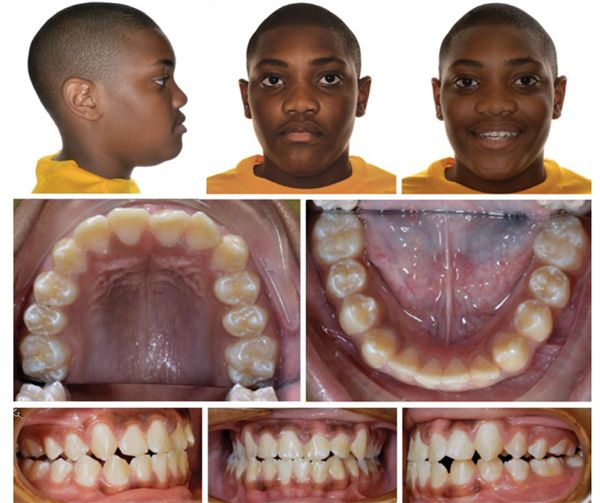
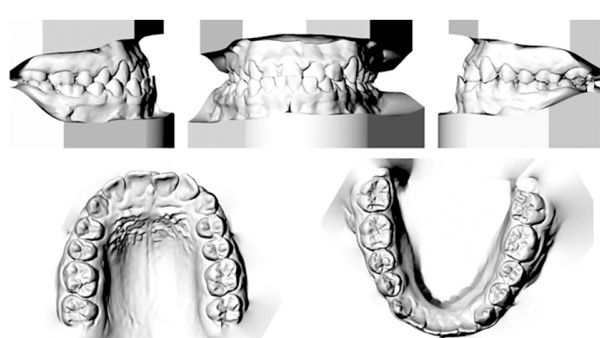
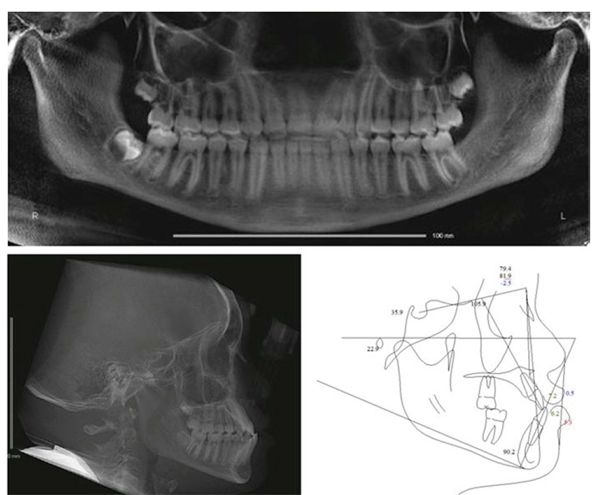
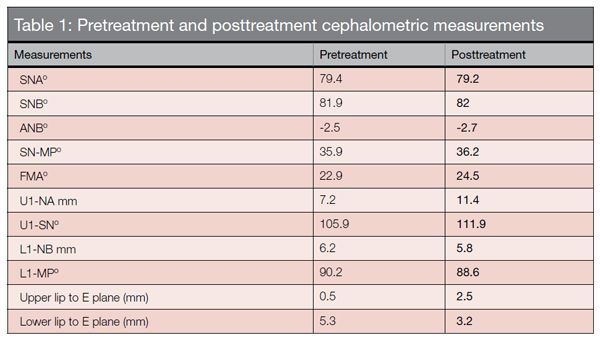
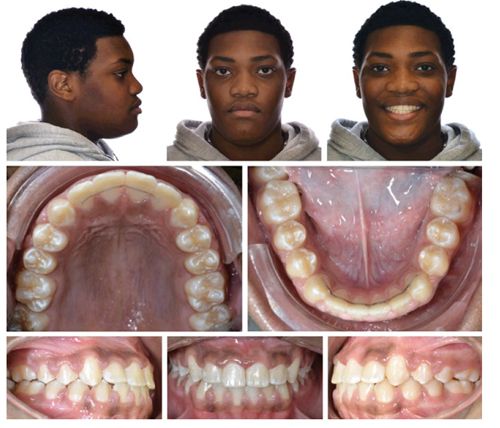
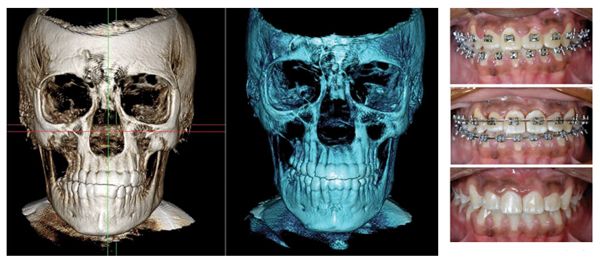
The patient was a 13-year-old African-American male who visited Department of Orthodontics in The University of Alabama at Birmingham for orthodontic consultation. The chief complaint was posterior crossbite on the right side. No specific medical problems or temporomandibular joint symptoms were observed. The clinical exam revealed that he had a Class I molar on the right and a half-step Class III molar on the left. The upper incisors were in negative overjet. In addition, the upper dental midline was deviated 2 mm to the left while the lower dental midline was deviated 4 mm to the right from the midsagittal plane (Figures 1 and 2). Even though a CR-CO shift was suspected, it was impossible to de-program the patient fully at the clinical exam. A CBCT radiograph (Carestream 9500) was taken to verify if a true skeletal mandibular asymmetry was present. A mildly retrusive maxilla and a prognathic mandible contributed to a Class III skeletal relationship (ANB = -2.5). His mandibular plane angle was normal (SN-MP = 35.9°) (Figure 3 and Table 1). The maxilla was skeletally narrow in the transverse dimension. Mild crowding of less than 3 mm existed in the maxillary and mandibular arches. There was Bolton discrepancy with large upper lateral incisors. His facial profile was slightly concave with a normal chin-throat distance and normal nasolabial angle. He showed mild facial asymmetry with deviation of mandible to the right side.
Treatment objectives
The treatment objectives for the dentition were correction of the right posterior cross-bite, to make the maxillary, mandibular, and facial midlines coincident. The treatment objectives for the skeleton and soft tissue were to improve the facial asymmetry, including the deviation of the chin, to correct the transverse discrepancy, and to improve the facial profile by reducing the lower lip protrusion. Thus, facial symmetry, normal overjet and overbite, and Class I canine-to-molar relationships could be obtained.
Treatment progress
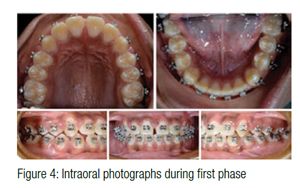
The treatment plan included two phases. During the first phase of treatment, a removable diagnostic bite plate was used. The design included maxillary first molar clasps, no labial bow, an anterior bite ramp, and an acrylic plate covering the palate with an expansion screw embedded in the acrylic. The anterior bite ramp disoccluded his dentition for deprogramming of the jaw. The patient was instructed to wear the appliance full time for 23 days without any expansion. Upper metal brackets from canine-to-canine were bonded, and the expansion was initiated (1 turn/day). A 5.5 mm expansion was achieved by 22 turns, and the posterior crossbite was successfully corrected. The remaining upper and lower teeth were bonded. After 5 months of treatment, the anterior bite plate was removed, and the mandible appeared to be in the new position (Figure 4). During the second phase, treatment continued with fixed orthodontic treatment. The upper archwire progressed to 0.016 x 0.022 Niti, and the lower archwire progressed to 0.020 SS wire. At this time, Class III elastics were worn full time. The wire progression continued to 0.019 x 0.025 SS upper archwire and 0.017 x 0.025 SS reverse Curve of Spee wire on the lower arch to level the Curve of Spee. After 16 months of total treatment, appliances were removed. Maxillary and mandibular retention was performed with fixed retainers.
Figure 7: Posttreatment cephalometric radiograph; Figure 8: Cephalometric superimposition before and after treatmentResults
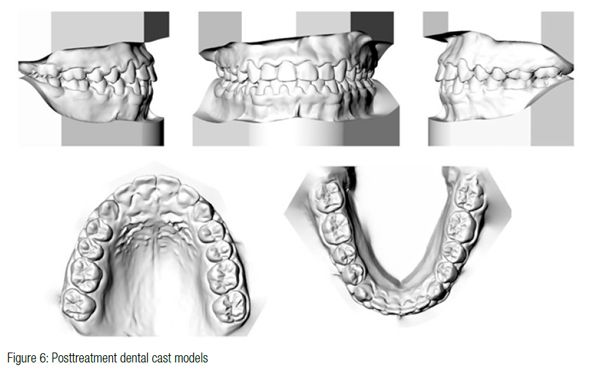
Intraoral photographs obtained after the first phase of treatment are presented in (Figure 4). The final records show that the unilateral posterior crossbite was resolved, and dental midlines were coincident with each other and with the facial midline. (Figures 5 and 6). The skeletal facial asymmetry was corrected by the correction of mandibular shift. Intraorally, a Class I canine and molar relationship with optimal overbite and overjet was achieved. In the comparison of the dental casts before and after treatment, maxillary inter-molar widths increased by 4 mm. Cephalometric superimposition showed A point moved back slightly due to upper anterior lingual torque. Maxillary incisors were proclined and moved forward. Mandibular incisors were slightly retroclined (Figures 7 and 8). A straight profile was achieved with improvement of lower lip to E-line. As shown in the CBCT, deviation of the mandible asymmetry resolved after treatment (Figure 9). Diode laser (NV® Microlaser, DenMat) was used to recontour hyperplastic gingiva (Figure 10). Posttreatment panoramic radiographs showed acceptable root parallelism and developing third molars (Figure 11).
Conclusion
Facial asymmetry with a unilateral crossbite and functional shift of the mandible was treated in a growing patient, due to the expansion of the maxilla and symmetrical repositioning of the mandible. Consideration of a hidden functional shift is important for treatment planning for these patients. Orthognathic surgery may not be necessary in growing patients with functional asymmetries. Minimally invasive treatment can be treatment planned for patients exhibiting unilateral posterior crossbites possessing transverse discrepancies.[/userloggedin]
[userloggedout][/userloggedout]
 Jamie Y. Kim, DMD, MS, received her degree in Doctor of Dental Medicine at the Medical College of Georgia. She completed the Certificate of Orthodontics and Master of Science at the University of Alabama-Birmingham. Dr. Kim is currently practicing in Atlanta, Georgia.
Jamie Y. Kim, DMD, MS, received her degree in Doctor of Dental Medicine at the Medical College of Georgia. She completed the Certificate of Orthodontics and Master of Science at the University of Alabama-Birmingham. Dr. Kim is currently practicing in Atlanta, Georgia.
 Chung How Kau, BDS, MScD, MBA, PhD, MOrth, FAMS, FDSGlas, FFD (Ortho), FDSEdin, FAMS, FICD, is Chairman and Professor at the Department of Orthodontics, The University of Alabama at Birmingham. He is a Diplomate of the American Board of Orthodontics and enjoys practicing clinical orthodontics. He is a researcher with a keen interest in three-dimensional and translational research. Currently, he is Principal Investigator on a number of grants and has a research involvement in excess of $4 million dollars. He actively contributes and publishes in the orthodontic literature and has over 300 peer-reviewed publications, conference papers, and lectures. He was also made the King James IV Professor by the Royal College of Surgeons in Edinburgh, Scotland, in 2011.
Chung How Kau, BDS, MScD, MBA, PhD, MOrth, FAMS, FDSGlas, FFD (Ortho), FDSEdin, FAMS, FICD, is Chairman and Professor at the Department of Orthodontics, The University of Alabama at Birmingham. He is a Diplomate of the American Board of Orthodontics and enjoys practicing clinical orthodontics. He is a researcher with a keen interest in three-dimensional and translational research. Currently, he is Principal Investigator on a number of grants and has a research involvement in excess of $4 million dollars. He actively contributes and publishes in the orthodontic literature and has over 300 peer-reviewed publications, conference papers, and lectures. He was also made the King James IV Professor by the Royal College of Surgeons in Edinburgh, Scotland, in 2011.
 Ahmet A. Celebi, BDS, MSc, PhD, graduated from Marmara University School of Dentistry, Turkey, with a BDS degree. He had completed an MSc degree in Physiology and a PhD in Orthodontics in Kirikkale University, Turkey. Currently, Dr. Celebi is a Postdoctoral fellow in the Department of Orthodontics, The University of Alabama at Birmingham.
Ahmet A. Celebi, BDS, MSc, PhD, graduated from Marmara University School of Dentistry, Turkey, with a BDS degree. He had completed an MSc degree in Physiology and a PhD in Orthodontics in Kirikkale University, Turkey. Currently, Dr. Celebi is a Postdoctoral fellow in the Department of Orthodontics, The University of Alabama at Birmingham.
- Bell RA. Functional posterior crossbites in children. J Pediatric Dent Care. 2005;11(1):28-31.
- Piero AC. Interceptive orthodontics: The need for early diagnosis and treatment of posterior crossbites. Med Oral Patol Oral Cir Bucal. 2006;11:E210-214.
- Bell RA, Kiebach TJ. Posterior crossbites in children: Developmental-based diagnosis and implications to normative growth patterns. Semin Orthod. 2014;20(2).
- Anhoury PS. Nonsurgical treatment of an adult with mandibular asymmetry and unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2009;135(1):118-126.
- Santos Pintos A, Buschang PH, Throckmorton GS, Chen P. Morphological and position asymmetries of young children with functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2001;120:513–520.
- Vitral RW, Fraga MR, Oliveira RS, Vitral JC. Temporomandibular joint alterations after correction of a unilateral posterior crossbite in a mixed-dentition patient: a computed tomography study. Am J Orthod Dentofacial Orthop. 2007;132(9):395-399.
- Hesse KL, Artun J, Joondeph DR, Kennedy DB. Changes in condylar position and occlusion associated with maxillary expansion for correction of functional unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 1997;111(4):410-418.
- Bishara SE, Burkey PS, Kharouf JG. Dental and facial asymmetries: a review. Angle Orthod. 1994;64:89-98.
- Proffit WR. Treatment of orthodontic problems in preadolescent children. In: Reinhardt RW, ed. Contemporary Orthodontics. 2nd ed. St. Louis, MO: Mosby; 1993.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
