Drs. Larry W. White and Kim Fretty discuss simple, inexpensive, and patient-friendly supplements to the Class II corrector armamentarium
Abstract
Class II malocclusions make up a large part of the difficult orthodontic maladies that clinicians must correct.
[userloggedin]
Traditional techniques, such as elastics, headgears, and removable functional appliances, have recently been supplanted with so-called noncompliant appliances that are fixed in the mouth, requiring patients to use them 24 hours per day.
While these fixed appliances have had remarkable success, the non-acceptance by many patients, the frequent breakage, and considerable cost have discouraged many orthodontists from routinely using them. Posterior occlusal guides (POGs) offer a simple, inexpensive, and patient-friendly supplement to the Class II corrector armamentarium.
Introduction
For several decades, European orthodon-tists successfully used removable functional appliances far more extensively than their American counterparts for the treatment of Class II malocclusions. This was probably due to the fixed appliances that appealed more to early leaders in American orthodontics, such as E.H. Angle and Calvin Case. Over the past 4 decades, European clinicians have endorsed fixed appliances far more than in the past. Although removable functional appliances have seemingly lost much of their appeal throughout the world, those of the fixed variety enjoy remarkable popularity, e.g., Herbst1, MARA2, MPA3, Forsus4, and so on.
The fixed functional appliances’ large allure rests upon their cemented attachments that must remain in the mouth. Doctors have enjoyed using these since they obligate patients to wear them until corrections take place. Because of this feature, they have acquired the cognomen of noncompliant appliances. However, anyone who has treated orthodontic patients for a minimum of time knows that a high level of compliance is needed for patient acceptance of the noncompliant mechanisms. There is nothing a clinician can put in patients’ mouths that they cannot remove — one way or another.
Although many patients have used these noncompliant apparatuses successfully, there are large numbers that have refused to use them or have succeeded in developing into “serial destroyers.” These latter patients break so many appliances that it finally results in doctors seeking alternate therapies.
Several features of noncompliant appliances bear responsibility for patient non-acceptance:
- the size and bulk of the appliances
- the connection that keeps the maxillary and mandibular irretrievably connected
- the interference with normal chewing for several weeks
- the unnatural and therapeutic bite it forces on the patient
- parental objections regarding the restricted movements of the appliances
Even with their recent popularity among orthodontists, these Class II appliances have a number of negative features that discourage doctors’ use:
- cost of the appliances
- need of a laboratory procedure
- patient and parental complaints
- patient refusal to wear after placement
- patient breakage of the appliances
- anterior displacement of the mandibular dentition
Clearly, an alternative to the current fixed functional appliances that is more patient friendly and easier for the orthodontic clinician to apply would be welcome. As with many discoveries in life, a serendipitous development has opened new and effective possibilities for Class II corrections that can be used both unilaterally and bilaterally.
Theory, technique, and therapeutic examples
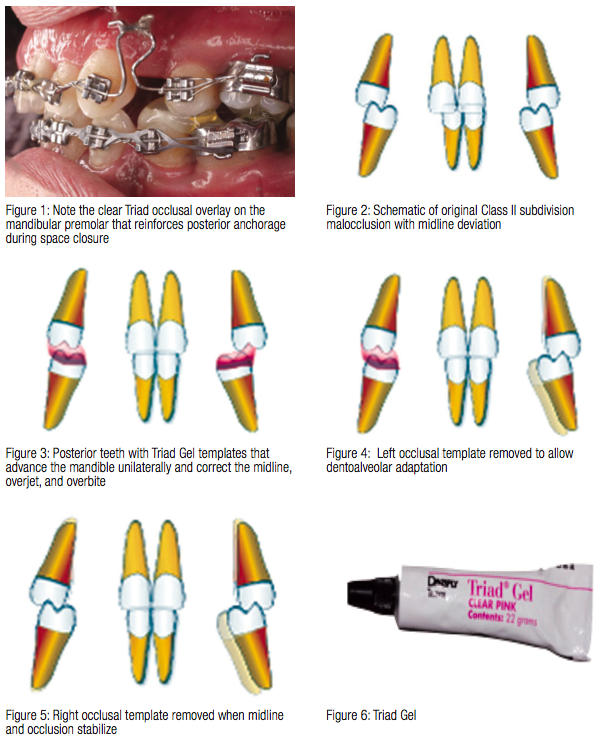 Dr. Birte Melsen and Dr. Giorgio Fiorelli5 were using Triad® Gel (Dentsply) to augment anchorage by increasing occlusal pressure on the anchor or reactive part of the orthodontic appliance (Figure 1) when Dr. Fiorelli6 discovered he could reposition the mandible and correct slight midline deviations, overjet and overbite discrepancies along with Class II subdivisions by building up the posterior teeth with Triad Gel while holding the mandible in the new position that corrected the midline, overbite, and overjet (Figures 2-7).
Dr. Birte Melsen and Dr. Giorgio Fiorelli5 were using Triad® Gel (Dentsply) to augment anchorage by increasing occlusal pressure on the anchor or reactive part of the orthodontic appliance (Figure 1) when Dr. Fiorelli6 discovered he could reposition the mandible and correct slight midline deviations, overjet and overbite discrepancies along with Class II subdivisions by building up the posterior teeth with Triad Gel while holding the mandible in the new position that corrected the midline, overbite, and overjet (Figures 2-7).
Light-cure Triad Gel is supplied in a tube with a variety of colors, but many who use this technique prefer a more viscous product. Other clinicians express a preference for the Triad material that comes as a sheet and is commonly used to make Hawley retainers or splints. The sheet’s viscosity prevents it from spreading uncontrolled and gives the operator more time to review its placement before curing with the light. Either of these Triad materials will form a useful occlusal guide, and the selection will depend on the clinician’s experience and choice. Other materials, such as bonding composites, glass ionomer cements, and others, can also serve successfully for POGs.
The posterior occlusal guides, which Dr. Fiorelli fortuitously developed, act somewhat akin to fixed functional appli-ances that can cause temporomandibular fossae and dentoalveolar remodeling7-9. He reveals this strategy with the following images of patient therapy (Figures 8-10).
Interestingly, a colleague of Dr. Fiorelli, Dr. Paola Merlo6, expanded on this idea of posterior occlusal guides and came up with a brilliant idea for intercepting Class II malocclusions in the mixed dentition. She either removes or slices the distal portion of the maxillary second primary molar, which allows her to build up a template of Triad Gel on the lower dentition that encourages the mandible to slide forward. Figures 11-17 illustrate how she guides these patients into Class I occlusion.
Patient therapy
The images shown in this article display a sequence of photos during the orthodontic therapy for a Class II subdivision patient using Posterior Occlusal Guides (POGs). The patient’s models display a firm Class I occlusion on the right side, a Class II occlusion on the left side, a lingually displaced maxillary left lateral incisor in crossbite, and a maxillary midline deviation to the left. The patient used .022 Insignia™ brackets supplied by Ormco™. Ostensibly, the Insignia formula builds first, second, and third order movements within the brackets and also supplies customized arch wires for the patient.
Figure 22 illustrates the original malocclusion, while Figure 23 displays the initial cephalometric tracing combined with the Visualized Treatment Objective (VTO). The VTO shows that the maxillary incisors lie exactly on the A Line10 and need no facial or lingual movement with only a slight amount of torque to correctly position the roots and crowns; and they need only slight extrusion. The lips have contours that closely conform to the Holdaway ideals.11,12 The mandibular incisors can move facially a slight amount with minimum intrusion.
Figures 24-31 show a series of photos from the initiation of treatment through completion of therapy. It took 4 months for the Class II side to correct into a Class I. No typical Class II mechanics, e.g., elastics, functional appliances, or headgears were used during this first phase of treatment. The patient used light Class II elastics on the left side for a couple of months near the end of therapy, but no other Class II mechanics were used at any point.
Figures 32A and 32B illustrate the after cephalometric tracing and the super-imposition of the before treatment and after treatment cephalometric tracings. The superimpositions were made by superimposing on the line S-N at the most anterior part of the sella turcica as suggested by Melsen.5 Some mandibular terminal growth is expressed by a downward and forward movement. The maxillary incisors extruded and essentially stayed in place anteriorly-posteriorly. The mandibular incisors intruded but stayed in place anteriorly-posteriorly. The maxillary molars moved forward slightly but did not extrude, while the mandibular molars showed little movement at all. Although the maxillary and mandibular incisors moved more than the VTO forecast, the extrusion and position of the maxillary incisors were the movements indicated by the prediction as was the slight amount of crown inclination. The mandibular incisors did not display the slight forward movement forecast by the VTO, but they did intrude as needed. The lips remained essentially unchanged and conform to the Holdaway norms for Caucasian females.
Discussion and conclusion
These therapies show the potential and effectiveness of posterior occlusal guides, and their ease of application should soon result in their adaptation by many orthodontic clinicians. Compared with any of the available functional Class II correctors or other Class II therapies, POGs offer several advantages such as the following:
- ease of application
- avoidance of impressions and a subsequent lab technique
- relatively low cost of application
- less interference with mastication
- their fixed nature that does not rely on patient compliance
- durability and resistance to breakage
- no restrictive mechanistic connection between the maxilla and mandible
- lack of mandibular restriction
- lack of bulky gadgetry
- less breakage and fewer patient complaints
- greater patient acceptance
- simple repairs, alterations, and removals
Although its disadvantages seem few, here are the most notable:
- their need to be replenished and supplemented as the mandible retracts
- their need of occlusion to function
- their lack of constant pressure as provided by many functional appliances
The limited and isolated therapies displayed in this paper don’t provide ironclad affirmation for their inclusion in the orthodontic armamentarium. But it is difficult to avoid the conclusion that difficult problems seem to resolve with their use.
At this time, no collection of treated patients exists. Without such a reservoir of POG therapies, their effects will require conjecture and some extrapolation. Specifically, we need to know if they anteriorly displace the mandibular dentition, retract the maxillary molars, change the occlusal plane, extrude the maxillary incisors, bend the mandible, or remodel condyles among other inquiries.13 In all probability, they should function much as other noncompliant Class II correctors, i.e., primarily by dentoalveolar changes.
Recently, a published study on Class II subdivision malocclusions found that these rather common orthodontic challenges do have significant skeletal and dental discrepancies between the Class I and Class II sides, but that two-thirds of the asymmetry is dentoalveolar.14 This suggests that POGs will work primarily by rearranging the dentition through dentoalveolar remodeling with these malocclusions.
Fortunately, the POGs represent the least invasive Class II corrector in existence. Patient acceptance is excellent, and none has reported any discomfort. Since they are bonded to mandibular posterior teeth, they work 24 hours a day, which accounts for their efficiency and effectiveness. Any breakage repairs quickly and easily. Just as with other functional appliances, POGs need additions occasionally as they affect their changes. But the added Triad bonds easily to the original by simply priming the cured material with a bonding sealant before light curing — but only after re-assuring the overbite, overjet, and midline. Upon removal, the occlusal spaces once occupied by the POGs quickly resolve by the subsequent eruption of the involved posterior teeth.
Compared with other Class II correctors, they seem to have few disadvantages, but this is early into their introduction, and it will take more experience with more clinicians to discover their limitations and specific applications.
References
1. Pancherz H. Treatment of class II malocclusions by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod. 1979;76(4):423-442.
2. Eckhart JE, White, L.W. Functional Nonextraction Treatment. Clinical Impressions. 2009;17(1):32-34.
3. Coelho Filho CM. Mandibular protraction appliances IV. J Clin Orthod. 2001;35(1):18-24.
4. Jones G, Buschang PH, Kim KB, Oliver DR. Class II non-extraction patients treated with the Forsus Fatigue Resistant Device versus intermaxillary elastics. Angle Orthod. 2008;78(2):332-338.
5. Melsen B, Fiorelli G. Biomechanics in Orthodontics. Denmark: Aarhus; 2013.
6. White LW. Orthodontic Pearls, A Clinician’s Guide. Dallas, TX: Taylor Publishing Co.; 2012.
7. Voudouris JC, Woodside DG, Altuna G, Kuftinec MM, Angelopoulos G, Bourque PJ. Condyle-fossa modifications and muscle interactions during herbst treatment, part 1. New technological methods. Am J Orthod Dentofacial Orthop. 2003;123(6):604-613.
8. Woodside DG, Altuna G, Harvold E, Herbert M, Metaxas A. Primate experiments in malocclusion and bone induction. Am J Orthod. 1983;83(6):460-468.
9. Woodside DG, Metaxas A, Altuna G. The influence of functional appliance therapy on glenoid fossa remodeling. Am J Orthod Dentofacial Orthop. 1987;92(3):181-198.
10. Alvarez A. The A line: a new guide for diagnosis and treatment planning. J Clin Orthod. 2001;35(9):556-569.
11. Holdaway RA. A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part I. Am J Orthod. 1983;84(1):1-28.
12. Holdaway RA. A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part II. Am J Orthod. 1984;85(4):279-293.
13. Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara JA Jr. Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthod Dentofacial Orthop. 2006;129(5):599, e1-12, e1-6.
14. Minich CM, Araújo EA, Behrents RG, Buschang PH, Tanaka OM, Kim KB. Evaluation of skeletal and dental asymmetries in Angle Class II subdivision malocclusions with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2013;144(1):57-66.
Gallery
{gallery}140322_white{/gallery}
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
