Dr. Bradford Edgren illustrates cases where early treatment avoided later complications
 An impacting tooth is any tooth that is unlikely to erupt into its normal position in the mouth prevented by the lack of space, tissue, bone, and/or by another tooth.
An impacting tooth is any tooth that is unlikely to erupt into its normal position in the mouth prevented by the lack of space, tissue, bone, and/or by another tooth.
When discussing early interceptive treatment of potentially impacting teeth, typically the maxillary canines are being addressed since they are most commonly impacted teeth, second only to third molars.
[userloggedin]
1
The maxillary canine has the longest period of development with the most tortuous course of travel from its origin to full eruption of all maxillary teeth.2 Its calcification commences at 4 to 5 months of age, which is approximately the same age as the initiation of calcification of the maxillary central incisor and first molar.3 Eruption of the upper canine doesn’t occur until 11-12 years of age, much later than the eruption of the first molar (6 years of age) and the central incisor (7-8 years of age),3 and is one of the last teeth to erupt into the maxillary dental arch.
It has been hypothesized that the permanent maxillary canine is more susceptible to ectopic eruption and impaction because of its development high up in the most concentrated portion of the alveolus and its relatively late age of eruption.2 A study by Coulter and Richardson4 found that the maxillary canine travels nearly 22 mm from its position at age 5 years to its final position at age 15 years.
However, maxillary canines are not the only impacting permanent teeth that can benefit from early interceptive treatment. Premolars, molars, and incisors can also become potentially impacted at an early age and respond well to early interceptive orthodontic treatment. In the young ortho-dontic patient, many of the permanent tooth roots are not fully formed, and the dentofacial skeleton is more amicable to dentofacial orthopedics. Addressing potentially impacting teeth early provides the opportunity to reduce damage or loss of adjacent permanent teeth, diminish the incidence of ankylosis, provide optimum alveolar bone support and morphology, improved buccal root torque/angulation, and an enhanced overall final result. Leaving a jaw condition untreated until after the eruption of the permanent teeth can result in a dental and/or skeletal discrepancy that is too severe to achieve an ideal or even an acceptable orthodontic result. At that point, if treatment is initiated after all or most of the permanent teeth have erupted, the treatment regimen has to adapt to the already established or nearly established face.5
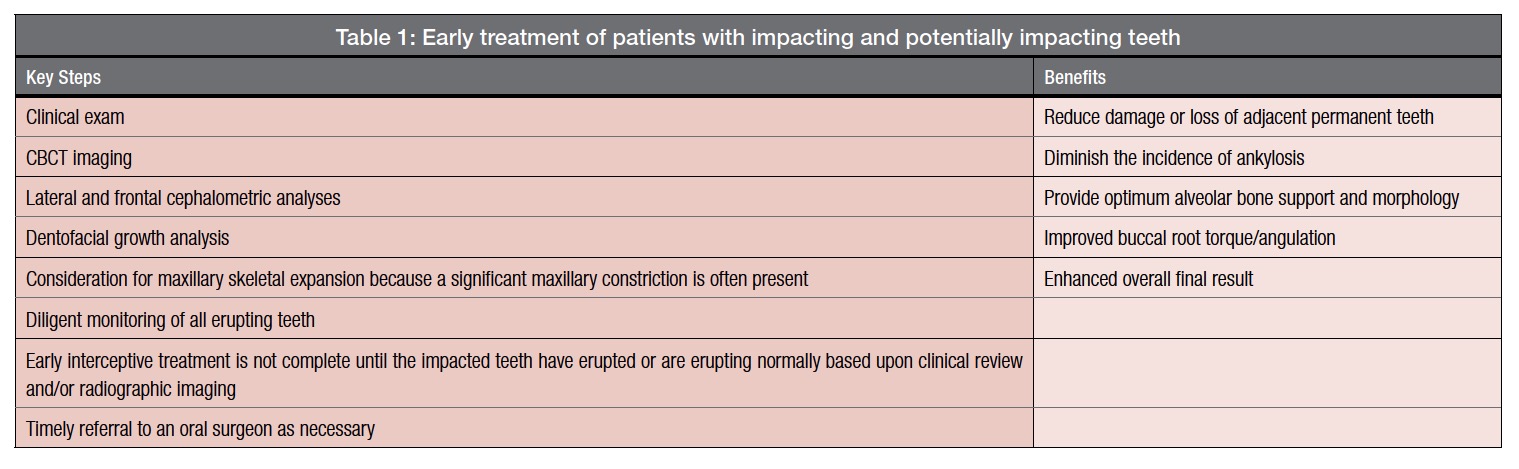
The keys to early intervention of patients with impacting and potentially impacting teeth include a clinical exam, cone beam computed tomography (CBCT) imaging, lateral and frontal cephalometric analyses, dentofacial growth analysis, consideration for maxillary skeletal expansion, diligent monitoring of all erupting teeth, and timely referral to an oral surgeon for tooth exposure as necessary.
CBCT imaging is a key component to comprehending the full extent of a patient’s dentofacial anatomy and determining a diagnosis before embarking on treatment. The better the radiographic imaging, the more complete the diagnosis and understanding of the complexity of the patient’s problem. The availability of CBCT imaging makes traditional panoramic radiography inadequate for evaluating and treating impacting or impacted teeth due to the inherent distortions associated with the traditional technique. Traditional panoramic images do not provide the subtle details of tooth position, root form, and dentoalveolar width necessary to diagnosis and treat impacting teeth.6 The “power of slices” provided by CBCT allows the clinician to thoroughly evaluate the mesiodistal, buccolingual, and vertical orientations of all unerupted teeth. Canines that might appear to be resorbing the lateral incisor roots on a traditional panoramic radiograph may actually be just buccally or palatally positioned to lateral incisor root with no resorption evident when analyzed with CBCT.
Future dentofacial growth is another key factor that requires consideration for all young orthodontic patients. Patients with the potential for growth should always have lateral cephalometric and dentofacial growth analyses performed. Many of these patients with impacting maxillary teeth suffer from horizontal and transverse maxillary hypoplasia and therefore have the potential for relative excessive mandibular growth.
 McConnell, et al., established that patients with maxillary canine impactions demonstrated a profound transverse anterior arch deficiency.7 Schindel and Duffy also stated that patients possessing a transverse discrepancy are more likely to have an impacted maxillary canine than those without the transverse deficiency.8 They also stated that the early mixed dentition is the best time to assess a patient for potential canine impaction. Imprudent permanent maxillary tooth extraction can exacerbate anterior and posterior crossbites following the full expression of facial growth.
McConnell, et al., established that patients with maxillary canine impactions demonstrated a profound transverse anterior arch deficiency.7 Schindel and Duffy also stated that patients possessing a transverse discrepancy are more likely to have an impacted maxillary canine than those without the transverse deficiency.8 They also stated that the early mixed dentition is the best time to assess a patient for potential canine impaction. Imprudent permanent maxillary tooth extraction can exacerbate anterior and posterior crossbites following the full expression of facial growth.
Maxillary expansion should be routinely considered because of the high likelihood of a maxillary skeletal constriction and the need for a complete diagnosis, including the frontal analysis.5,9 Consequently, injudicious extraction of deciduous teeth in these young patients without early active orthodontic treatment is ill-advised. Bazargani, et al., found a significant decrease in maxillary arch length occurred at sites where deciduous canines were extracted with palatally displaced canines compared to controls.10
Active early interceptive treatment of patients with impacted and/or impacting teeth is not complete until the teeth are erupting normally based upon clinical review and/or radiographic imaging. If it becomes evident that the course of eruption of the teeth in question does not improve in a timely fashion, and damage to adjacent teeth is imminent, then a referral to an oral surgeon for early exposure and bonding with a gold chain for guided eruption techniques is warranted. Moreover, since these patients typically possess significant maxillary skeletal constrictions, diligent monitoring of all erupting teeth is necessary because additional permanent teeth can become impacted.
Case report 1

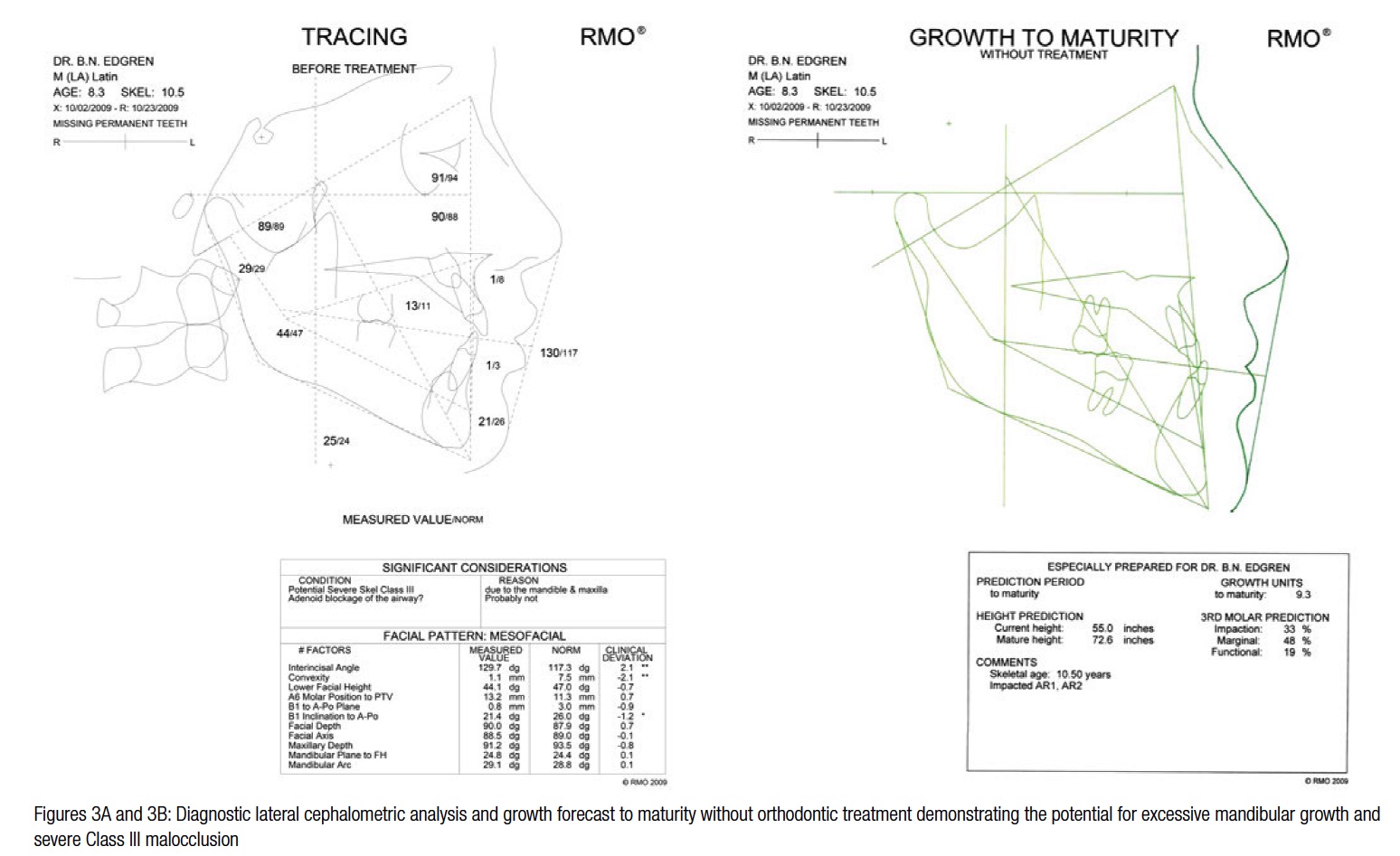
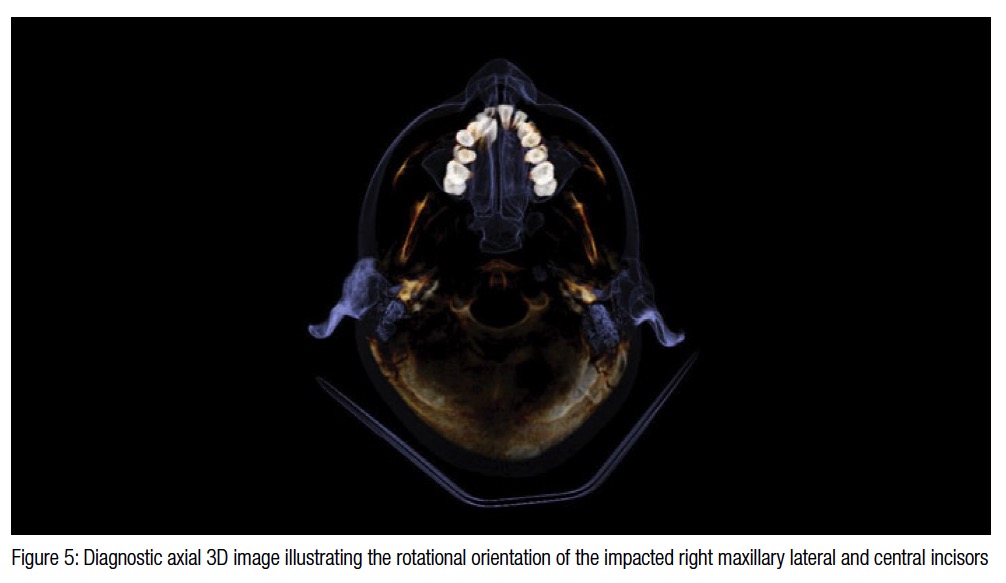 This 8-year 4-month-old male presented with severely impacted maxillary right lateral and central incisors (Figures 1-2). His case illustrates that maxillary permanent teeth can impact at an early age and benefit from a thorough diagnostic evaluation. This was his second opinion with the original treatment plan necessitating extraction of the impacted incisors and implant replacement after the completion of dentofacial growth. His CBCT scan, taken on an i-CAT™ Next Generation scanner (Imaging Sciences International), and Ricketts’ lateral and frontal cephalometric analyses and growth forecast, performed by Rocky Mountain Orthodontics Data Services® (RMODS®), indicated a potential for a severe skeletal Class III malocclusion due to the mandible and maxilla, a skeletal lingual crossbite pattern due to the maxilla, the need for extended treatment due to probable excessive mandibular growth resulting in an anterior crossbite, and severe Class III malocclusion (Figures 3-5). Extraction of the impacted right maxillary incisors would only have exacerbated the potentially developing Class III malocclusion, and would have had a devastating outcome for this patient.
This 8-year 4-month-old male presented with severely impacted maxillary right lateral and central incisors (Figures 1-2). His case illustrates that maxillary permanent teeth can impact at an early age and benefit from a thorough diagnostic evaluation. This was his second opinion with the original treatment plan necessitating extraction of the impacted incisors and implant replacement after the completion of dentofacial growth. His CBCT scan, taken on an i-CAT™ Next Generation scanner (Imaging Sciences International), and Ricketts’ lateral and frontal cephalometric analyses and growth forecast, performed by Rocky Mountain Orthodontics Data Services® (RMODS®), indicated a potential for a severe skeletal Class III malocclusion due to the mandible and maxilla, a skeletal lingual crossbite pattern due to the maxilla, the need for extended treatment due to probable excessive mandibular growth resulting in an anterior crossbite, and severe Class III malocclusion (Figures 3-5). Extraction of the impacted right maxillary incisors would only have exacerbated the potentially developing Class III malocclusion, and would have had a devastating outcome for this patient.
His early interceptive orthodontic treatment plan included maxillary expansion with a bonded expander, fixed appliances, and timely referral to the oral surgeon for exposure of the right central incisor and canine that were bonded with gold chains for guided eruption techniques. Shortly after the cessation of active maxillary expansion, the right later incisor erupted, eliminating the need for surgical exposure. The expander was removed after 9 months, and the right canine and central incisor were exposed and bonded. After 15 months of treatment, the canine and central incisor erupted.
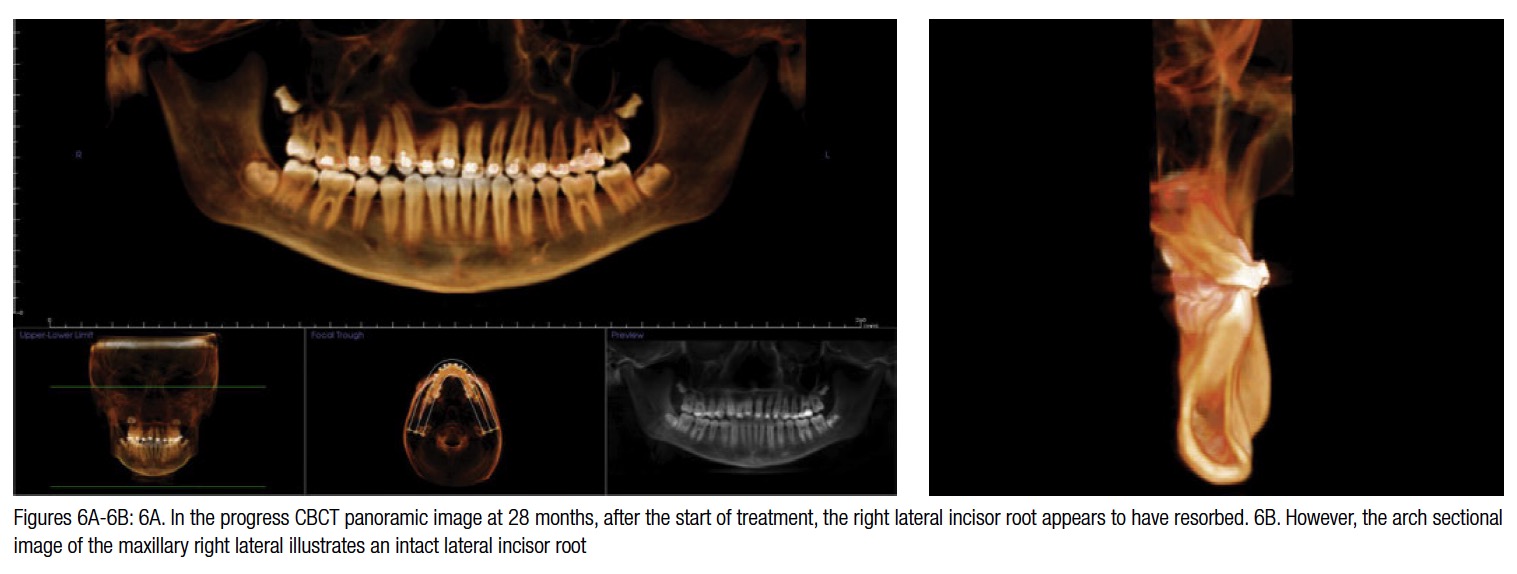

 Twenty-eight months after the start of treatment, a progress CBCT scan was taken. Initially, it appears as though the right lateral incisor root has suffered significant resorption (Figure 6A). Upon further inspection, via the “power of slices” with CBCT imaging, it is evident that the lateral incisor root is severely proclined due to the initial positions of the canine and central incisor, but the root is fully intact with no resorption (Figure 6B). It would take a total of 46 months of orthodontic treatment to upright the right maxillary lateral incisor while competing against his excessive mandibular jaw growth (Figures 7 and 8). Follow-up care on this patient will only require comprehensive orthodontic treatment including additional maxillary expansion and fixed appliances. Timely early interceptive treatment, with guided eruption of the maxillary right canine and central incisor, no longer results in a severe skeletal class III malocclusion, anterior crossbite, damage to adjacent teeth, or the need for implants.
Twenty-eight months after the start of treatment, a progress CBCT scan was taken. Initially, it appears as though the right lateral incisor root has suffered significant resorption (Figure 6A). Upon further inspection, via the “power of slices” with CBCT imaging, it is evident that the lateral incisor root is severely proclined due to the initial positions of the canine and central incisor, but the root is fully intact with no resorption (Figure 6B). It would take a total of 46 months of orthodontic treatment to upright the right maxillary lateral incisor while competing against his excessive mandibular jaw growth (Figures 7 and 8). Follow-up care on this patient will only require comprehensive orthodontic treatment including additional maxillary expansion and fixed appliances. Timely early interceptive treatment, with guided eruption of the maxillary right canine and central incisor, no longer results in a severe skeletal class III malocclusion, anterior crossbite, damage to adjacent teeth, or the need for implants.
Case report 2

 This 8-year-old female initially presented with severe crowding, premature loss of the maxillary right deciduous canine and right first deciduous molar, and partial anterior crossbite (Figure 9).
This 8-year-old female initially presented with severe crowding, premature loss of the maxillary right deciduous canine and right first deciduous molar, and partial anterior crossbite (Figure 9).
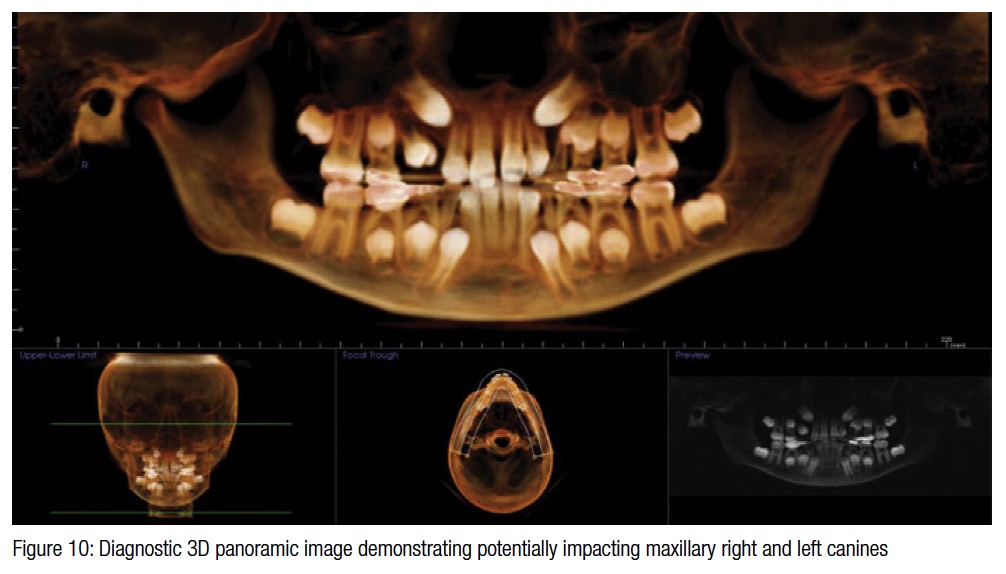
Review of her CBCT imaging, lateral, frontal, and dentofacial growth analyses revealed significant mandibular retrognathia, tendency for a skeletal open bite, and lingual crossbite pattern due to both jaws, and potentially impacting maxillary canines (Figure 10).
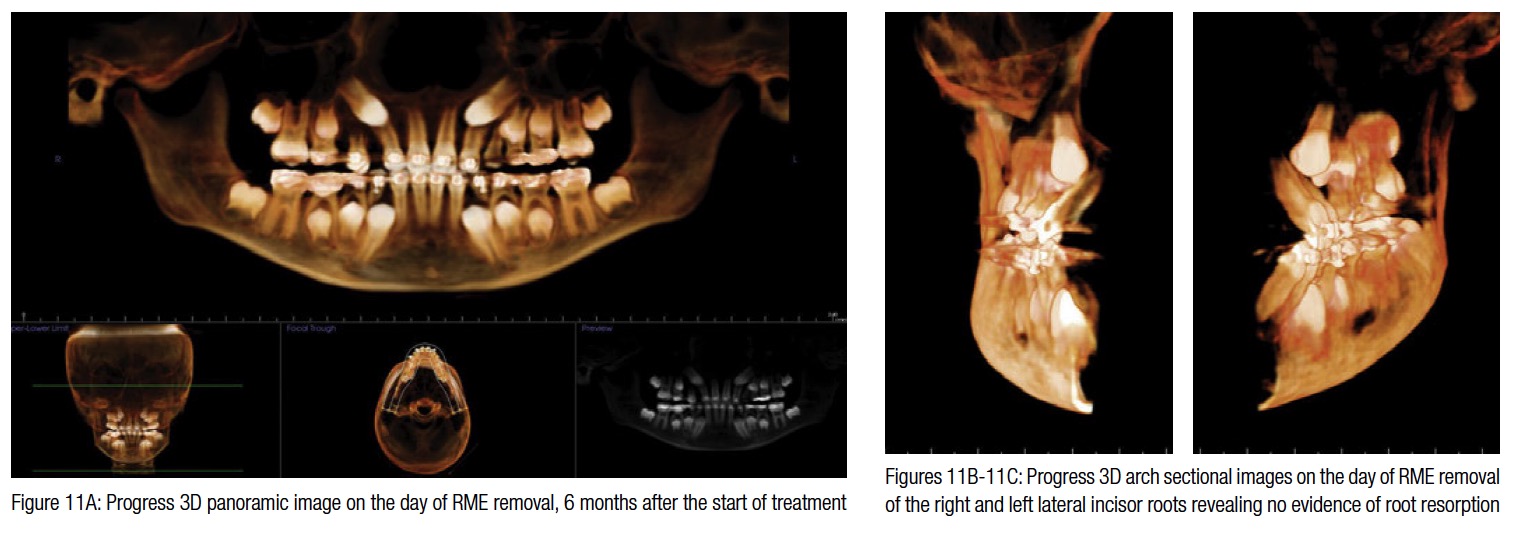
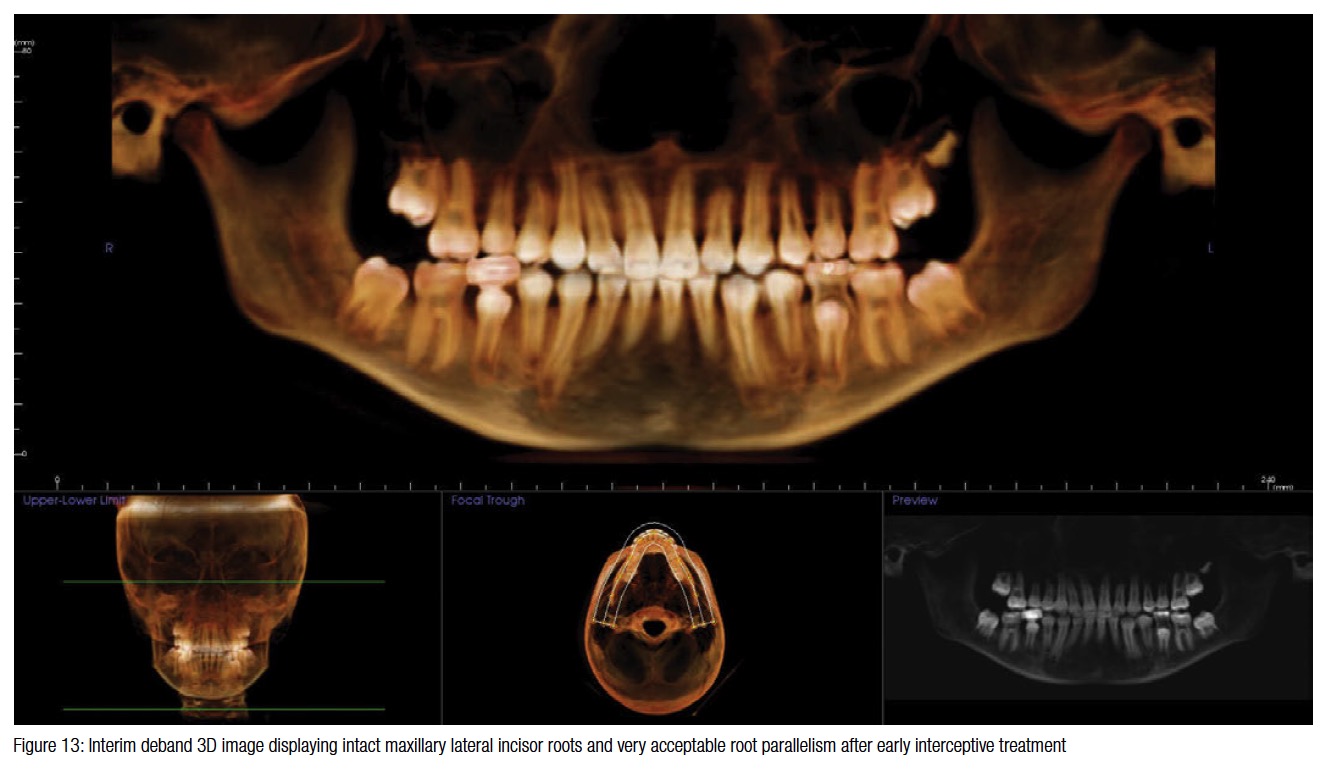
Her early interceptive treatment involved maxillary expansion with a bonded expander and fixed appliances to create space for the potentially impacting canines. Six months after the start of treatment, her expander was removed, and a CBCT scan was taken to monitor the eruption paths of the canines (Figure 11A). The CBCT imaging revealed that the canines were continuing upon their same, potentially destructive, eruption paths and consequently, she was referred to the oral surgeon for exposure and bonding of the canines for guided eruption. CBCT imaging is invaluable in cases like this one since it not only revealed the buccal position of the canines but also that the incisor roots were intact (Figures 11B and 11C). Note that even with maxillary expansion, it is evident that canine impaction was imminent. Successful surgical exposure of the canines is more reproducible with improved imaging. Bilateral exposure of the canines was accomplished 6 weeks after expander removal. Elastic cord was attached to the gold chains and the upper archwire. Nine months after surgery, 16 months after the start of treatment, the canines erupted. The patient was debanded 29 months after the initiation of treatment, and the result was maintained with upper and lower removable Hawley retainers (Figures 12 and 13). The possibility of damage to the adjacent lateral incisor roots and/or permanent tooth extraction would have likely occurred without early treatment.
 Note that not all early treatment cases with impacting or potentially impacting teeth require surgical intervention. See Case report 2 from the CE article “The fundamental objectives of early interceptive treatment” in the 2015 January/February edition of Orthodontic Practice US.5 In that case report, early interceptive treatment prevented the impaction of both maxillary canines and significantly improved the eruption path without surgical exposure.
Note that not all early treatment cases with impacting or potentially impacting teeth require surgical intervention. See Case report 2 from the CE article “The fundamental objectives of early interceptive treatment” in the 2015 January/February edition of Orthodontic Practice US.5 In that case report, early interceptive treatment prevented the impaction of both maxillary canines and significantly improved the eruption path without surgical exposure.
Patients such as these can be extremely challenging, but the rewards for the patient and the orthodontist are immeasurable. Remember, we are treating patients who will be using their smiles for a lifetime.
 Bradford Edgren, DDS, MS, earned both his Doctorate of Dental Surgery, as Valedictorian, and his Master of Science in Orthodontics from the University of Iowa, College of Dentistry. He is a Diplomate, American Board of Orthodontics, and a member of the Southwest Component of the Edward H. Angle Society. Dr. Edgren has presented nationally and internationally to numerous orthodontic groups on the importance of orthodontic diagnosis, early interceptive orthodontic treatment, CBCT, and upper airway obstruction. He has been published in AJO-DO, the American Journal of Dentistry, as well as other orthodontic publications. Dr. Edgren currently has a private practice in Greeley, Colorado. Disclosure: Currently, Dr. Edgren is not receiving compensation from RMO on this appliance.
Bradford Edgren, DDS, MS, earned both his Doctorate of Dental Surgery, as Valedictorian, and his Master of Science in Orthodontics from the University of Iowa, College of Dentistry. He is a Diplomate, American Board of Orthodontics, and a member of the Southwest Component of the Edward H. Angle Society. Dr. Edgren has presented nationally and internationally to numerous orthodontic groups on the importance of orthodontic diagnosis, early interceptive orthodontic treatment, CBCT, and upper airway obstruction. He has been published in AJO-DO, the American Journal of Dentistry, as well as other orthodontic publications. Dr. Edgren currently has a private practice in Greeley, Colorado. Disclosure: Currently, Dr. Edgren is not receiving compensation from RMO on this appliance.
- Shah RM, Boyd MA, Vakil TF. Studies of permanent tooth anomalies in 7,886 Canadian individuals. I: impacted teeth. Dent J. 1978;44(6):262-264.
- Dewel BF. The upper cuspid: its development and impaction.Angle Orthod. 1949;19(2):79-90.
- Fuller JL, Denehy GE. Concise Dental Anatomy and Morphology. 2nd ed. Chicago, IL: Year Book Medical Publishers; 1984: 55, 81, 139.
- Coulter J, Richardson A. Normal eruption of the maxillary canine quantified in three dimensions. Eur J Orthod. 1997;19(2):171-183
- Edgren BN. The fundamental objectives of early interceptive treatment. Ortho Practice US. 2015;6(1):26-33.
- Mah J. Straight talk: Instruction on CBCT in orthodontic graduate education. Orthotown. Sept 2010:47-48.
- McConnell TL, Hoffman DL, Forbes DP, Janzen EK, Weintraub NH. Maxillary canine impaction in patients with transverse maxillary deficiency. ASDC J Dent Child. 1996;63(3):190–195.
- Schindel RH, Duffy SL. Maxillary transverse discrepancies and potentially impacted maxillary canines in mixed-dentition patients. Angle Orthod. 2007;77(3):430-435.
- Miner RM, Al Qabandi S, Rigali PH, Will LA. Conebeam computed tomography transverse analysis. Part 1: Normative data. Am J Orthod Dentofacial Orthop. 2012;142(3):300-307.
- Bazargani F, Magnuson A, Lennartsson B. Effect of interceptive extraction of deciduous canine on palatally displaced maxillary canine: a prospective randomized controlled study. Angle Orthod. 2014;84(1):3–10.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
