
Dr. Tara Emerick tailors treatment to children’s individual needs
In my orthodontic practice, I have the privilege of working with a diverse patient population, ranging from young children who need early interceptive care to adults seeking the latest in aligner technology. As an orthodontist and a mother of three, I’ve seen firsthand the unique needs of each child and how important it is to tailor our treatment approaches accordingly.
While traditional early Phase 1 tools like fixed palatal expanders and braces are time-tested, they do present notable challenges. These include discomfort, difficulties with oral hygiene, and, perhaps most significantly, limited tolerability for neurodiverse or highly sensory-sensitive children. For these kids, traditional solutions can be more than just uncomfortable — they can be impractical.
That’s why I was intrigued by Angel Aligner™ KiD, a flexible, intuitive, and comprehensive system that combines dental alignment, jaw development, and supports myofunctional habit correction all within one clear aligner platform. After successfully treating many Angel Aligner cases in both teens and adults, I wanted to explore whether Angel Aligner KiD could provide a new standard of care for my younger patients, especially those needing customized, gentle solutions.
Unlike other Phase 1 appliances I’ve used, Angel Aligner KiD was built for adaptability. It incorporates unique features like curved turbos, eruption guides, and specialized trimlines that help guide developing dentition while respecting the nuances of a child’s oral environment. Additionally, features such as A6 mandibular advancement, angelButton™, and the angelHook™ Maxillary Protraction Solution with Facemask compatibility open new possibilities for skeletal correction in a comfortable, removable format. Angel Aligner KiD’s capacity to support myofunctional correction, manage eruption, and guide skeletal development makes it an ideal choice for patients who need a different kind of care.
I’ve been using Angel Aligner for 2 years now, and I’ve seen a growing number of Phase 1 patients benefit from it. I’m consistently impressed by the intuitive iOrtho software, the impressive features, the quick turnaround times, and the excellent case setups.
Case report: neurodivergent patient with ectopic canines
My patient, “JA,” is a bright, sweet, and sensitive 10-year-old boy who had been referred to my practice for early orthodontic intervention. Due to his neurodivergence and significant oral sensory sensitivities, fixed appliances were not an option for him.
JA presented with ectopic upper canines (U3s) tracking very mesially toward the roots of the upper laterals (U2s), along with upper spacing and moderate lower crowding. I had already referred him to his pediatric dentist for the extraction of his upper primary canines.
Space consolidation and root guidance were crucial in his case to prevent impaction and preserve the lateral incisors.
Diagnosis and treatment plan
Diagnosis
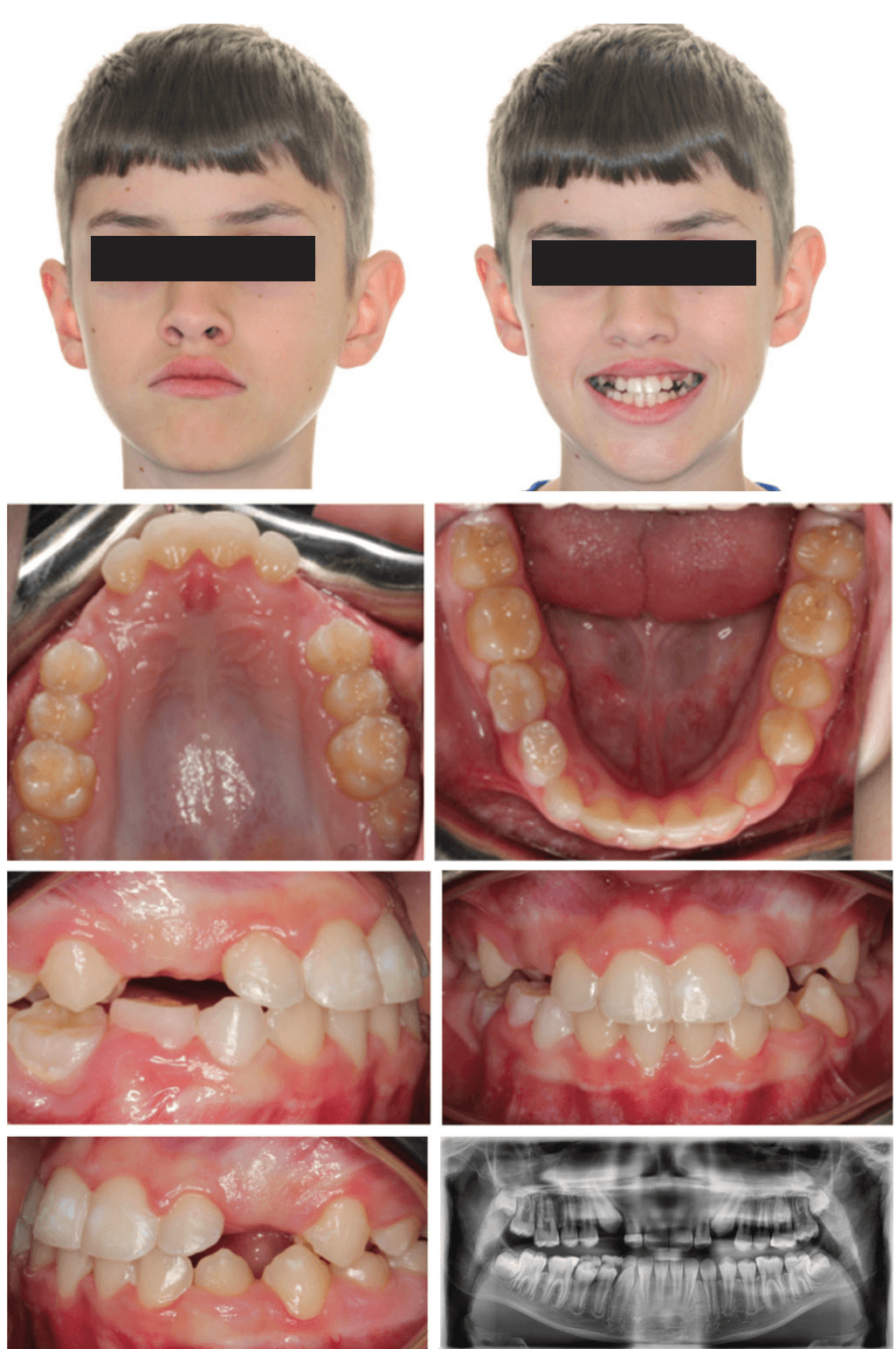
This patient presented in mixed dentition and a Class I occlusion with mild upper spacing, lower moderate crowding, and mild deep bite. The U3s were ectopic with a palatal position and a mesial path of eruption, converging onto the U2 roots, and the patient also had a tapered upper archform, an ovoid lower archform, and a posterior tongue tie (mid-tongue restriction). The upper midline was centered with the facial midline, but the lower midline was deviated 4 mm to the left of the upper (Figure 1).
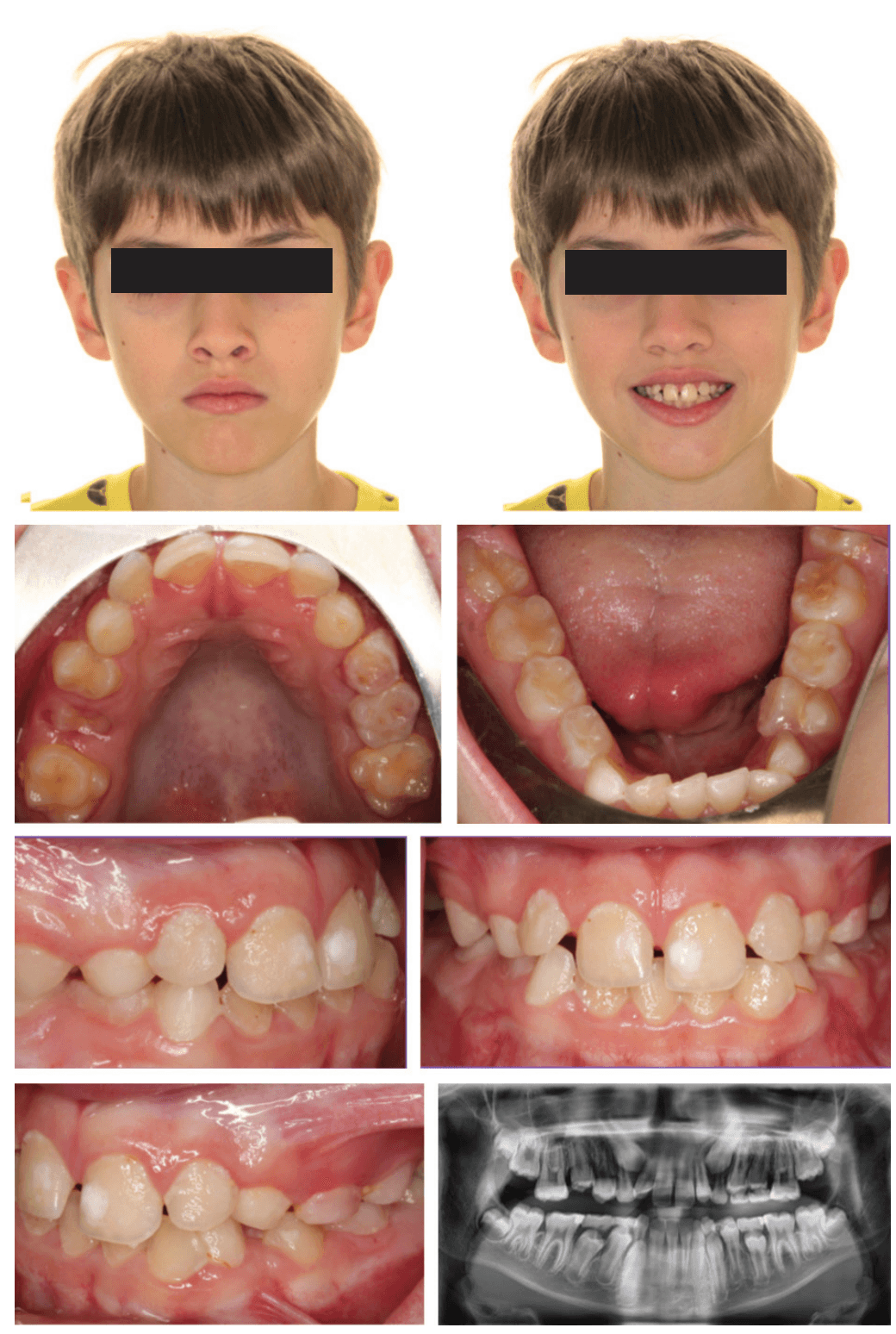
The patient exhibited hypersensitive oral behavior and is neurodivergent with motor and vocal tics. His mother reported that he would not tolerate any fixed appliances, and I was also concerned about his motor and vocal tics interfering with appliance placement. Oral hygiene was poor due to his aversion to the feeling of brushing his teeth. I was hesitant to start treatment due to the poor oral hygiene, but eager to redirect the eruption of the upper canines so we brought the patient in for a hygiene check. His hygiene had improved so we scanned for aligner treatment.
Treatment goals
The primary objectives were to expand both the upper and lower arches, consolidate anterior space, and apply a mesial root tip to the U2s to protect them from the U3 trajectory. My additional goals included aligning the arches and guiding the canines without using fixed appliances, all while respecting my patient’s comfort and cooperation threshold.
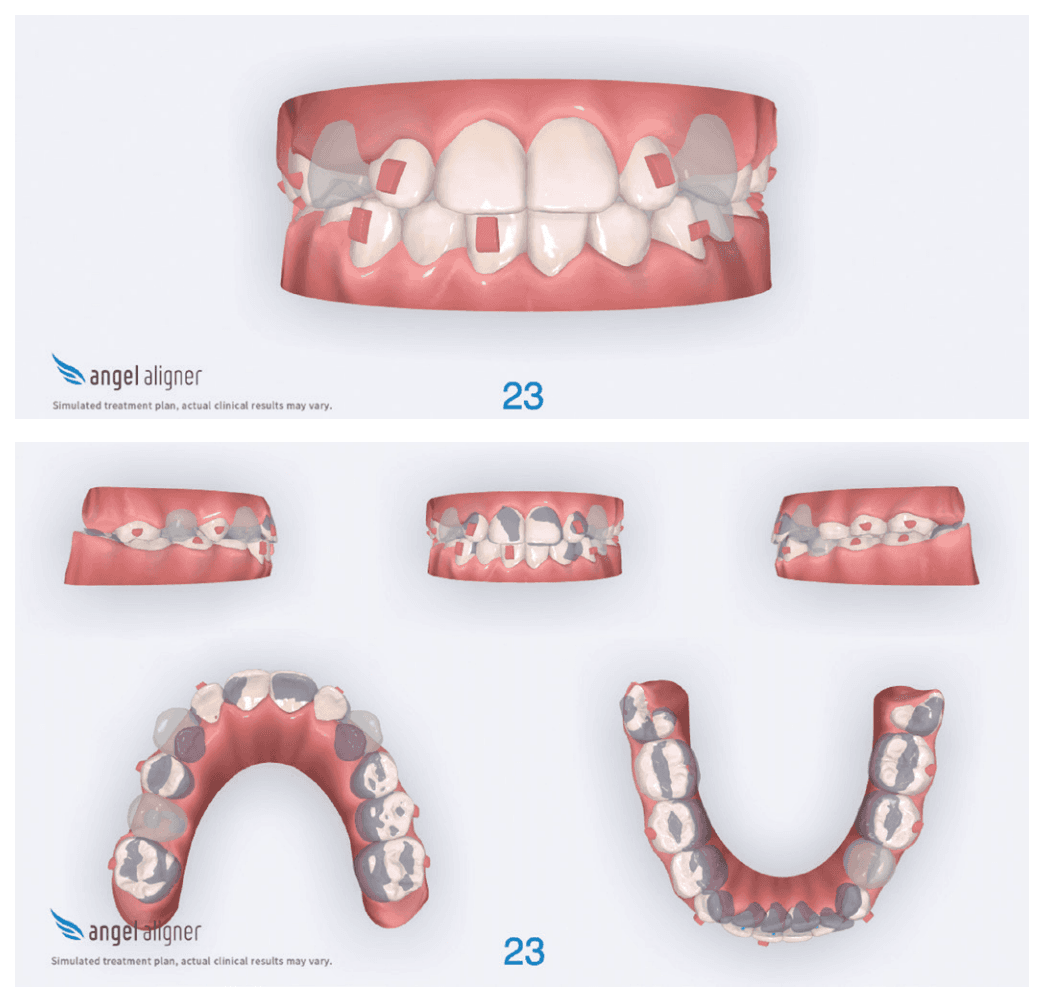
For expansion, I used my typical aligner expansion protocol of expanding the U6s first, followed by the Uc,d,e’s. For the lower, I requested uprighting of the lower posterior to coordinate with the upper arch (leveling of the Curve of Wilson). I also wanted to apply mesial root tip of the U2s to place them in a more protected position, away from the ectopic U3s. I selected Angel Aligner KiD because of its comfort, removability, and ease of hygiene for a sensory-sensitive patient.
Treatment progression
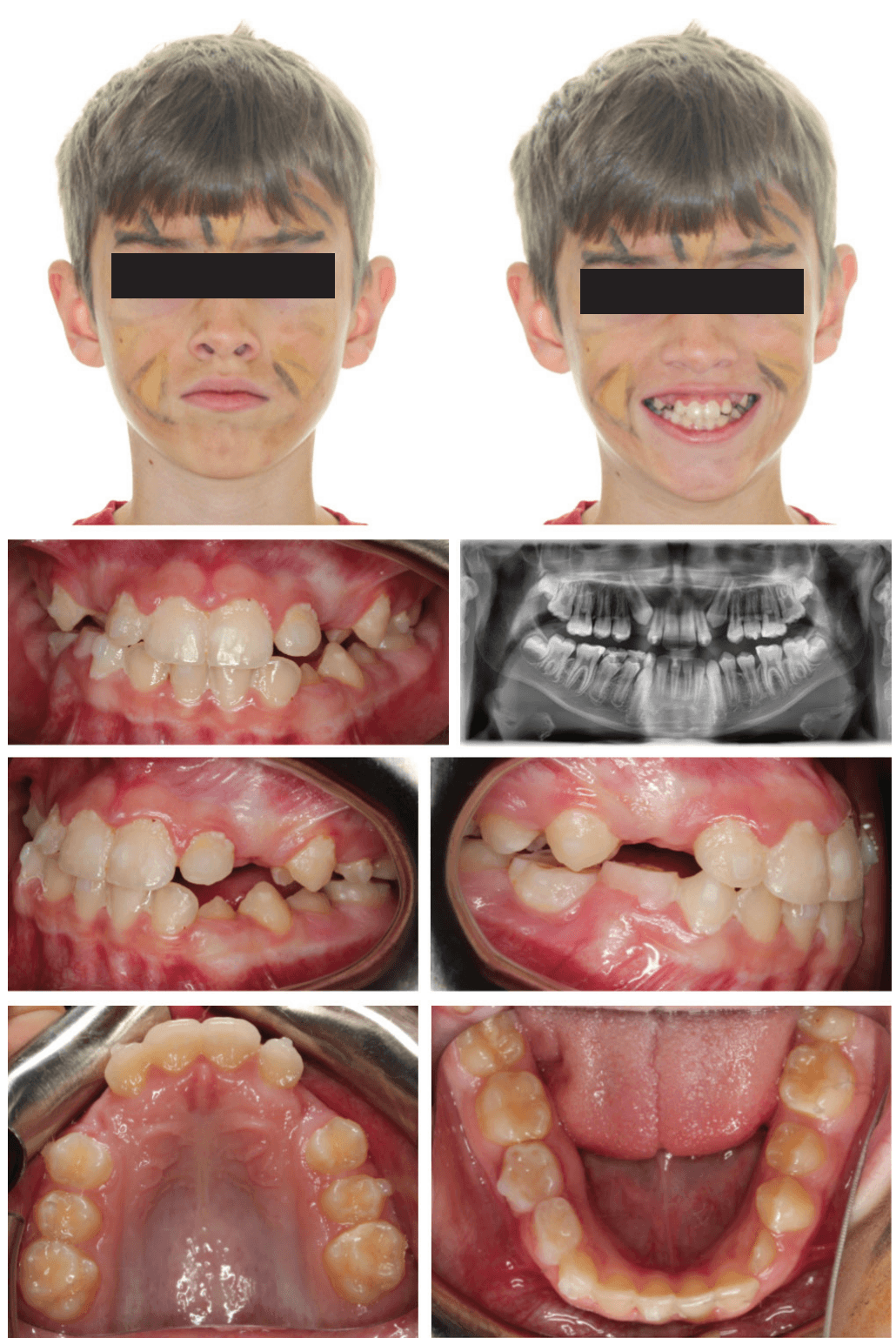
The primary phase of treatment had a total of 20 sets of aligners, and we saw the patient for three appointments (Figure 4). His compliance with aligner wear and tracking was excellent. We were pleasantly surprised by how well he adapted to both the aligners and attachments, especially given his severe oral sensitivities.
At the third appointment, we scanned for refinement to finish closing the U2-2 spacing and exaggerate the U2 mesial root tip. This refinement phase had 16 sets of aligners, and the patient had an additional three appointments, including the debond appointment. Overall, the patient’s treatment spanned 10 months and included six appointments.
Clinical outcome
After 10 months, I’m pleased to report on the successful completion of Phase 1 treatment for the patient. His arches have been expanded and aligned, and the space has been appropriately consolidated.
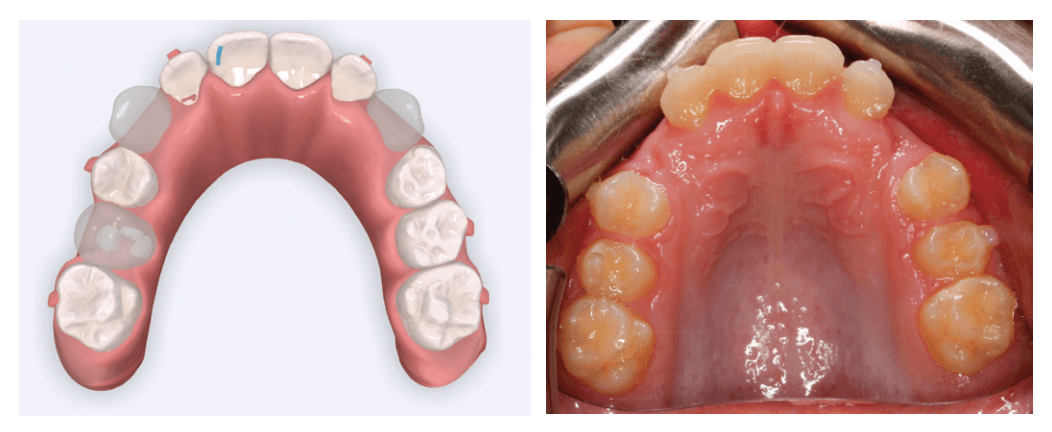
We successfully tipped the U2 roots mesially, which created a natural shield for the erupting U3s. As a result, the canines are now erupting naturally into a favorable path, avoiding root damage (Figure 5).
lower arches expanded and aligned, anterior spacing consolidated, midlines centered, and U2 mesial root tip exaggerated
The patient and his mother are thrilled with the outcome, which exceeded their expectations and was achieved without emotional or physical distress. He now enjoys coming back to see us for his retainer checks because he had such a positive treatment experience.
Key learnings
This case truly highlighted the power of personalized orthodontics for me. Using Angel Aligner KiD, I was able to:
- Safely treat a challenging Phase 1 case.
- Avoid canine impaction and the need for future surgical exposure.
- Reduce any stress or trauma often associated with early orthodontic care in neurodivergent children.
- Maintain precise control over root movement and space management without relying on fixed appliances.
The capability of Angel Aligner KiD to integrate alignment, expansion, and functional correction into one streamlined system makes it an indispensable tool in my Phase 1 toolbox. It has also enabled me to provide comprehensive care in a compassionate and minimally invasive manner.
Conclusion
Every child deserves a smile journey that respects their individuality. Angel Aligner KiD delivers on that promise with advanced engineering, smart software, and adaptable features that redefine what’s possible in early interceptive treatment.
For my patient, it meant a future free of canine impaction and surgery. For me, it was a reminder that innovation is about more than outcomes — it’s about compassion, access, and adaptability.
 Tara Emerick, DDS, MS, is a board-certified orthodontist and the owner of Emerick Orthodontics in Carmel, Indiana. She completed her undergraduate and master’s degrees at The University of Illinois at Urbana-Champaign. Dr. Emerick earned her Doctor of Dental Surgery degree from Indiana University, followed by a certificate in Orthodontics and a master’s in Oral Sciences from The University of Illinois at Chicago. At her pink, boutique-style start-up practice in Carmel, Dr. Emerick is passionate about using innovation to deliver exceptional and individualized care. Dr. Emerick is a proud mother of three and an advocate for compassionate, tech-forward orthodontics.
Tara Emerick, DDS, MS, is a board-certified orthodontist and the owner of Emerick Orthodontics in Carmel, Indiana. She completed her undergraduate and master’s degrees at The University of Illinois at Urbana-Champaign. Dr. Emerick earned her Doctor of Dental Surgery degree from Indiana University, followed by a certificate in Orthodontics and a master’s in Oral Sciences from The University of Illinois at Chicago. At her pink, boutique-style start-up practice in Carmel, Dr. Emerick is passionate about using innovation to deliver exceptional and individualized care. Dr. Emerick is a proud mother of three and an advocate for compassionate, tech-forward orthodontics.
Disclosure: Dr. Tara Emerick is a paid consultant of USA Angelalign Technology Corp.
- Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 1988 Nov;10(4):283-95. doi: 10.1093/ejo/10.4.283.
- Angel Aligner KiD Patient Brochure. Angel Aligner. angelaligner.com.
- Alvarado, P. “Angel Aligner KiD Webinar.” Angel Aligner. https://education.angelaligner.com/event/angel-aligner-kid-aligning-young-smiles-with-confidence/.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
