Drs. David M. Sarver and W. Eugene Roberts write that superelastic archwires deliver the right amount of force for a specific tooth to achieve efficient movement and reduced trauma to the PDL. Read more details about this new generation of technology.
Drs. David M. Sarver and W. Eugene Roberts discuss a new generation of multi-force archwires
Introduction
Superelastic archwires have been commonly used in orthodontic practices for over 2 decades, and these archwires have been based primarily on nickel-titanium materials. These archwires are relatively uniform in their force delivery across the arch form, meaning that force levels are ideal for some teeth, but not for others. What do I mean by that? Just think about the periodontal ligament (PDL) surface area of a maxillary lateral incisor versus that of the maxillary first molar. The force needed to move a first molar is much greater than what is needed to produce similar movement of a lateral incisor. Current archwire technology results in appropriate force levels in some areas of the mouth, but not in others. This may be expressed in many ways, such as irregular progress in correcting malocclusion and a tendency for increased root resorption on susceptible teeth like maxillary lateral incisors.
What is new in superelastic archwire technology?
The current generation of superelastic wires are all resistant to permanent deformation, deliver relatively uniform force, and have a lower modulus of elasticity compared to stainless steel and TMA wires. A new generation of multi-force archwire has been developed that has differential superelastic properties based on advanced concepts in materials science and PDL physiology.
What makes the new arch wire different from copper-nickel-titanium (CuNiTi) superelastic wires?
What if you could have an archwire that is “programmed” to deliver loads that are specific for each tooth in the arch? For example, a lighter force delivered to lateral incisors, and a heavier one for molars? Basically, that is the idea behind the development of a multi-force archwire. Using pulsed fiber laser conditioning of shape memory alloy (SMA) wires such as copper-nickel-titanium (CuNiTi), a patented multiple memory material concept can precisely program narrow transition zones with numerous superelastic unloading profiles programmed into a single CuNiTi wire. The idea is to simply deliver the right amount of force for a specific tooth to achieve efficient movement and reduced trauma to the PDL.
Clinical study
How does this new archwire technology compare to CuNiTi ?
Study A: A single 0.016″ Ormco SmartArch™ laser-engineered CuNiTi technology produced 25% faster (143 vs. 180d for controls), and >56% more efficient initial alignment because of fewer residual discrepancies, improved deepbite correction, and a reduction of the curve of Spee.1
Study B: In approximately 6 months, two SmartArch wires (0.016″ for 111days followed by 0.017″ x 0.025″ for 87 days) corrected axial inclinations in 3D to a near ideal alignment (cast discrepancies <29 points).1
In comparison, it usually requires about 6 months to only align a crowded lower arch with routine CuNiTi and stainless steel (SS) archwires. The bottom line is two SmartArch wires are more effective than 4-6 routine archwires for correcting malocclusions with a deepbite >3mm (>75% of all malocclusions in the total sample of 50).1
Why are multi-force SmartArch archwires more rapid and efficient for tooth movement?
- Optimizing the load (moment-to-force ratio) for individual teeth is important for PDL health. Like all archwire activations, SmartArch results in some areas of PDL necrosis when it is first engaged, but there is only one archwire change during treatment, and that is when the rectangular SmartArch is installed. In effect, gentle continuous force accomplishes the treatment with minimal PDL necrosis because only two archwires are
- Since molars have the largest PDL/bone interface, SmartArch archwires are stiffer in the posterior compared to anterior segments. Thus, anterior crowding is corrected with gentle force at the same time the arch is leveled with the same archwire.1
Case examples
Case 1
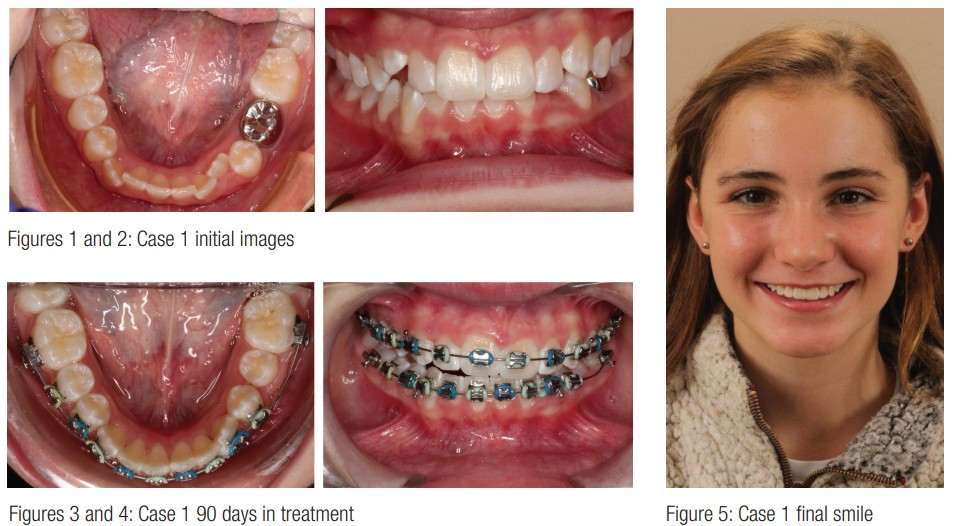
This 12-year-old patient was referred for correction of her moderate Class II deep bite malocclusion. She represents a patient in the initial study of the 90 days in the 0.016″ SMA group. Her initial images were gathered (Figures 1 and 2), and she was submitted for setup using the Insignia™ (Ormco) appliance. When we received the setup, the brackets were bonded and the 0.016″ archwire placed, and the alignment after 90 days showed good alignment of the lower arch and overcorrection of bite opening (Figures 3 and 4).
Conclusion/critiques
I would have reset the lower left canine rotation prior to the photograph, but that would have contaminated the data of our study. The significant observation in her case is how efficiently the bite was opened in 90 days with one continuous archwire. SmartArch delivered gentle and continuous forces that were preferred for optimal tooth movement and patient comfort.
Case 2
This 12-year-old girl was referred by her dentist for consultation regarding her severe crowding (Figure 6).
She had totally blocked out her mandibular left canine, and her leeway space had been held during her transitional dentition with a lingual arch. However, she still had quite a bit of crowding, but a reasonable posterior occlusion (Figure 7).

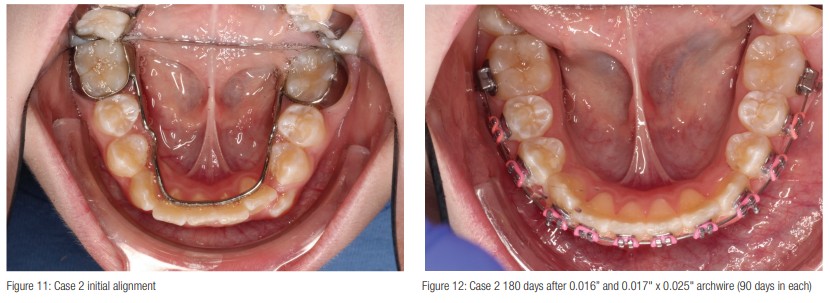
The patient was clearly mandibular-deficient (Figure 8) and had a good vertical incisor display, smile arc, and maxillary projection, while the maxillary incisors were slightly retroclined in compensation for the mandibular deficiency (Figure 9). I performed a setup (Figure 10) for a lower incisor extraction, but the outcome showed an unacceptable amount of overjet. In consultation with the periodontist, we agreed on an approach utilizing biomimetic grafting material to reinforce periodontal root structure in preparation for orthodontic treatment. This was achieved using Emdogain® (Straumann®) (enamel matrix derivative) with synthetic bone grafting (EDTA) preparation. Approximately 4 months after the graft was placed, treatment was initiated with full-fixed appliances (Titanium Orthos™, Ormco), and 0.016″ SMA archwires (SmartArch) were placed in both arches. Three months later 0.017″ x 0.025″ SMA archwires were placed (Figures 11 and 12).
Conclusion/critiques
Treatment time can be more efficient by engaging the posterior teeth at the beginning of treatment and minimizing repetitive archwire adjustments. Significant changes had occurred 180 days after initial archwire placement and two archwires (Figures 11 and 12).
Conclusion
Conventional wire progressions step through multiple rounds of progressively greater size and force. That approach challenges the variable root biology throughout the arch, introducing multiple episodes of lag phase prior to tooth movement. Inevitably, this prolongs treatment times. In both cases, SmartArch wire technology — a patented, highly controlled application of pulsating, precision laser energy to predetermined portions of the memory shape CuNiTi archwire — avoided these lag phases. Our clinical study demonstrated that SmartArch averaged approximately 50% greater tooth movement than the control group comprised of standard CuNiTi archwires. Clinicians are able to engage anterior and posterior teeth for more efficient leveling and aligning. Clinicians may also schedule longer intervals between appointments. Retrospectively, it appears the best time to begin treatment with SmartArch is upon full eruption of the second molars. This takes full advantage of posterior molar uprighting from Day One.
After reading about superelastic archwires, check out an article about the early days of nitinol wire. Read the interview with Dr. Patrick Brady here. https://orthopracticeus.com/columns/conversation_with_brady.
- Roberts WE, Roberts JA, Tracey S, Sarver, DM. SmartArch® Multi-Force, Super-Elastic Archwires: A New Paradigm in Orthodontics. Journal of Digital Orthodontics. 2019;55. https://iaoi.pro/archive/post/id/328. Accessed October 8, 2019.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
