Drs. Mohamed Abd El-Ghafour, Noha Ali El-Ashmawi, Amr Ragab El-Beialy, Mona M. Salah Fayed, and Faten Hussein Kamel Eid investigate the effect of low level laser therapy (LLLT) on the rate of maxillary canine retraction
Abstract
Objectives: This split-mouth randomized controlled trial investigates the effect of low level laser therapy (LLLT) on the rate of maxillary canine retraction.
[userloggedin]
Materials/Methods: Eligibility criteria included malocclusion that required extraction of the maxillary first premolar and canine retraction, maximum anchorage requirement, good oral hygiene, and medically free patients. Each patient received LLLT on one side during canine retraction, while the other served as the control. NiTi coil springs delivering 150 gm of force retracted the canines. LLLT with active medium indium gallium arsenide (InGaAs). Semiconductor diode and energy density of 29.3 J/cm2 was applied buccally. LLLT was applied every week for the first 4 weeks, then every 2 weeks till the end of the 4-month study. On each visit of laser application, impressions were made to produce dental models to assess the rate of canine retraction. The primary outcome compared the rate of canine retraction between the laser and control sides; the secondary outcome measured molar anchorage loss. Randomization was done by concealed allocation of the computer-generated sequence in opaque sealed envelopes. Blinding to the assessors was performed, which was not applicable to the patients and operators. Results: Twenty-two patients (19 females and 3 males with mean age of 21.45 (±3.23) years) were randomized with ratio 1:1, and no patients were lost during the 4-month follow-up. The distance traveled by the canine on the laser sides was 3.823 (±1.39) mm, while the control side was 3.832 (±1.91) mm. Molar anchorage loss on the laser side was 1.009 (±1.41) mm and 1.177 (± 1.54) mm on the control sides. No statistically significant difference was found between the two sides in the canine and molar distances traveled. The detected harm was seen in three patients, who had a burn vesicle at the site of laser application, which completely healed after 2 weeks. Limitations: The only considered limitation in this study was the disability to blind both the participants and the operator, but blinding to the assessor was done. Conclusions/Implications: LLLT application was not able to accelerate orthodontic tooth movement according to the protocol used in the present study.
Registration: This trial was not registered.
Protocol: The protocol was not published before trial initiation.
Funding: No funding or conflict of interest to be affirmed.
Introduction
One of the disadvantages of orthodontic treatment is the duration of treatment, which averages around 23.5 months.1 Extended treatment increases the risk of white spot lesions, caries,2,3 inflammatory root resorption,4 gingival inflammation, and periodontal breakdown5 as well as decreasing the patients’ compliance.6
Clinicians have used several methods to accelerate orthodontic tooth movement:
- Pharmacological approaches using prostaglandins,7 interleukins,8 leukotrienes,9 cyclic adenosine monophosphate,10 vitamin D,11 and platelet-rich plasma12
- Physical approaches such as applying direct electrical current,13 pulsed electromagnetic field,14 samarium-cobalt magnet,15 and low- intensity pulsed ultrasound16
- Surgical approaches by performing gingival fiberotomy,17 alveolar surgery,18 distraction osteogenesis,19 and corticotomy20
The idea of lasers started in 1917 with Einstein21 and Bohr,22 and then multiple modifications were done till the 1960s when Maiman23 and Goldman24 introduced the laser in dentistry. The versatile properties of lasers encouraged orthodontists to use it for etching, bonding, debonding, pain control, and soft tissue cutting, e.g., gingivoplasty, frenectomy, and exposure of impacted teeth.25
Low level laser offers orthodontists another use.25 LLLT is also known as “soft laser therapy,” “cold laser,” “low energy laser therapy (LELT),” and “low intensity laser therapy (LILT)”26. LLLT provides another physical approach, ostensibly to accelerate orthodontic tooth movement.25 This acceleration claim is based on its biostimulatory effect.27
The orthodontic literature encompasses controversial results regarding the effect of LLLT on acceleration of orthodontic tooth movement. By using variable energy density, application protocol, and sites, some studies28-43 found that LLLT accelerated tooth movement while others44-50 had opposite results. Several systematic reviews51-56 have been published that evaluate its effect on acceleration of tooth movement. No conclusions were reached due to the low and medium quality of the present evidence. All of these systematic reviews recommended a high-quality randomized controlled trial to reach a conclusion regarding the effectiveness of LLLT as a method of accelerated tooth movement.
Specific objectives or hypotheses
Accordingly, this study aimed to detect the effect of LLLT on accelerated tooth movement via canine retraction as a research model in a split-mouth randomized controlled trial.
Materials and methods
Trial design and any changes after trial commencement
The study design provided a split-mouth randomized controlled trial with assessment of the two sides with two parallel groups with an allocation ratio of 1:1.
Participants, eligibility criteria, and settings
This study selected participants according to the following inclusion criteria: age range from 18 years to 25 years, malocclusion that required extraction of the maxillary first premolars and canine retraction (e.g., bimaxillary dentoalveolar protrusion and Class II Division 1 malocclusion), maximum anchorage requirement, all permanent teeth were present and fully erupted with the exception of the maxillary and mandibular third molars, good oral hygiene and periodontal condition, and medically free subjects with no long-term use of any drugs. Exclusion criteria comprised medically compromised patients, patients suffering from any periodontal disease, patients who had undergone previous orthodontic treatment, and syndromic patients. The study was carried out in the outpatient clinic of the Department of Orthodontics and Dentofacial Orthopedics, Faculty of Oral and Dental Medicine, Cairo University. No changes to methods after trial commencements occurred
Interventions
 Preparatory phase: The 22 recruited participants (19 females and three males with mean age of 21.45 (±3.23) years) received a conventional fixed orthodontic appliance; Roth prescription slot 22 mil × 28 mil (Ormco Mini 2000 brackets). The brackets were bonded to the labial surface of the upper teeth using orthodontic composite resin (Grēngloo™ two-way color change adhesive for metal brackets, Ormco). Ready-made molar bands (Ormco ready-made bands) with two buccal tubes (main and auxiliary) were selected, fitted, and cemented on the maxillary first molars using glass ionomer cement. The archwire sequence in the initial leveling and alignment stage was tailored according to each case until insertion of the stainless steel archwire, 16 x 22 mil (Figure 1).
Preparatory phase: The 22 recruited participants (19 females and three males with mean age of 21.45 (±3.23) years) received a conventional fixed orthodontic appliance; Roth prescription slot 22 mil × 28 mil (Ormco Mini 2000 brackets). The brackets were bonded to the labial surface of the upper teeth using orthodontic composite resin (Grēngloo™ two-way color change adhesive for metal brackets, Ormco). Ready-made molar bands (Ormco ready-made bands) with two buccal tubes (main and auxiliary) were selected, fitted, and cemented on the maxillary first molars using glass ionomer cement. The archwire sequence in the initial leveling and alignment stage was tailored according to each case until insertion of the stainless steel archwire, 16 x 22 mil (Figure 1).
Anchorage preparation and premolar extraction: In order to obtain maximum anchorage, a mini-screw (HUBIT orthodontics, Korea [1.6 × 8 mm]) was inserted between the maxillary second premolar and first molar at the level of the mucogingival junction. Indirect anchorage used an L-shaped 19 × 25 mil stainless steel wire in the auxiliary tube of the maxillary first molar band (cinched back) and connected to the mini-screw with a composite ball (Figure 2). The oral surgery department extracted the maxillary first premolars.
 Canine retraction: Stainless steel ligature ties minimized ligation friction during canine retraction on the active and control sides. ANiTi closed coil spring (Ormco) delivering a force of 150 gm calibrated using Correx tension gauge (Haag-Streit Diagnostics), extending from the hook of the first permanent molar tube to the hook of the canine bracket retracted the canines. The coil was checked every appointment to maintain a constant amount of force.
Canine retraction: Stainless steel ligature ties minimized ligation friction during canine retraction on the active and control sides. ANiTi closed coil spring (Ormco) delivering a force of 150 gm calibrated using Correx tension gauge (Haag-Streit Diagnostics), extending from the hook of the first permanent molar tube to the hook of the canine bracket retracted the canines. The coil was checked every appointment to maintain a constant amount of force.
LLLT application: LLLT with active medium InGaAs (indium gallium arsenide) semi-conductor diode (Epic™ 10 Console, Biolase), wavelength of 940 nm, power density of 1.43 W/cm2 and energy density of 29.3 J/cm2 was applied buccally at the level of the middle third of the canine root (Figure 3). LLLT was applied once/week in the first 4 weeks, then once every 2 weeks until the end of the 4-month study. On each visit of laser application, alginate impressions were made to assess the rate of canine retraction.
Data collection
The dental models identified the landmarks and lines shown in Figure 4. To overcome the curvature of the palatal vault, the models were 2D scanned using a Xerox machine with 1:1 proportion after the above landmarks were marked with 0.7 black marker, which produced a flat image upon which the measurements were made between the canine lines and the third rugae lines bilaterally and between the molar lines and the third rugae lines bilaterally. Measurements were made with a digital caliper.
 A CBCT scan made immediately before canine retraction and after 4 months of active canine retraction captured the three dimensional movement of the canines. The CBCT field of view is restricted to the maxilla, with minimal CBCT machine parameters settings. The distance traveled by the canine cusp tip was measured from the frontal reference plane at the pre-and post- retraction time points (Figure 5).
A CBCT scan made immediately before canine retraction and after 4 months of active canine retraction captured the three dimensional movement of the canines. The CBCT field of view is restricted to the maxilla, with minimal CBCT machine parameters settings. The distance traveled by the canine cusp tip was measured from the frontal reference plane at the pre-and post- retraction time points (Figure 5).
Outcomes (primary and secondary) and any changes after trial commencement
The primary outcome of this trial was to detect the rate of canine retraction on both the LLLT and control sides and to compare between them. Molar anchorage loss was the secondary outcome. There were no outcome changes after the trials began.
Sample size calculation
Sample size was calculated using PS-power and sample size calculator. The input data was extracted from a similar study done by Doshi-Mehta and Bhad-Patil42 describing the rate of canine retraction per 3 months for the control and laser applied groups, where The Type I error probability for a two sided test α = 0.05, power = 0.8. A difference in population means δ = 0.32, and for dependent tests σ is within group standard deviation = 0.45. Based on the aforementioned data, sample size calculation yielded 18 subjects, and thus, 22 subjects were selected for the study to avoid attrition bias.
Interim analyses and stopping guidelines
No interim analyses were performed. The study protocol called for stoppage of the trial if any patient suffered complications such as unusual discomfort.
Randomization
Randomization was done in three steps: a) Sequence generation: done with computer-generated random numbers using a Microsoft Office Excel 2007 sheet. The first column contained numbers 1 to 20, then the second column select function RAND() generated the randomization number. Sorting these numbers was done according to the randomization number, which randomly distributed the first column numbers. The first 10 random numbers comprised the laser group and second 10 as the control group. b) Allocation concealment: The randomization numbers produced from the sequence generation were written on opaque papers and folded 4 times, sealed in opaque envelopes, and kept in a box till the time of implementation (the day of premolar extractions). c) Implementation: On the day of extraction and first day of laser application, each subject chose one of the envelopes to detect his/her number for the randomization sequence and to select the laser and control sides. The principle operator had the code for each patient’s laser and control sides and had the responsibility for making the laser application and impressions.
Blinding
Blinding was done for the assessors, where the first assessor carried on the measurements blindly on both sides using each patient’s dental models and then repeated the measurements after 2 weeks to calculate the intraobserver error. The second assessor made the same measurements blindly to calculate the interobserver error. Since patients and operators would know about the laser application, blinding did not occur for them.
Statistical analysis (primary and secondary outcomes, subgroup analyses)
Statistical analysis was performed by SPSS in general (version 17), while Microsoft Office Excel handled data and graphical presentation. The variables were described by the Mean and Standard Deviation (SD). Kolmogorov-Smirnova, and Shapiro-Wilk tests of normality tested the normality hypothesis of all quantitative variables for further choice of appropriate parametric and non-parametric tests. Paired sample t test and Wilcoxon Signed Ranks Test were used for testing pre–post measurements within the same group while paired t tests and Mann-Whitney U tests were used for comparing the mean changes between the two groups. Significance occured at P < 0.05 (S); while P < 0.01 was considered highly significant (HS).
Results
Participant flow
Since the design was a split mouth, each group (laser and control) numbered 22. After randomization, no participants dropped from the study. A total of 222 out of 242 laser applications and dental models were made for the recruited subjects. Twenty laser applications and dental models were dropped due to missed appointments.
Baseline data
The split-mouth design matched the two groups regarding the baseline characteristics: age, gender, malocclusion, periodontal condition, and medical condition.
Outcomes and estimation
Laser side: The mean differences between each reading and the baseline reading of distance traveled by the canine on the laser side were analyzed (Figure 6). Generally, there was a statistically significant difference between the distances measured from the canine tip to the reference landmark in all the stages of canine retraction. The distances measured from the canine tip to the reference landmark decreased along the path of the canine distally except in 2nd week and 13th week. Along the 4-month trial period, the canine moved distally by 3.823 mm. The daily rate of canine movement on the laser sides is shown in Table 1. The period of the highest rate of canine retraction occurred in the 5th, 7th, 9th, and 11th week.
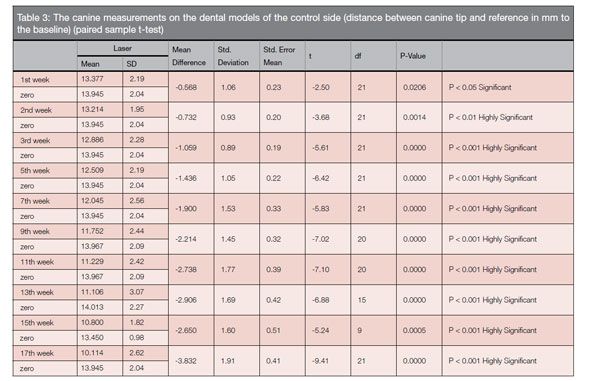
Control side: On the control side, a statistically significant difference occurred between the distances measured from the canine tip to the reference landmark in all the stages of canine retraction (Figure 7). The distances measured from the canine tip to the reference landmark decreased along the path of the canine distally except 15th week only. Along the 4-month trial period, the canine moved distally by 3.832 mm. The daily rate of canine movement in the control side is shown in Table 1. The period of the highest rate occurred in the 3rd, 5th, 7th, 9th, and 11th weeks.
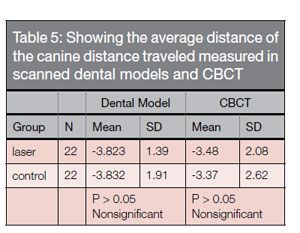
 Laser versus control: By comparing the differences in distances traveled by the canine to the baseline measurement between the two sides, no statistically significant differences occurred between the two sides (Table 2). The difference between the distances moved by the maxillary canines on the laser and control sides to the baseline were the highest at the 3rd week and 15th week. Comparing the distance traveled by the canine via the two measuring modalities; scanned dental models and CBCT, yielded
Laser versus control: By comparing the differences in distances traveled by the canine to the baseline measurement between the two sides, no statistically significant differences occurred between the two sides (Table 2). The difference between the distances moved by the maxillary canines on the laser and control sides to the baseline were the highest at the 3rd week and 15th week. Comparing the distance traveled by the canine via the two measuring modalities; scanned dental models and CBCT, yielded
a minimal difference (Table 3).

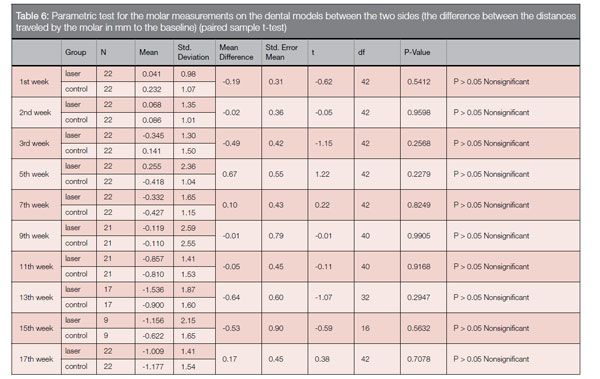
Molar anchorage loss: Molar anchorage loss (Table 4) on the laser side was 1.009 (±1.41) mm and 1.177 (± 1.54) mm on the control sides, which were statistically significant, but no statistical significant difference was found comparing the two sides.
In one session, three patients suffered burn vesicles at the site of laser application, which healed uneventfully in 2 weeks.
Discussion
The inability to blind both the participants and the operator provided a limitation, but blinding of the assessor eliminated the detection bias.
One might consider the external validity and applicability of this trial’s results limited since it is a single center study. Also, the energy density and protocol of LLLT need more definition to reach values that allow decisive conclusions regarding its effectiveness.
Main findings in the context of the existing evidence — interpretation
This trial’s protocol was designed according to SPIRIT 2013 explanation and elaboration: guidance for protocol of clinical trials.57 Following the SPIRIT reporting guidelines helps in minimizing the risk of bias and increases the reliability of the results.
The primary outcome assessed the maxillary canine distance traveled along time interval (i.e., rate of canine movement) on both the laser and control sides. Canine movement can be explained from two points of view; Nanda58 offers a mechanical explanation that describes the four phases of canine retraction via sliding mechanics. Burstone,59 Pilon, et al.,60 and van Leeuwen, et al.,61 describe the biological basis of canine retraction when the hyalinized tissue disappears after 30 days. The distance traveled by the maxillary canine was measured as the distance between the canine cusp tips to a line passing through the third rugae.
The statistical test compared each dental model to the baseline (first model at the day of extraction). In the laser sides, the distance between the canine and the reference plane significantly decreased along the path of the canine distally except in in 2nd week and 13th week where the canine cusp tip moved mesially.
 On the control sides, the rate of canine retraction steadily increased from the 1st to the 11th week; then it decreased in the 13th and 15th week, then increased again in the 17th week. The phenomenon of rebound of the canine cusp tip occurred in the control side once in the 15th week. This may be due to the faster movement of the canine on the laser sides, where the four phases’ cycle was repeated twice. Comparing the distance traveled, there was no statistically significant difference between the two sides, where the canine in both the laser and control sides traveled 3.8 mm. But by re-examination of the laser sides, it was found that, it passed through by two cycles of four phases mentioned by Nanda,58 while the control side passed through one. Furthermore, the fourth phase of the control sides occurred 2 weeks later than the fourth phase of the second cycle on laser side.
On the control sides, the rate of canine retraction steadily increased from the 1st to the 11th week; then it decreased in the 13th and 15th week, then increased again in the 17th week. The phenomenon of rebound of the canine cusp tip occurred in the control side once in the 15th week. This may be due to the faster movement of the canine on the laser sides, where the four phases’ cycle was repeated twice. Comparing the distance traveled, there was no statistically significant difference between the two sides, where the canine in both the laser and control sides traveled 3.8 mm. But by re-examination of the laser sides, it was found that, it passed through by two cycles of four phases mentioned by Nanda,58 while the control side passed through one. Furthermore, the fourth phase of the control sides occurred 2 weeks later than the fourth phase of the second cycle on laser side.
Our study coincided with the results of Limpanichkul, et al.,47 who found no difference in the rate of canine retraction between the laser and control groups. Similarly, Domínguez, et al.,48 found a insignificant increase in the rate of tooth movement in the laser group as did Altan, et al.,49 and Kansal, et al.50 Conversely, other researchers found that the laser significantly accelerated tooth movement (Cruz, et al.36; Youssef, et al.37; Camacho and Cujar9; Sousa, et al.41; and Doshi-Mehta and Bhad-Patil42).
 The matched measurements extracted from the model scanning and the CBCT regarding the total amount of canine movement after 4 months of retraction had a consensus of outcome. This validated the poor man’s technique (model scanning) for measuring the rate of canine movement.
The matched measurements extracted from the model scanning and the CBCT regarding the total amount of canine movement after 4 months of retraction had a consensus of outcome. This validated the poor man’s technique (model scanning) for measuring the rate of canine movement.
Molar anchorage loss was measured on the dental models as a distance from the mesiobuccal cusp tip of the first molar to the line passing through the 3rd rugae. In the laser sides, the total anchorage loss was statistically significant as the molar moved mesially by 1.009 mm. On the control sides, similar results and the molars moved mesially significantly by 1.17 mm. However, when comparing the two sides, no significant difference was found between the laser and control sides.
This confirms the ineffectiveness of the soft laser used in the current study to accelerate canine retraction and preserve molar anchorage. The significant amount of anchorage loss occurred using indirect anchorage mini-screws raises a question about its effectiveness. None of the previous studies36,37,40–43,47–50 evaluated the changes in the molar position with laser application.
In the current study, LLLT was applied using parameters (energy density), time, and application site recommended by the manufacturer.
Concerning the energy density, Goulart, et al.,28 concluded that acceleration of orthodontic movement occurred at an energy density of 5.25 J/cm2 and suggested a higher energy density, 35.0 J/cm2, may retard it. The animal study conducted by Rowan45 who used 50 J/cm2 showed no increase in the rate of tooth movement. A systematic review published by Ge, et al.,55 concluded that a relatively lower energy density (2.5, 5, and 8 J/cm2) was more effective than 20 J/cm2, and higher, although no one has yet determined the optimal dose.
Conversely, several studies using lower energy densitie showed no acceleration in tooth movement. The animal studies conducted by Rowan45 and Seifi, et al.46, both used lower energy densities of 5 J/cm2 and 6 J/cm2 respectively, yet neither showed acceleration of tooth movement. A human study done by Altan, et al.,49 used 5.3 J/cm2 and found no acceleration of tooth movement. Similarly Kansal, et al.,50 used 4.2 J/cm2, and no acceleration of tooth movement occurred. Futhermore, an animal study by Altan, et al.33 using a high energy density o laser (1717.2 J/cm2 and 477 J/cm2) concluded that low-level laser irradiation accelerates the bone remodeling process. For now we can conclude that no one has yet determined what the optimal energy density of LLLT might be.
This study applied the laser once a week 4 times, then once every 2 weeks until the end of the 4-four month trial. Preceding studies36,37,40–43,48–50 applied the laser on days 0, 3, 7, 14 of each month, while Limpanichkul, et al.,47 applied laser in the first three 3 days of each month, taking in consideration that some of these studies36,37,40–43 resulted in acceleration of tooth movement while others47–50 showed no effect. Unlike the previous studies, Gui and Qu38 applied laser therapy once per week and found acceleration of tooth movement. None of the aforementioned studies offered the rationales for their protocols. Although most of these studies used similar protocols, they achieved different results.
We applied the laser tip in the current study on the buccal mucosa above the middle third of the canine’s root. Previous studies36,40,41,43,50 applied the laser on the buccal and palatal surfaces of the canine by the buccal side and five by the palatal side, were carried out, distributed, and ordered as follows, in other studies37,42,47–49 used different application sites. With so many differing opinions regarding LLLT density, site of application, and timing of application, researchers have not come to close to reaching a consensus about a single feature, much less several variables of soft laser application.
The results of this split-mouth randomized controlled trial revealed no acceleration of orthodontic tooth movement as assessed by dental models. We recommend further studies with similar designs using different parameters and protocols to elucidate the effect of LLLT on acceleration to discover if LLLT can accelerate tooth movement with any protocol.
Conclusion
Within the limitation of this trial, LLLT application did not stimulate tooth movement with an energy density of 29.3 J/cm2 following a recommended protocol from the manufacturer table and the single buccal application site. We found no statistical nor clinical significant differences in the rate of canine retraction or molar anchorage preservation between LLLT exposure and control sides.
Acknowledgment
The authors would like to express their deepest gratitude to Dr. Larry White for his support and efforts in preparing this article for publication.[/userloggedin]
[userloggedout][/userloggedout]
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
