Drs. Rohit C.L. Sachdeva, Steven Moravec, Takao Kubota, and Jun Uechi continue their exploration of management of skeletal deformities using suresmile® technology
Introduction
Suresmile® technology is a total patient care management system that enables the orthodontist to provide personalized care to patients with a wide variety of malocclusions.1-16 These include patients with skeletal deformities requiring orthognathic surgery. In a previous article,16 three approaches to planning surgical care for a patient using suresmile were described. Each approach is distinguished by the type of the image taken for planning purposes. These are “Fusion” (CAT scan), “Direct” (CBCT), or OraScan (Sachdeva).
Also, in a previous article,16 planning care with the “Fusion” approach was discussed. In this article, aided with an example of a patient history, the “Direct” method is described for planning orthognathic surgery and designing custom surgical archwires with the goal of providing effective and efficient care for
a patient.
Patient C.H.
Patient C.H., a 20-year-old female Caucasian patient, presented with a chief complaint of “I cannot bite into an apple, and I have a protruding lower jaw.” She had a previous history of orthodontic treatment. Her oral hygiene was unremarkable, and she had all teeth present with the third molars unerupted. She demonstrated a skeletal Class 3 pattern with a maxillary deficiency and mandibular excess. No functional shifts were recorded. Her initial records with a cephalometric analysis are shown in Figure 1. Also, note that the Virtual Diagnostic Model (VDM) in this case is a suresmile post-processed CBCT scan. Currently, four systems are certified for use with suresmile: i-CAT™ Next Generation, i-CAT™, i-CAT™ FLX (Imaging Sciences International, Hatfield, Pennsylvania), and Kodak® CS 9300 (Carestream Dental LLC, Atlanta, Georgia). The images taken by these CBCT scanners are processed for surface data from the CBCT scan (Figure 1B).

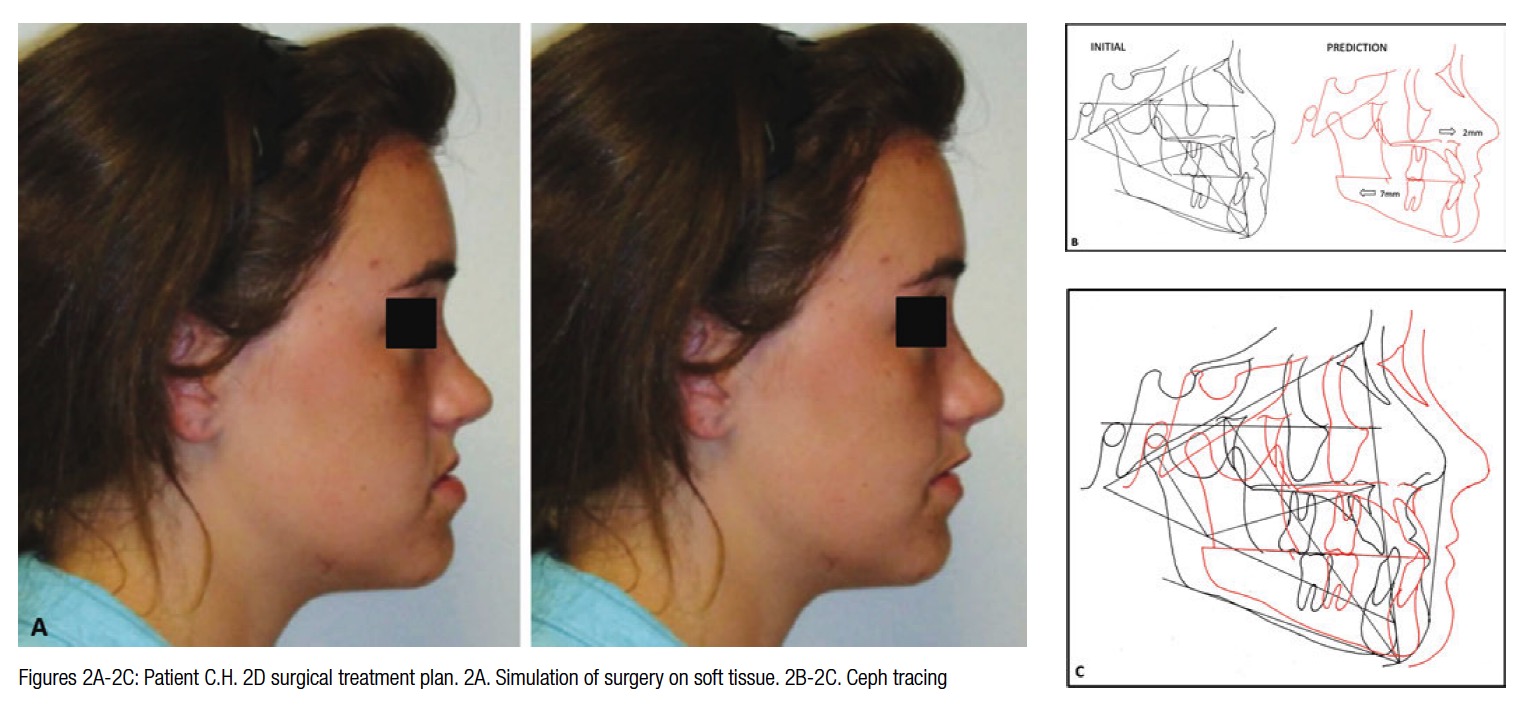
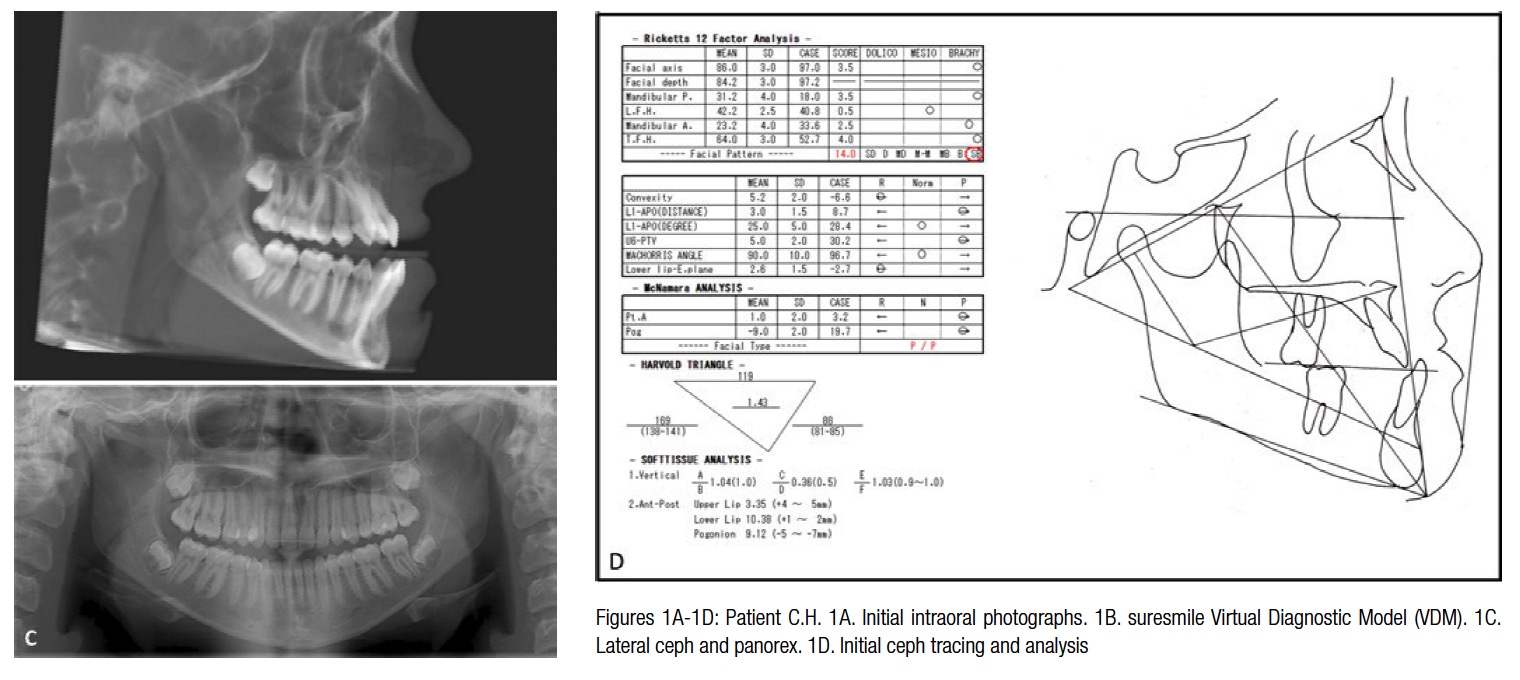

Since any tooth contact prevents the capture of the entire crown surface and leads to a distorted image during post-processing, the CBCT image is taken with mouth open with the patient requested to bite down on a piece of wax as the image is captured. A sagittal perspective of the volumetric image can be reconstructed to render the cephalometric view. Also, for the purposes of a cephalometric analysis, the tracing is corrected for the open-mouth position by rotating the mandible around the condylar head to the point of first tooth contact in order to establish a better representation of the patient’s mandibular spatial relationship with respect to the rest of the craniofacial complex. The plan for patient C.H. was soft-tissue driven. Soft tissue changes were projected in response to maxillo-mandibular movements (Figure 2A). To achieve the best esthetic results, mandibular setback and maxillary advancement with a clockwise rotation was planned in 2D using WinCeph® Ver 9.0 software from Rise Inc. (www.risecorp.co.jp) (Figure 2).
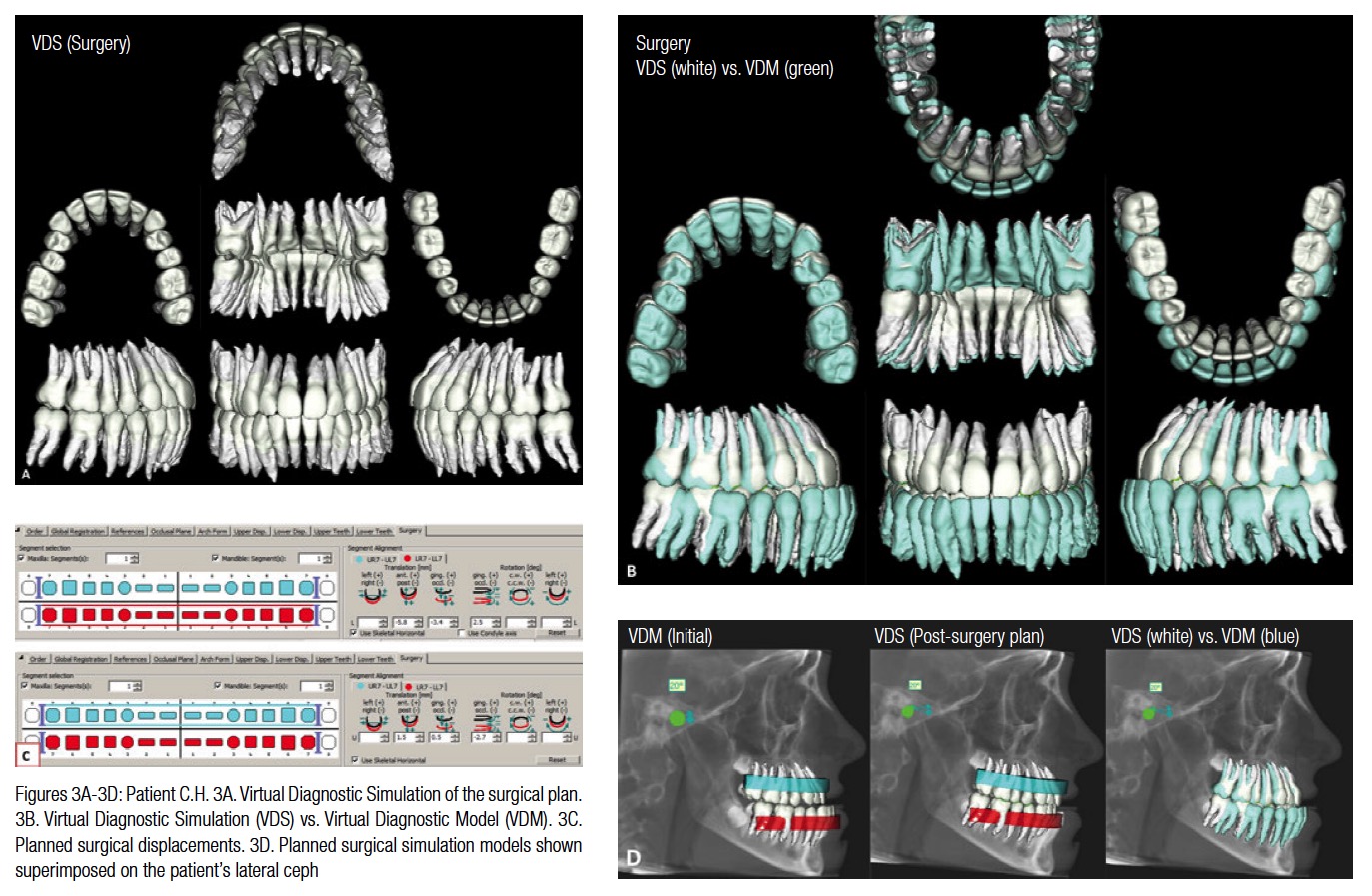
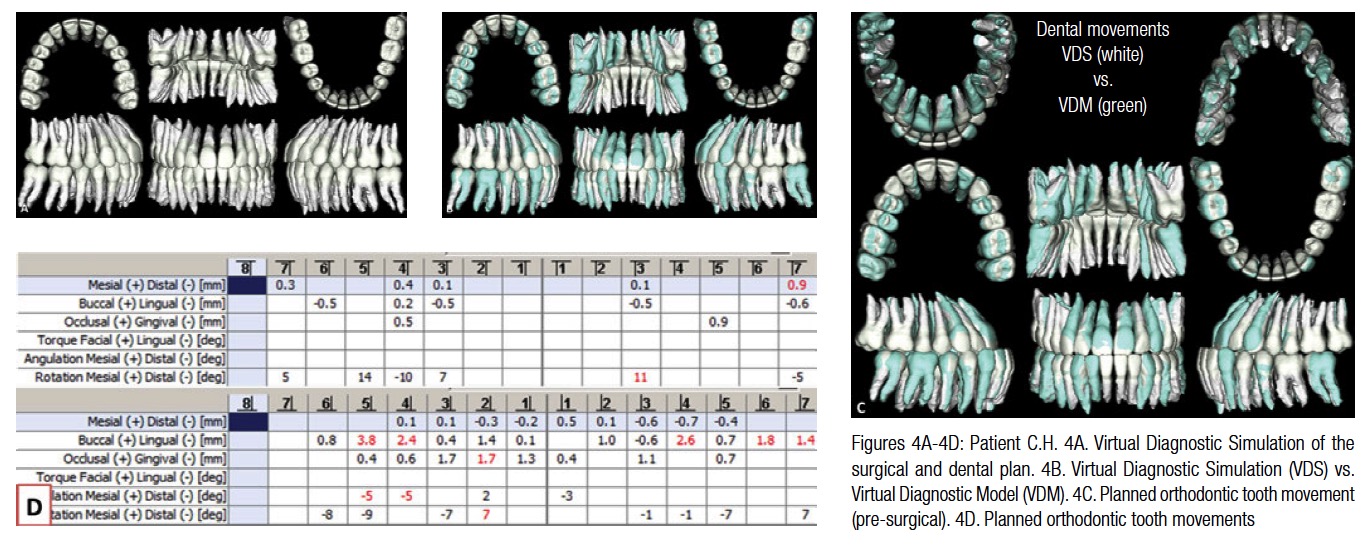
The displacement coordinates from the 2D simulation were used as a guideline to plan the skeletal movements in 3D with the Virtual Diagnostic Model (VDM) to create the Virtual Diagnostic Simulation (VDS). The VDS in Figure 3 shows the planned skeletal movements, and Figure 4 shows the planned pre-surgical and dental movements
Treatment was initiated by bonding the patients with Strite Industries Speed Rhomboid (www.speedsystem.com) brackets with 0.022″ slot width. The initial archwires used in both the upper and lower arches were .016x.022 CuNiTi AF 35°C.
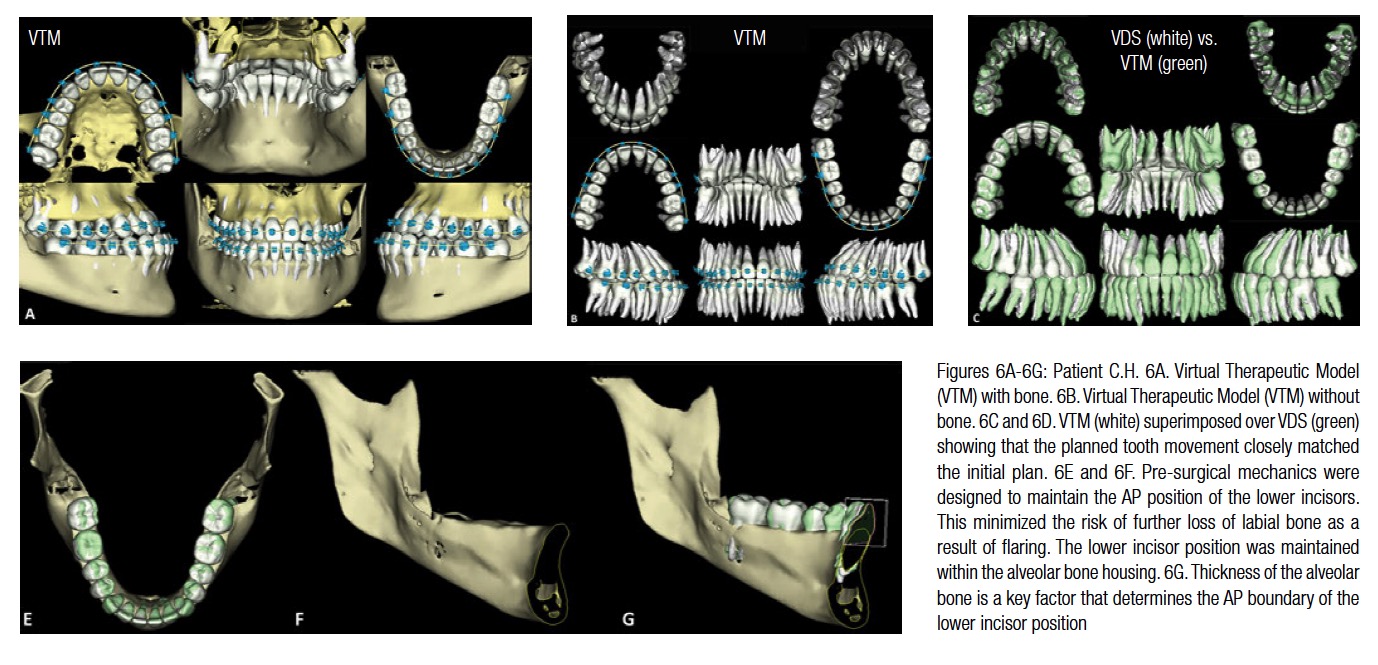
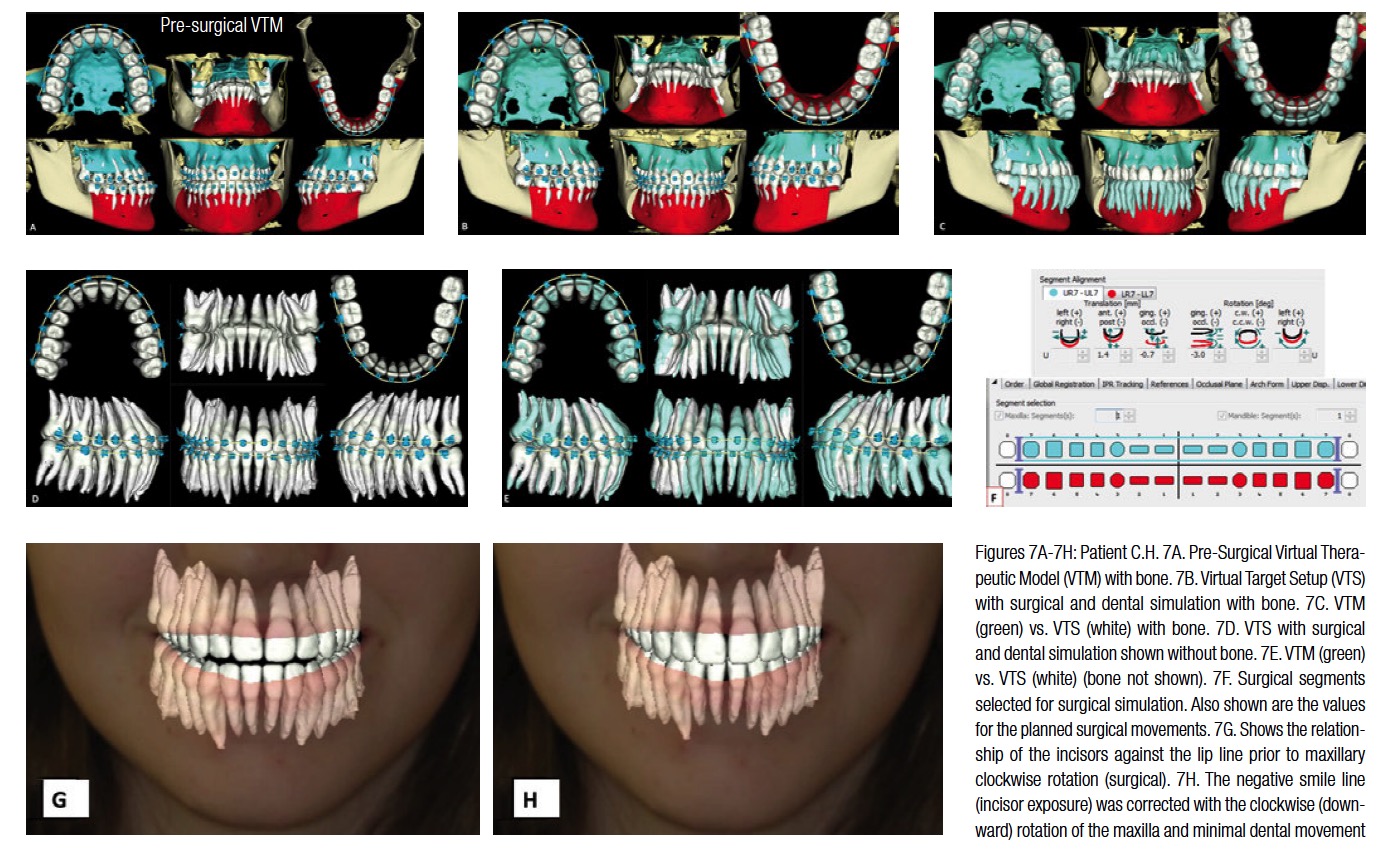
The patient was seen 10 weeks later, and a therapeutic CBCT scan was taken. The intraoral photos and X-rays at the time of therapeutic scan are shown in Figure 5. The superimposition of the VDS to VTM (Figure 6) shows that most of the pre-surgical treatment objectives were achieved. Note that the lower incisors demonstrate minimal bone on the labial aspect. The pre-surgical mechanics were designed to maintain the AP position of the lower incisors to minimize any further loss of labial bone as a result of flaring. The lower incisor position was maintained within the alveolar bone housing (Figures 6E and 6F). As can be seen in Figure 6G, the labiolingual thickness of the alveolar bone is the limiting factor in determining the AP position of the lower incisors. Planning with the surgical Virtual Therapeutic Model (VTM) was initiated by selecting the osteotomy segments. These are shown in Figures 7A and 7F. The surgical Virtual Target Setup (VTS) with and without bone and the accompanying tooth movement are shown in Figures 7B-7F. The smile line was planned by employing the superimposed image of the 3D maxillary segment with the facial image. (The suresmile digital lab as one of its services superimposes the 3D post-processed CBCT image to the 2D extraoral frontal smile image.) The maxillary segment was rotated clockwise to establish a better incisor-stomion relationship. (This can be seen in Figures 7G and 7H).
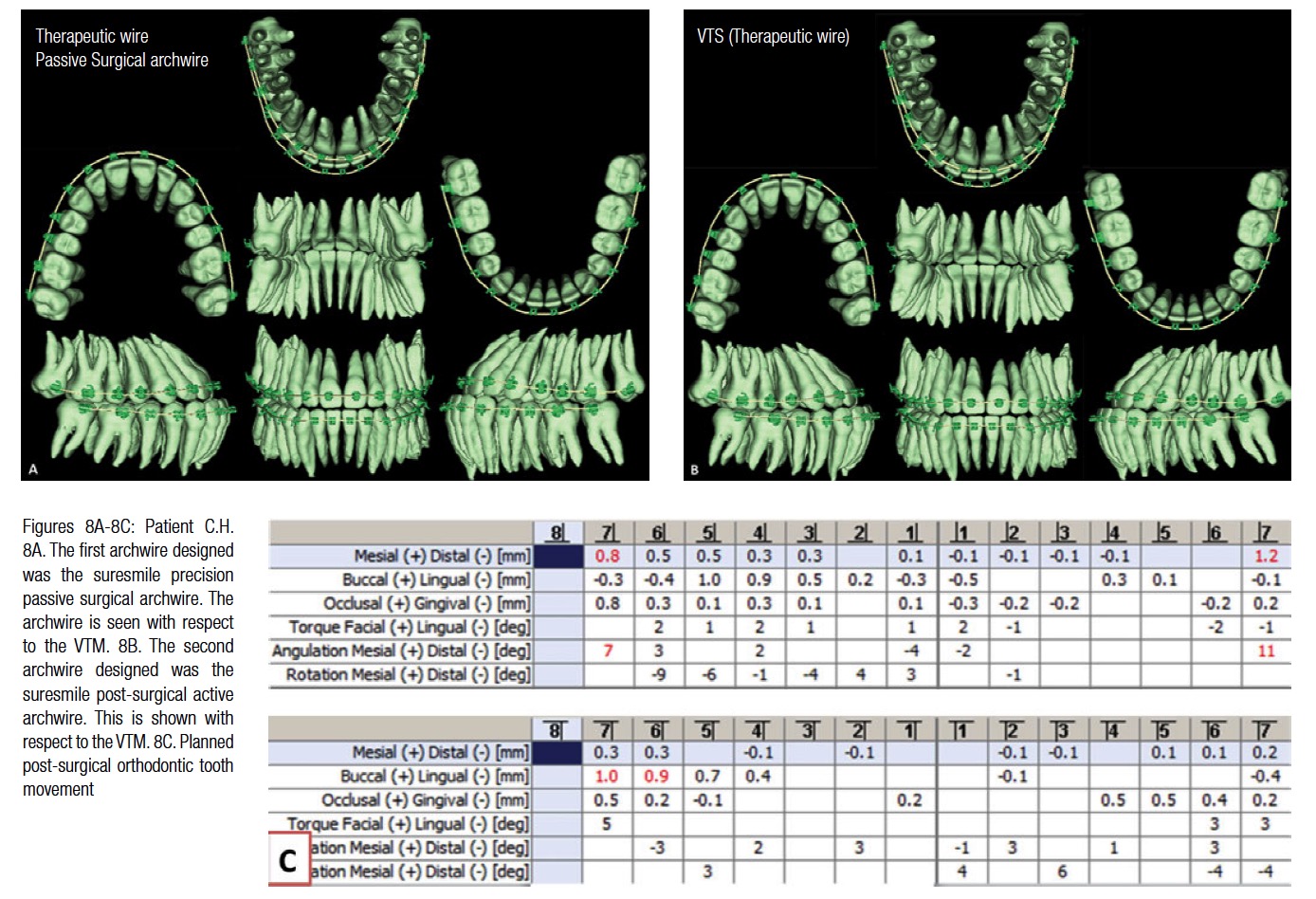
The Virtual Target Setup (VTS) was staged to design the suresmile archwires. The first setup was used to design the suresmile precision passive surgical archwire (.017x.025 CuNiTi) and the second for the post-surgical suresmile precision active archwire (.017x.025 CuNiTi AF 35°C) (Figure 8). The pre-surgical archwire was inserted 6 weeks post-therapeutic CBCT scan. Because of schedule conflicts, the patient’s surgery was performed 8-weeks post suresmile precision passive archwire insertion. Patient C.H. was seen 6 weeks post-surgery and the active post-surgical archwire inserted (Figure 9).
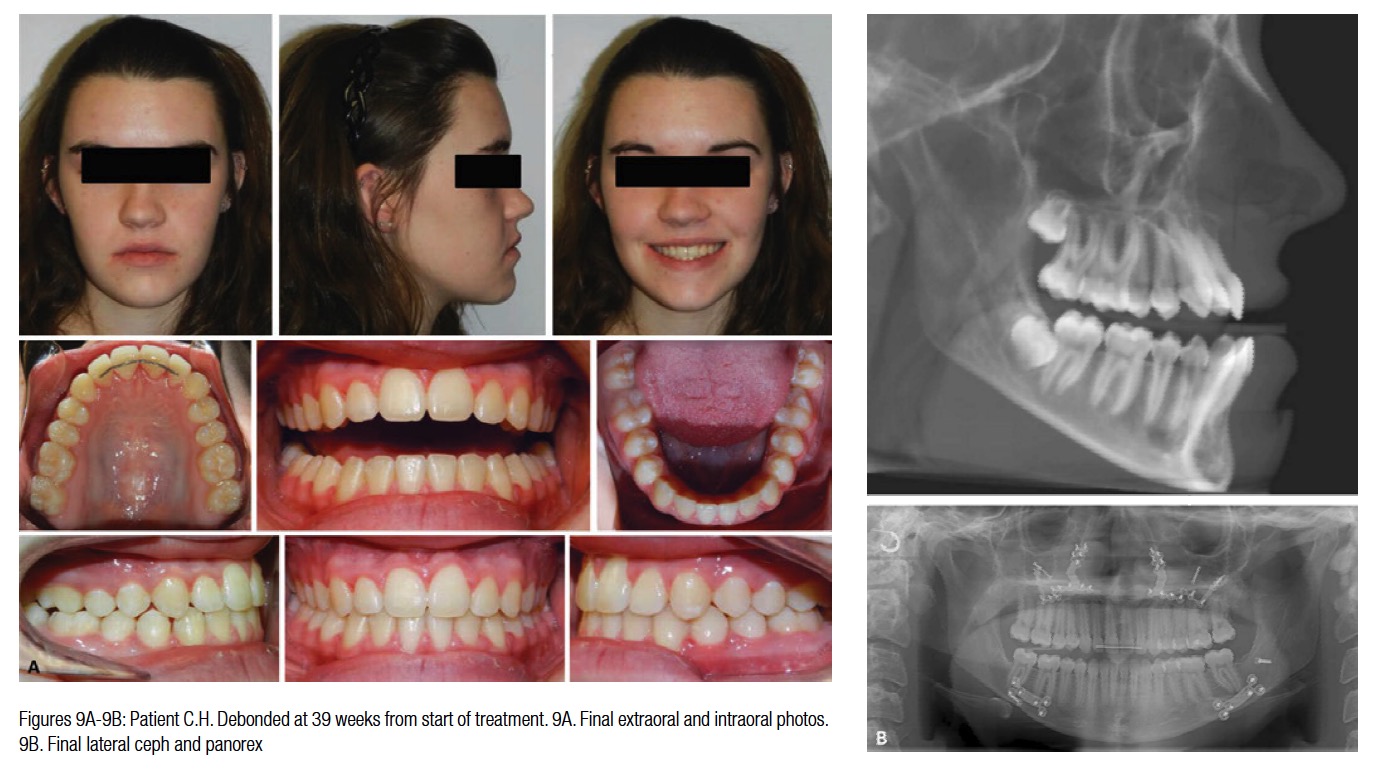
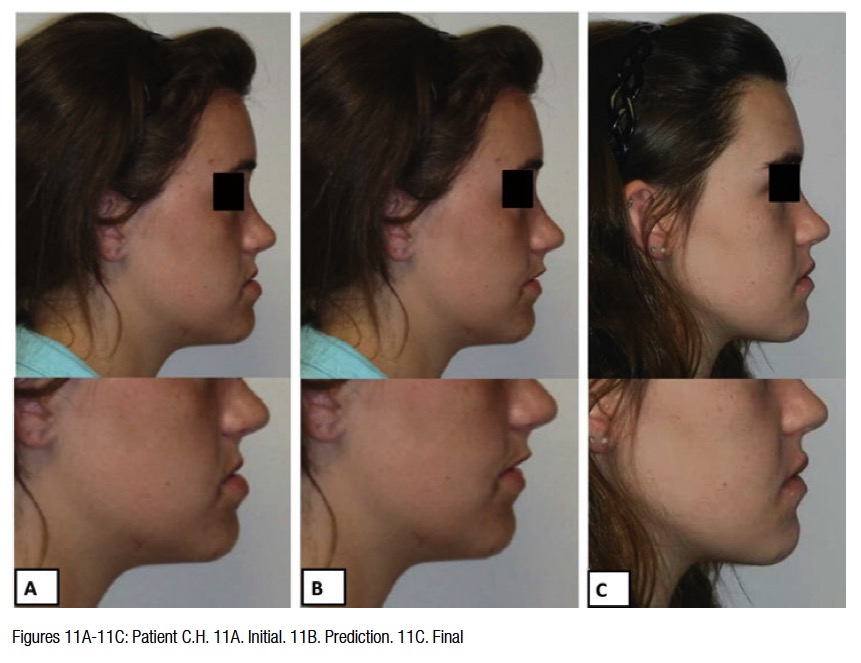
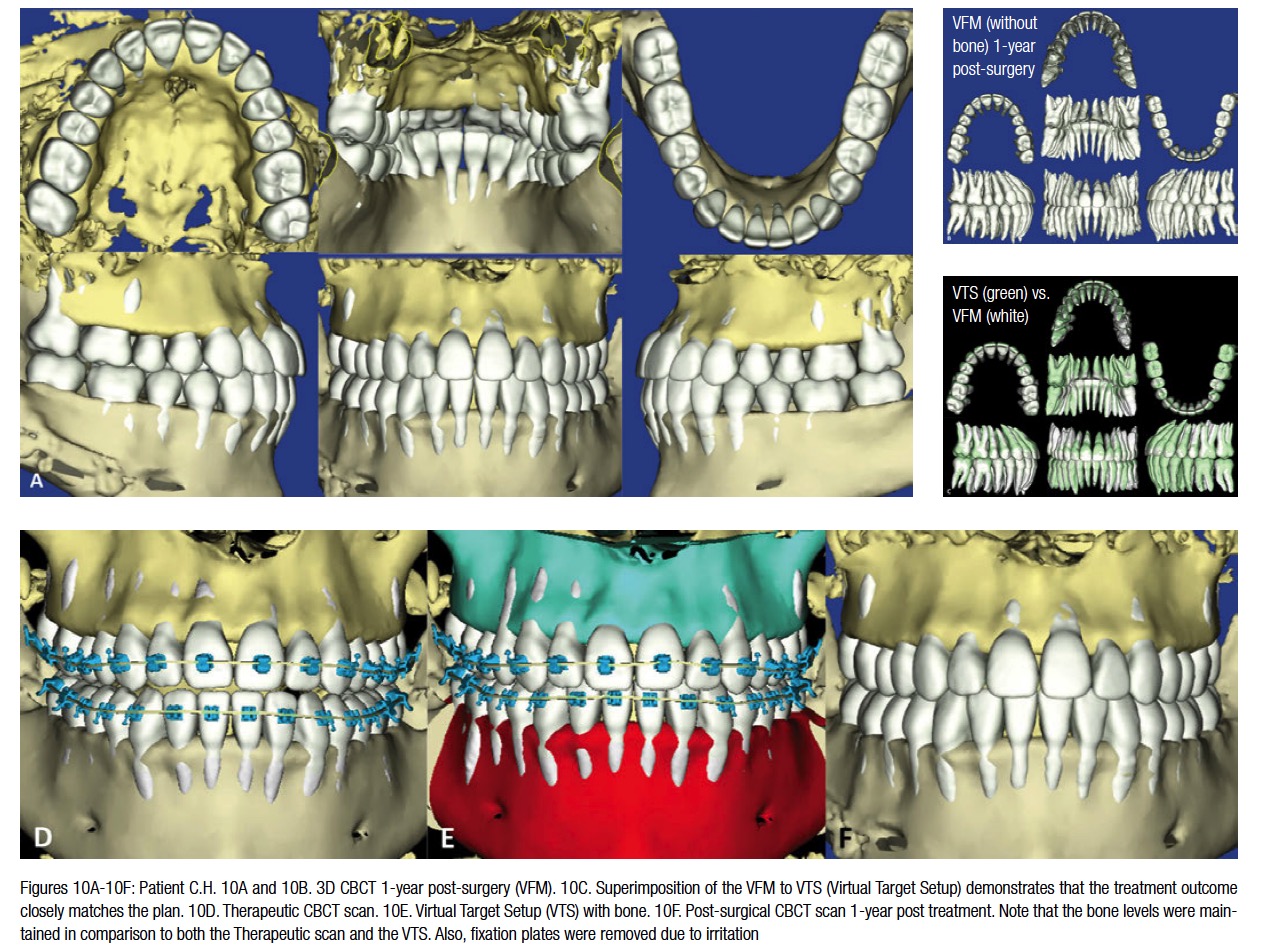
The patient was asked to wear short Class 3 elastics and scheduled to be seen 6 weeks later. The patient was debonded a month after her last appointment. The final records are shown in Figure 9. Note the Virtual Therapeutic Simulation (VTS) versus the Virtual Final Model (VFM) superimpose very closely suggesting that the planned result was achieved (Figure 10). Also, note in Figures 10D-10F, the response of the alveolar bone to treatment is seen. The doctor can observe that generally bony architecture was preserved. The soft tissue changes were favorable. One can see the final changes were similar to the animated prediction (Figure 11).
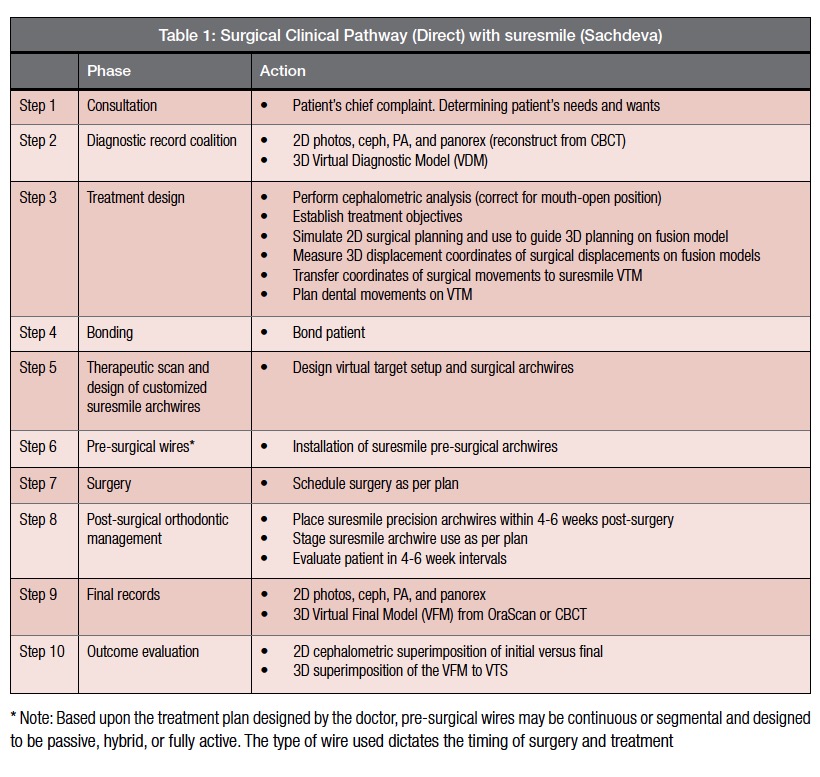
A summary of the clinical pathway developed by Sachdeva is shown in Table 1
Conclusions
The total treatment time for patient C.H. was 9 months. However, treatment for patient C.H. could have been shortened by bonding the patient and taking a diagnostic/therapeutic CBCT scan at the first appointment. The definitive surgical and orthodontic treatment plan with the surgical archwire could have been designed with this scan. This was possible since minimal pre-surgical tooth movement for the patient was required. In other words, the patient could have been set up for surgery within 6-8 weeks of initiating treatment and possibly debonded 10-12 weeks post-surgically. The total treatment time for this protocol would have been no greater than 20 weeks. Furthermore, had these clinical pathways been followed, we would have obviated the necessity of taking a second CBCT scan. This approach to care is similar to that described in an earlier paper by the senior author (Sachdeva) that describes fast-track treatment.4
 The “Direct” method using CBCT and suresmile technology provides a reliable approach to plan and manage personalized care for the surgical patient. The post-processed suresmile CBCT images allow visualization and planning of both roots and the bone position that can help the orthodontist to better plan care. Also, being able to design precision pre- and post-surgical archwires and to stage them provides unprecedented control of tooth movement. This results in a predictable treatment outcome. The “Direct” approach obviates the necessity of using the “Fusion” technique, which can be cumbersome and time-consuming. Lastly, planning with suresmile software can be performed interactively between the surgeon and orthodontist, minimizing any disconnect in treatment objectives between the caregivers. Currently, clinical testing by suresmile is underway to evaluate the suitability of using the post-processed CBCT image for designing splints directly and manufacturing them with sterolithography using a biocompatible material.
The “Direct” method using CBCT and suresmile technology provides a reliable approach to plan and manage personalized care for the surgical patient. The post-processed suresmile CBCT images allow visualization and planning of both roots and the bone position that can help the orthodontist to better plan care. Also, being able to design precision pre- and post-surgical archwires and to stage them provides unprecedented control of tooth movement. This results in a predictable treatment outcome. The “Direct” approach obviates the necessity of using the “Fusion” technique, which can be cumbersome and time-consuming. Lastly, planning with suresmile software can be performed interactively between the surgeon and orthodontist, minimizing any disconnect in treatment objectives between the caregivers. Currently, clinical testing by suresmile is underway to evaluate the suitability of using the post-processed CBCT image for designing splints directly and manufacturing them with sterolithography using a biocompatible material.
Acknowledgments
Our sincere thanks are extended to Donald Kalant, DDS, MS, (Kalant and Associates Oral and Maxillo-facial Surgery, Illinois), the surgeon on our team for his outstanding care of patient C.H. We also wish to thank Sharan Aranha, BDS, MPA, and Arjun Sachdeva for their help in the preparation of this manuscript.
 Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com for access information.
Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact improveortho@gmail.com for access information.
Dr. Takao Kubota is in private practice in Yours Orthodontic Clinic, 378-6 Motomura Yame City, Fukuoka 834-0063 Japan. He is also the co-founder of the Instiute of Orthodontic Care Improvement in Japan.
Dr. Jun Uechi is from the Department of Orthodontics, School of Dentistry, Health Sciences University of Hokkaido, 1757, Kanazawa, Ishikari-Tobetsu, Hokkaido 061-0293, Japan.
Dr. Steven Moravec is in private practice at Moravec Orthodontics, 23842 W. Main Street, Plainfield, Illinois.
- Sachdeva R. BioDigital orthodontics: Planning care with Suresmile technology: part 1 Orthodontic Practice US. 2013;4(1):18-23.
- Sachdeva R. BioDigital orthodontics: Designing customized therapeutics and managing patient treatment with Suresmile technology: Part 2. Orthodontic Practice US. 2013;4(2):18-26.
- Sachdeva R. BioDigital Orthodontics: Diagnopeutics with Suresmile technology (Part 3). Orthodontic Practice US. 2013;4(3):22-30.
- Sachdeva R. BioDigital orthodontics: Outcome evaluation with Suresmile technology: part 4. Orthodontic Practice US. 2013;4(4):28-33.
- Sachdeva R. BioDigital orthodontics. Management of Class 1 non–extraction patient with “Fast–Track”©– six month protocol: Part 5. Orthodontic Practice US. 2013;4(5):18-27.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of Class 1 non–extraction patient with “Standard–Track”©– nine month protocol: Part 6. Orthodontic Practice US. 2013;4(6):16-26.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of space closure in Class I extraction patients with Suresmile: Part 7. Orthodontic Practice US. 2014;5(1):14-23.
- Sachdeva R, Kubota T, Moravec S. BioDigital orthodontics. Part 1-Management of Class 2 non–extraction patients: Part 8. Orthodontic Practice US. 2014;5(2):11-16.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Part 2-Management of patient with Class 2 malocclusion non–extraction: Part 9. Orthodontic Practice US. 2014;5(3):29-41.
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Part 3- Management of patients with Class 2 malocclusion extraction: Part 10. Orthodontic Practice US. 2014;5(4):27-36
- Sachdeva R, Kubota T, Hayashi K. BioDigital orthodontics. Management of patients with class 3 malocclusion: Part 11. Orthodontic Practice US. 2014;5(5):28-38.
- Sachdeva RCL, Kubota T. BioDigital orthodontics. Part 1 – Management of patients with openbite (1): Part 12. Orthodontic Practice US. 2014;5(6):22-31.
- Sachdeva RCL, Kubota T,Lohse.J. BioDigital orthodontics. Management of patients with openbite (2): Part 13. Orthodontic Practice US. 2015;6(1):13-23.
- Sachdeva RCL, Kubota T, Hayashi K, Uechi J, Hasuda M. BioDigital orthodontics: Management of patients with transverse (midline) discrepancies: Part 14. Orthodontic Practice US. 2015;6(2):25-36.
- Sachdeva RCL, Kubota T, Hayashi K, . BioDigital Orthodontics-: Management of Patients with Transverse (Midline) Discrepancies (2):part 15. Orthodontic Practice. US. 2015;6(3):28-44.
- Sachdeva RCL, Kubota T, Hayashi K, Uechi J. BioDigital Orthodontics. Management of Skeletal deformities with Orthognathic Surgery: Part 1 (Part 16 of the series). Orthodontic Practice US. 2015;6(4):26-32.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
