Drs. Larry White and Francesca Scilla Smith show promising techniques for treating impacted mandibular second molars.
Drs. Larry W. White and Francesca Scilla Smith offer a technique to simplify a complex and lengthy procedure
Introduction
Nothing slows the completion of orthodontic therapy as the failure of impacted mandibular second molars to erupt or achieve eruption through surgery and subsequent orthodontic intervention. Still, surgical intervention adds to the cost, trauma, and duration of treatment for the patient and doctor. Many clinicians have suggested several approaches to this continuing problem, and this article will review some of those techniques as well as illustrate a recent development that holds great promise in simplifying this difficult and time-consuming chore.
Previous techniques
Pool1 introduced an innovative and simple method of uprighting semi-impacted mandibular second molars in the 1970s; however, the second molar needs to have a measure of eruption, so the mechanism can be placed (Figures 1A, 1B, and 1C).

At the dawn of bracket bonding in 1977, Rubin2 developed a technique that also required partial eruption of the ectopic erupting mandibular second molar. This took advantage of early bonding materials, and he was able to bond an auxiliary uprighting spring to the occlusal surface of the molar (Figure 2).
In 1987, Orton and Jones3 suggested another tack for uprighting semi-impacted mandibular second molars that relied on the ability to bond a tube on the partially erupted second molar and, essentially, reversed the uprighting spring assembly of Rubin (Figure 3).

One of the most novel ways of deimpacting ectopic erupting mandibular second molars was developed by Dr. Bach4 (Figures 4-8). Dr. Bach has created a nonsurgical method for uprighting ectopic molars that has an elegance and simplicity heretofore unseen. It neither requires special instrumentation nor depends on laboratory construction of a special appliance. Although the ectopic molar appears to contact the tooth it abuts, there is a space between the two teeth that Dr. Bach exploits in an un-usually effective manner. He depends on a highly flexible wire — usually a CuNiTi .016 — to elevate the ectopic molar with the following approach by inserting the short NiTi wire vertically along the distal marginal ridge of the first molar so that it clears the mesial marginal ridge of the impacted second molar. He then bends the visible vertical wire over the occlusion of the first molar and secures it with some compomer; e.g., Band Loc®, (Reliance Orthodontic Products).


Dr. Bach uses wires as small as .013 CuNiTi but no larger than .014 x .025 CuNiTi and leaves the wire in until the target molar uprights, and he then bonds a tube to it.
With the advent of miniscrews and bone plates, clinicians5,6 have developed multiple ways of using them as anchorage to upright and retract the impacted molar. Most of the techniques previously described require surgical uncovering or, at a minimum, the partial eruption of the impacted molar. Once either of those occurs, an attachment can be bonded, and several methods can retract the tooth. A popular and simple method is to add a NiTi open-coil spring to push the ectopic molar distally (Figure 9).


A new technique for uprighting and erupting ectopic molars
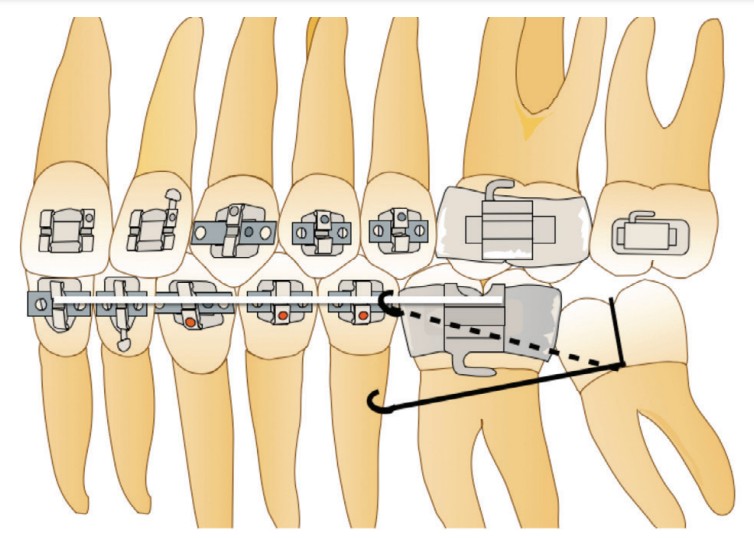
The technique described in this article offers an additional way of uprighting and retracting the molar without resorting to surgery and is similar in concept to the Bach technique, but avoids the occlusal bonding of the NiTi wire to the first molar. A .014 NiTi wire is piggybacked to the principal wire in the posterior quadrant (first molar, first and second premolars) and ligated with stainless steel wires plus O-rings (Figures 10-13). This wire extends beyond the first molar by the approximate width of the ectopic second molar.
The clinician then holds the secured .014 NiTi with a hemostat or pliers and pushes it below the crown of the first molar, which will allow it to contact the mesial surface of the impacted molar’s crown (Figure 12).
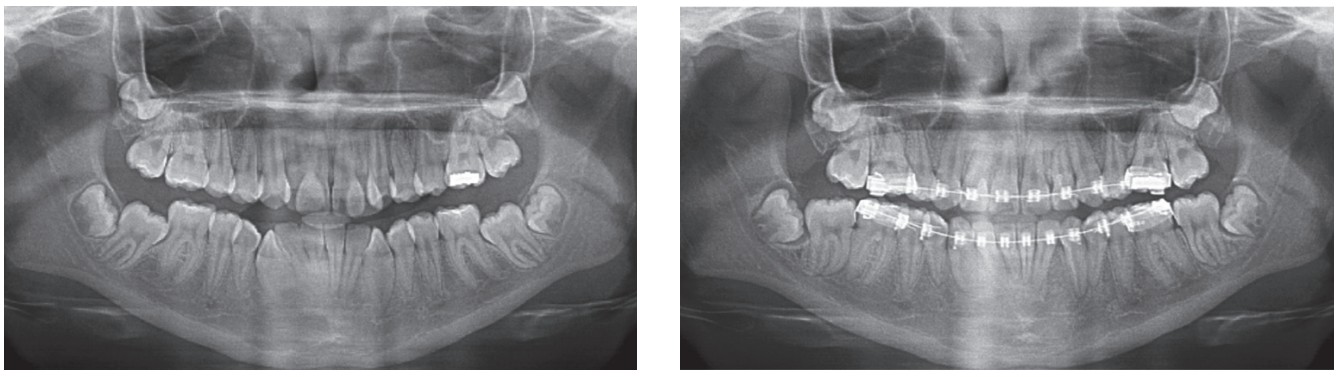
The panograph X-rays in Figures 12 and 13 illustrate the effect this wire had on the impacted molars in 5 weeks.
Summary
The avoidance of surgery and a complete orthodontic solution to upright and erupt ectopic molars offers patients and doctors several advantages:
- Avoids considerable trauma for the patient.
- Avoids extra expense to orthodontic therapy.
- Avoids the incomplete uncovering of the ectopic molar that can make the bonding of attachments difficult to impossible to do.
- Avoids secondary uncovering.
- Offers a relatively painless and rapid resolution to an ordinarily slow and difficult procedure.
Orthodontic clinicians can apply this therapy without needing additional supplies. The auxiliary .014 NiTi wire securely attaches to the principal wire and has little opportunity of breakage or loosening.
One final caveat for clinicians — will this new method prove efficacious and efficient for every patient with ectopic erupting mandibular molars? Probably not. Still, based on the limited but impressive results so far, we remain optimistic about its potential to simplify one of the most complex and lengthy procedures that orthodontists encounter.
Besides impacted mandibular second molars, Drs. White and Smith have explored treatments for cuspids. Read “Examining the Dental Canon” here: https://orthopracticeus.com/examining-the-dental-canon/
 Larry W. White, DDS, MSD, FACD, is a graduate of Baylor Dental College and Baylor Orthodontic Program and now has an orthodontic practice in Dallas, Texas.
Larry W. White, DDS, MSD, FACD, is a graduate of Baylor Dental College and Baylor Orthodontic Program and now has an orthodontic practice in Dallas, Texas.
 Francesca Scilla Smith, DDS, MS, was born and raised in Arezzo, Italy. She graduated summa cum laude at the University of Florence Dental School and obtained her orthodontic degree from Nova Southeastern University College of Dental Medicine in Fort Lauderdale, Florida, with a master thesis on conventional and digitally driven indirect bonding. Dr. Scilla Smith practices orthodontics in Dallas, Texas.
Francesca Scilla Smith, DDS, MS, was born and raised in Arezzo, Italy. She graduated summa cum laude at the University of Florence Dental School and obtained her orthodontic degree from Nova Southeastern University College of Dental Medicine in Fort Lauderdale, Florida, with a master thesis on conventional and digitally driven indirect bonding. Dr. Scilla Smith practices orthodontics in Dallas, Texas.
- Pool H. Orthodontic Pearls: A Clinicians Guide. White LW (ed). Taylor Publishing Co.; 2012.
- Rubin RM. Uprighting impacted molars. J Clin Orthod. 1977;11(1):44-46.
- Orton H, Jones S. Correction of mesially impacted lower second and third molars. J Clin Orthod. 1987;21:176-181.
- Bach RM. Non-surgical uprighting of mesially impacted lower molars. J Clin Orthod. 2011;45(12):679-681.
- Tseng YC, Chen CM, Chang HP. Use of a miniplate for skeletal anchorage in the treatment of a severely impacted mandibular second molar. Br J Maxillofac Surg. 2007;46(5):406-407.
- Zhen J, Liu CH, Zhang WX, et al. Uprighting deeply impacted mandibular second with miniscrew anchorage. J Clin Orthod. 2019;53(7):405-413.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
