Scott Huge, Paul Gange, and Dr. Michael Mayhew discuss the evolution and clinical benefits of indirect bonding
 Orthodontic indirect bonding delivers undeniable clinical advantages. Many practices recognize efficiency gains through office delegation, improved bracket placement, and chair time reductions. Despite these benefits, fewer than 20% of orthodontic specialists use the technique. However, recent numbers indicate an upward trend of new practices implementing indirect bonding (IDB), and many industry experts believe this trend will continue due to recent technological advancements. This article presents recent innovations and perspectives from three leading indirect bonding experts. Their knowledge represents decades of laboratory experience, adhesive development, and the clinical implementation of indirect bonding.
Orthodontic indirect bonding delivers undeniable clinical advantages. Many practices recognize efficiency gains through office delegation, improved bracket placement, and chair time reductions. Despite these benefits, fewer than 20% of orthodontic specialists use the technique. However, recent numbers indicate an upward trend of new practices implementing indirect bonding (IDB), and many industry experts believe this trend will continue due to recent technological advancements. This article presents recent innovations and perspectives from three leading indirect bonding experts. Their knowledge represents decades of laboratory experience, adhesive development, and the clinical implementation of indirect bonding.
Scott Huge founded Specialty Appliances orthodontic laboratory in 1981 and quickly became a leader of IDB development and production.
When introducing an updated product or service, it is interesting to review the history. Despite over 40 years of reported advantages with indirect bonding, the technique has never gained more than an estimated 15% market share among clinicians. Although surveyed IDB users say they cannot imagine practicing without the established benefits, we also know that there are many orthodontists who have tried IDB and abandoned the technique. Their typical reason generally falls into one of three categories — bond failure, inconsistent bracket positioning, and practice integration difficulties. Why does it work so well for some offices, but not for others? Let’s address some indirect bonding issues and highlight the innovations that provide solutions.
We obviously have a vested interest in promoting our IDB service, but there is another link that needs to be considered. Previously, there has been only a handful of commercial labs offering a consistently high-quality IDB service, so practices had to simultaneously conquer both the clinical and laboratory sides of the process. Many offices simply lack the necessary laboratory systems experience to produce IDB trays that deliver consistent clinical results. Unlike an invisible retainer, which can be made predictably by the “in-office” lab with minimal training, indirect bonding requires experience and fine-tuned laboratory processes. Even if a practice wants to manufacture IDB trays in-house, we recommend sending the first 15-20 cases to an experienced lab like Specialty Appliances. Once the staff has mastered chairside delivery of the trays and experienced the benefits, they can tackle tray production. Inconsistent trays resulting from inexperience will create a bad IDB experience in your practice.
Regardless of the source of fabrication, brackets must stay on the teeth. The first input to successful clinical delivery is accurate models. We constantly stress this issue with all appliance fabrication. However, accuracy is absolutely critical with indirect bonding. The practice must commit to taking high-quality impressions and pouring the models immediately in hard stone. For guaranteed success with IDB, there are simply no shortcuts allowed at this stage. The most exciting development in model accuracy is the widespread adoption of intraoral scanners. Presently, over 50% of our incoming IDB cases are submitted from an intraoral scanner. The improved accuracy of scanners is evident with our digital customers reporting minimal, if any, bond failures due to inaccuracies. In other words, the IDB trays fit better than ever when using scanners.
 Assuming we have accurate models, we turn to the bracket bases adhering to the teeth. At Specialty, all IDB cases (labial and lingual) are processed with custom adhesive bases as the interface between the bracket and tooth surfaces. This has been our standard for many years and is by far the most predictable method. For our custom base production method, we use thermal-set adhesive. This allows our senior technicians ample time to check all cases and make minor adjustments to bracket positions prior to tray fabrication. Custom bases require higher quality models due to the precision fit of the bases to the teeth, but they are extremely advantageous. Only a small amount of flowable adhesive is needed in the clinical delivery, minimizing flash around the brackets.
Assuming we have accurate models, we turn to the bracket bases adhering to the teeth. At Specialty, all IDB cases (labial and lingual) are processed with custom adhesive bases as the interface between the bracket and tooth surfaces. This has been our standard for many years and is by far the most predictable method. For our custom base production method, we use thermal-set adhesive. This allows our senior technicians ample time to check all cases and make minor adjustments to bracket positions prior to tray fabrication. Custom bases require higher quality models due to the precision fit of the bases to the teeth, but they are extremely advantageous. Only a small amount of flowable adhesive is needed in the clinical delivery, minimizing flash around the brackets.
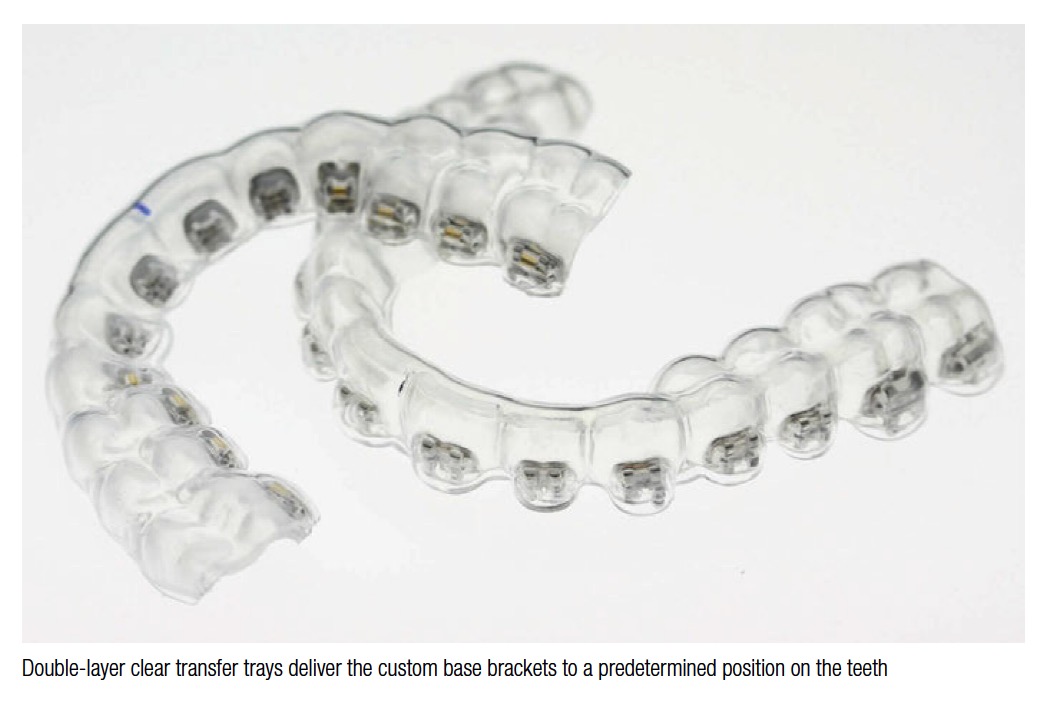
Once the brackets are set, we process the transfer trays using the traditional
“2 tray” technique, consisting of a softer inner tray coupled with a harder outer material. All trays are made from clear pressure-formed blanks using a BioStar® (Great Lakes Orthodontics), another tool proven to deliver consistent results. We prepare the brackets for tray processing by blocking out the significant undercuts in the bracket architecture to prevent the soft inner tray from forming too tightly around the brackets. We are aware of practices using a clear silicone to make transfer trays. In our experience, the silicone does work. However, we believe the clear dual tray system to be an easier technique in production on a high-volume basis.
For practices wanting to completely outsource their IDB fabrication, Specialty can accommodate even the most demanding offices. This includes our expertise in bracket placement and tray fabrication, managing digital files, printing models, and ensuring on-time deliveries. At Specialty, a senior technician oversees and checks brackets on 100% of cases. In addition, we have the ability to assign a specific senior technician to an individual practice to guarantee placement nuances of that doctor are followed on all cases.
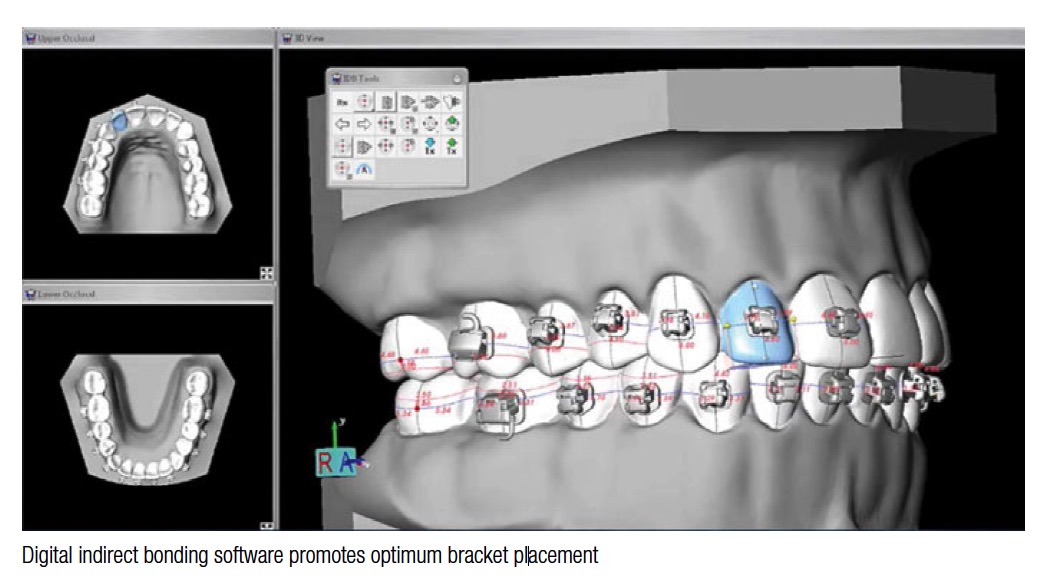
Specialty’s most recent IDB development uses advanced CAD software to meet the demand for high-precision bracket positioning. First, we produce a digital setup of the finished case in ideal occlusion. Brackets are then digitally placed on the ideal setup, using a full-size straight wire to ensure slot alignment. Doctors then have the ability to review, manipulate, and approve the bracket position. The software replicates the exact 3D bracket location from the ideal model to the malocclusion. Specialty’s proprietary process accurately transfers the digital bracket placement to the physical model. Transfer trays are then constructed and shipped to the orthodontic practice.
 Paul Gange founded Reliance Orthodontics in 1981 and is widely recognized as a leading expert in orthodontic bonding materials.
Paul Gange founded Reliance Orthodontics in 1981 and is widely recognized as a leading expert in orthodontic bonding materials.
The first custom base indirect bonded technique utilized a two-part chemical cure bonding resin (Concise™, 3M Unitek) to transfer the brackets from the tray onto the enamel. With regards to clinical durability, the shear bond strength with this method was determined by how well the custom composite pad on the bracket base fit each specific tooth. Any voids between the custom pad and dental anatomy, due to inaccuracies in the models or trays, would result in failure at some point. In addition, original IDB systems did not have adhesion boosters to promote an improved bond to enamel, porcelain, metal crowns, or the composite custom pad. All these factors, coupled with the challenges in fabricating accurate transfer trays, produced in-consistent results, and subsequently, clinicians abandoned the technique.
Today, we have universal bonding resins such as Enhance™, Assure® and Ortho Solo that promote a strong bond to wet or dry enamel. Additionally, Enhance and Assure will increase the chemical bond to the composite custom base on the bracket. These universal resins are applied to the etched enamel and custom base before the application of the transfer adhesive. From clinical feedback we’ve received, it is estimated that at least 75% of practices using indirect bonding are adding some type of adhesion “booster” to their clinical protocol.
 One proven method of transferring the brackets into the mouth uses a two-part chemical cure no-mix resin such as Custom IQ Maximum Cure®. Once the indirect trays are seated in the mouth, this adhesive polymerizes much quicker and produces a higher strength than previous chemical cure materials.
One proven method of transferring the brackets into the mouth uses a two-part chemical cure no-mix resin such as Custom IQ Maximum Cure®. Once the indirect trays are seated in the mouth, this adhesive polymerizes much quicker and produces a higher strength than previous chemical cure materials.
The second and most popular method uses a single paste, light cure, flowable composite such as Flow Tain (Reliance Orthodontics) or Transbond™ Supreme LV (3M Unitek). The advantages of light-cured adhesives are a longer working time, coupled with the ability to fill any micro-gaps between the custom pads and tooth surfaces. In the event there is not a perfect flush fit between the custom pad and tooth when the bracket is transferred in the mouth, the 65% filled paste will occupy that void and maintain bond strength, unlike the two-part chemical cure liquid resin. Due to the reduced amount of filler and application of flowable paste to the gingival half of the custom pad only, the polymerized peripheral flash is easily removed. Remember, when light curing through a clear tray, cure 10 seconds per bracket through the tray from the incisal edge. Remove the trays, and cure an additional 3 seconds each (from two angles) regardless of light intensity.
 In summary, modern indirect bonding techniques are much more dependable. Now, we also have universal bonding resins used to prep tooth surfaces and the custom pads, increasing adhesion at the tooth and bracket base. The fast-reacting chemical cure resins and light-cure flowable composites are stronger than their predecessors, making the shear bond strength of indirectly transferred brackets as strong and successful as direct bonding.
In summary, modern indirect bonding techniques are much more dependable. Now, we also have universal bonding resins used to prep tooth surfaces and the custom pads, increasing adhesion at the tooth and bracket base. The fast-reacting chemical cure resins and light-cure flowable composites are stronger than their predecessors, making the shear bond strength of indirectly transferred brackets as strong and successful as direct bonding.
Michael Mayhew, DDS, MS, PA, is a dual-trained Pediatric Dentist and Orthodontist practicing in Boone, North Carolina. Dr. Mayhew has utilized indirect bonding and played a key role in the development of digital bracket placement software over the past 12 years.
 Utilization of indirect bonding offers multiple benefits for our practice. The most realized advantages appear in practice management, clinical, and ergonomic efficiencies. IDB enables us to delegate the majority of chairside bonding time to our clinical staff, freeing the orthodontist to perform other doctor-required procedures, like new patient examinations. Recent laboratory innovations use state-of-the-art bracket placement software, allowing us to review a virtual treatment and even alter the positioning of teeth and brackets. Once approved, the lab sends us indirect trays ready for patient bonding.
Utilization of indirect bonding offers multiple benefits for our practice. The most realized advantages appear in practice management, clinical, and ergonomic efficiencies. IDB enables us to delegate the majority of chairside bonding time to our clinical staff, freeing the orthodontist to perform other doctor-required procedures, like new patient examinations. Recent laboratory innovations use state-of-the-art bracket placement software, allowing us to review a virtual treatment and even alter the positioning of teeth and brackets. Once approved, the lab sends us indirect trays ready for patient bonding.
 The most significant benefit of computer-assisted bracket placement is best-realized chairside. Clinical advantages are gained as initial alignment, archwire progression, and anticipated occlusal schemes develop readily due to optimal bracket positioning. Ergonomic efficiencies are realized through fewer repositions and detail bends, easier wire changes, and better clinical management of the patient. These benefits evoke confidence in doctors and staff as well as our patients and parents. Also, manipulating the digital models to demonstrate treatment goals for patients and parents is seen as “high tech.” We find that it improves patient education, case acceptance, and orthodontic practice marketing within our offices.
The most significant benefit of computer-assisted bracket placement is best-realized chairside. Clinical advantages are gained as initial alignment, archwire progression, and anticipated occlusal schemes develop readily due to optimal bracket positioning. Ergonomic efficiencies are realized through fewer repositions and detail bends, easier wire changes, and better clinical management of the patient. These benefits evoke confidence in doctors and staff as well as our patients and parents. Also, manipulating the digital models to demonstrate treatment goals for patients and parents is seen as “high tech.” We find that it improves patient education, case acceptance, and orthodontic practice marketing within our offices.
Indirect bonding provides reliable bond strength in our practice. Advancement in bonding techniques and materials with proper isolation eliminate past concerns. Our delivery system is an inner soft and outer hard clear tray with custom base brackets. After applying a bond enhancer to both pad and enamel surfaces, a small amount of flowable light-cured adhesive is placed on the back of each bracket pad. The flowable adhesive fills any small imperfections in the custom base, and minimal flash is created. We experience bond strength equal to direct bonding with this bracket delivery system.
Training your clinical staff to manage chairside IDB delivery presents a moderate learning curve, but our team has thrived with the additional responsibility. Each clinical staff member follows our precise IDB bonding protocol. It is important to emphasize extra detail on proper isolation in tooth preparation. An experienced clinical staff member can deliver bonding trays without an assistant, maximizing efficiency in the practice.
Indirect bonding can contribute many efficiency gains in the orthodontic practice. Increased staff utilization, decreased doctor chair time at bonding, increased doctor time availability, decreased repositioning and detailing requirements, and shorter treatment times with fewer appointments are noted advantages of this procedure. IDB systems are more reliable with today’s specialized bond enhancers, adhesives, and consistent delivery systems. The evolution of digital technology in orthodontics has optimized bracket placement and promises an exciting future for indirect bonding in orthodontics.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
