Dr. John Hayes encourages orthodontists to use the scientific method to discover the “why” before treatment.
Dr. John L. Hayes discusses the importance of discovering the why before treatment
Abstract
The “scientific method” was promoted by Francis Bacon (1561-1626) as a way to help move the society of his day away from old beliefs and superstitions. He believed that nothing was discovered without the scientific method and that scientists attempt to answer why. This article can serve as an example how the scientific method helped formulate a theory regarding the etiology of some malocclusions.
Introduction
Physicians and dentists learn about the scientific method as part of their education. In the process of research, there is usually an attempt to follow the scientific method. Here is the regimen:
- Formulate a hypothesis.
- Gather data.
- Analyze the data.
- Determine whether the findings support the hypothesis or not.
- Accept the hypothesis, or adjust the hypothesis, and repeat the process as necessary.
Sometimes research does not call for a hypothesis. In that scenario, the initial steps become 1) gather data and 2) analyze the data — without adherence to the scientific method. Nevertheless, the gathered information can add to the understanding of some topic even if a theory is not proposed.
Francis Bacon (1561-1626) is usually given credit for the development and promotion of the scientific method. He was a bright light of that age; he believed that if conditions were to improve for the common good, there needed to be a methodical way to help discover those means. Bacon saw the scientific method as “the way.” Nothing got discovered without the scientific method, according to Bacon.1
Bacon also said that that “idols” [old beliefs and superstitions] needed to be purged in order for the “scientific method” to succeed. Albert Einstein said it differently 400 years later: “The only thing that interferes with my learning is my education.”1,2,3
Moreover, Bacon stated that a scientist is not like a spider. “A spider weaves his own web” (think armchair theorist). Bacon further stated that a scientist is also not like an ant. An ant collects facts but does not create theories that explain the facts. Bacon held that a scientist must be like a bee. A bee collects, digests, and makes something new — honey. A scientist attempts to answer why.1
About 200 years later, in the early 1800s, four students at Cambridge University studied Bacon’s ideas over their Sunday “breakfast meetings.” Those students — William Whewell, Charles Babbage, John Herschel, and Richard Jones — went on to promote Bacon’s scientific method and to change the world.4
Discussion
The scientific method was invented in hope of improving the chances for the discovery of ideas that would benefit society. This method of discovery can be applied to any orthodontic malady in which the why (the etiology) is uncertain or unknown.
Exhibit 1
A common perception is that the causes of the malocclusions are, for the most part, unknown. Etiology is a black box. Treatment plans that do not address etiologies necessarily address only the symptoms of malocclusions. If the scientific method were to be applied to our unknowns and their etiologies were to be discovered, our treatments would be more efficient and lasting.
Thirty years ago a new theory of malocclusion was imagined — the intervening years were necessary to gather enough data, consistent with the scientific method, to be sure that enough data had been gathered. When the theory was first proposed, a pilot study was performed; when the theory held true, a 10-year study was then undertaken, also patterned after the scientific method. Data was continued to be gathered from published anthropologic studies and natural history museum visits over the past three decades. Over 7,000 patients in one private practice were treated to the goals and carefully evaluated. (Charles Darwin — a strong proponent of the scientific method — published On the Origin of Species in 1859 after 23 years of data gathering subsequent to his voyage on the good ship, Beagle.)
Axel Lundstrom (1875-1941) said that old and prehistoric arches exhibited “Harmony” that would be obvious when one saw it. However, Lundstrom admitted that he had no idea how to replicate the Harmony – he thought that the apical base was involved.5 Clinicians may be aware that old and prehistoric skeletal arches exhibit teeth that are well aligned and in a Class I relationship — with unquestioned stability throughout life. We were curious to discover the reason for the exceptional alignment and stability.5,6,7
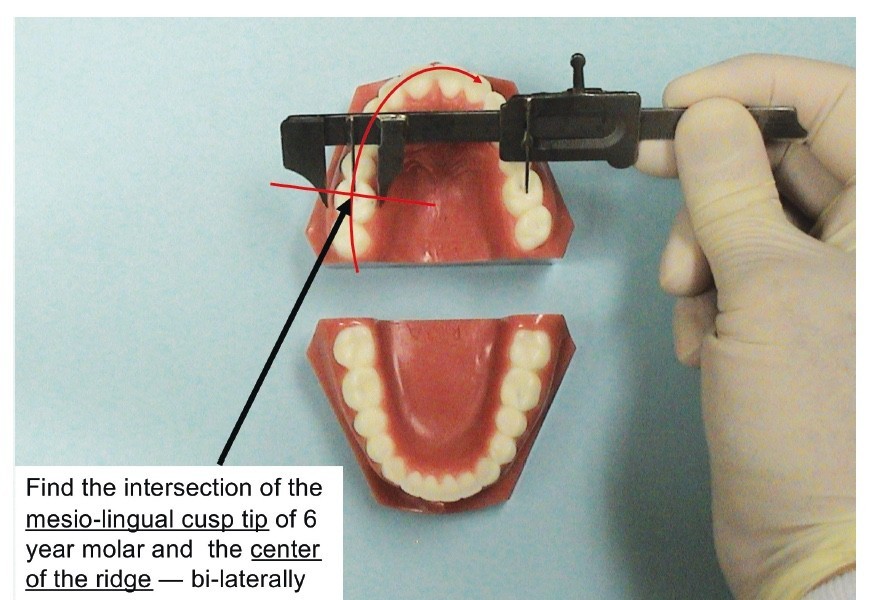
The theory is based on skeletal measurements of the alveolar ridge crests and the constant differential of 5 mm that was found with hundreds of old and prehistoric arches that were examined.
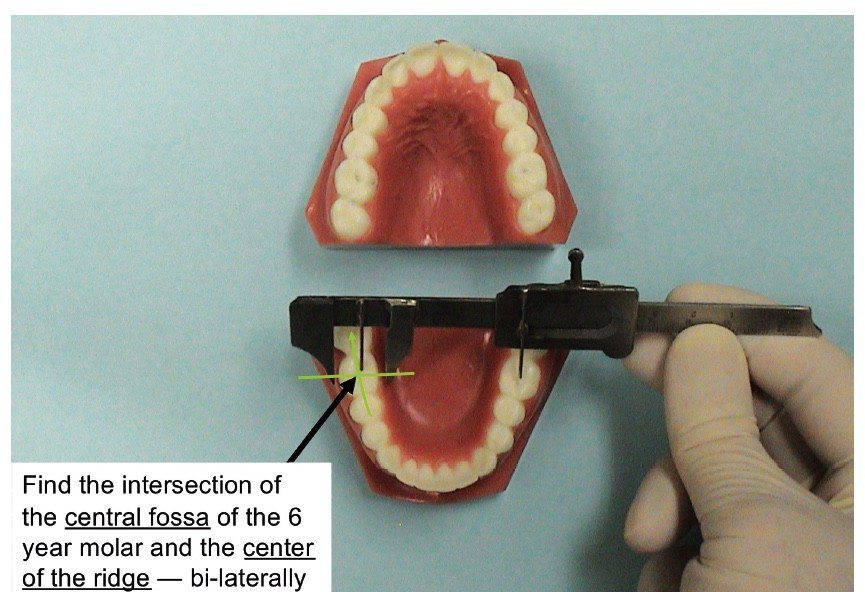
Exhibits 2 and 38,9,10,11,12
Consider the theory that malocclusions are primarily caused (proposed from experience, arguably, at 80%) by a transverse deficient maxillary arch when measured at the 6-year molars at the center of alveolar crests (CAC) technique. It is important to understand that the 80% estimate is an educated guess — it could be less; it could be a higher — but the exact percentage is not really the point. Etiology is the point. The other 20% of malocclusions are not related to a maxillary transverse deficiency but rather to causes such as premature loss of primary teeth, congenitally missing teeth, and untoward oral habits, etc. A typical orthodontic patient, in our experience, has some degree of transverse deficiency along with non-transverse related problems such as untoward oral habits along with premature loss of some primary teeth.
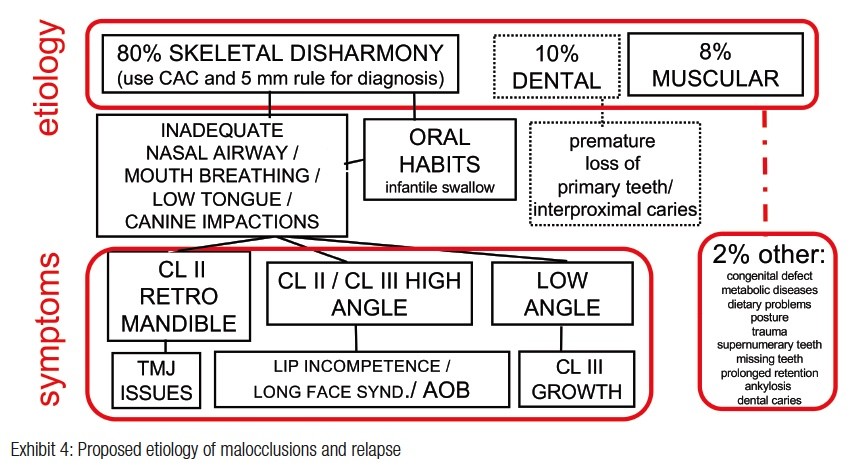
The etiology of many malocclusions — Exhibit 46,8,13,14
Exhibit 4 is a flow chart revealing that subsequent to a transverse deficiency, several different symptoms are possible. The theory defines an ideal maxillary arch when the mandibular CAC + 5 mm = maxillary arch CAC. The maxillary arch is transverse-deficient if it does not meet the 5 mm differential criteria. The measurement technique has been proven accurate. “Due to the diagnostic validity of the Penn analysis (CBCT based) and the CAC analysis (model based), they can be considered as the new gold standards for the precise diagnosis of transverse skeletal discrepancies.”8,15
After over 30 years of investigation and application, the theory can be considered to be a skeletal orthopedic law until proven otherwise.
Because malocclusions have been deemed mostly “unknown,” so-called progress has led to the invention of new devices to help address the symptoms of malocclusions and not the root causes. New devices can even be touted as “cures.” Eventually, a short-term solution can lead to relapse. Accordingly, labeling malocclusions as unknowns has held back orthodontic progress with diagnosis and treatment. Think back to Francis Bacon’s warning over 400 years ago: idols (false beliefs) must be purged in order for discovery take place.
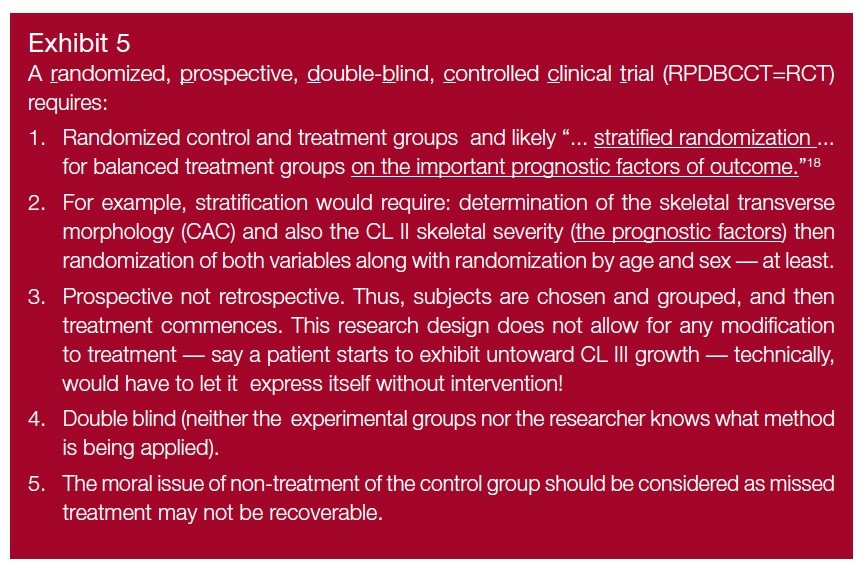
RCTs — Exhibit 5
RCT — an acronym for a randomized controlled trial — is a shortened version of RPDBCCT, or randomized, prospective, double-blind, controlled, clinical trial. Some research has been touted as a RCT when it was not. A famous Abraham Lincoln saying bears repeating: “Say a dog’s tail is a leg; now how many legs does a dog then have? Five! No, saying a dog’s tail is a leg does not make it so.”6 Saying that some research is a RCT does not necessarily make it so.
It can be argued that a bona fide RCT is actually not fully feasible with orthodontic treatment for a few reasons: First, double blind is an obvious stumbling block. Second, it is not feasible to treat an orthodontic patient without normal, necessary orthodontic “adjustments” as needed —“adjustments” are simply not allowed with a RCT. Third, leaving one group behind (the untreated control group as part of the controlled design) can be a moral failure because of the lost opportunity for timely care.1
Most importantly, the root cause of a particular orthodontic malady (the confounding variable) needs to be controlled for a real RCT. No confounding variable? No real RCT. “Age” and “sex” are commonly controlled, however, age and sex are not the causes of a malocclusion.
Conclusions
- The scientific method is used to discover the why of something (referred to as the prognostic factor or the etiology).
- Not all research uses the scientific method; not all research attempts to discover the why of something.
- Once the why is determined, further research can be performed (RCTs?).
- To perform an RCT, the first priority would be to determine the prognostic factor (the etiology, found by way of the scientific method).
- Once the prognostic factor of a malady is known, orthodontic treatment can be directed toward a patient’s malady.
- Treating the etiology of a malady is more effective than treating the symptom of a malady.
- In this article, the scientific method has been used to propose a theory of malocclusion. When skeletal arches are measured by the CAC technique, there is a 5 mm maxillary/mandibular differential that mimics the differential found with old and prehistoric skulls. Those old and prehistoric skulls deserve to be mimicked.
Dr. Hayes has explored the why before treatment in past articles. For more on the subject, check out “In search of the etiology of malocclusions — a common discovery technique is proposed.”
https://orthopracticeus.com/orthodontic-concepts/in-search-of-the-etiology-of-malocclusions-a-common-discovery-technique-is-proposed.
 John L. Hayes, DMD, MBA, received his dental degree from the Boston University, H.M. Goldman School of Graduate Dentistry, and his orthodontic certificate from the University of Pennsylvania, School of Dental Medicine, Orthodontic Depart-ment, where he is a Clinical Associate. He continues to research and lecture on the advantages of early interceptive treatment and on the etiology of malocclusions. Dr. Hayes is in private practice in Williamsport, Pennsylvania, with his wife, Sharon, who is also an orthodontist. He can be reached at jhayesortho@comcast.net.
John L. Hayes, DMD, MBA, received his dental degree from the Boston University, H.M. Goldman School of Graduate Dentistry, and his orthodontic certificate from the University of Pennsylvania, School of Dental Medicine, Orthodontic Depart-ment, where he is a Clinical Associate. He continues to research and lecture on the advantages of early interceptive treatment and on the etiology of malocclusions. Dr. Hayes is in private practice in Williamsport, Pennsylvania, with his wife, Sharon, who is also an orthodontist. He can be reached at jhayesortho@comcast.net.
- Klein J. Francis Bacon. The Stanford Encyclopedia of Philosophy Edward N. Zalta, ed. Winter 2016 Edition. https://stanford.library.sydney.edu.au/archives/win2016/entries/francis-bacon/. Accessed February 23, 2020.
- Lightman A. The Discoveries: Great Breakthroughs in 20th Century Science. Vintage reprint edition: Canada; 2009.
- Einstein A. Brainy Quote. https://www.brainyquote.com/quotes/albert_einstein_110208. Accessed February 23, 2020.
- Snyder LJ. The Philosophical Breakfast Club: Four Remarkable Friends Who Transformed Science and Changed the World. Broadway Books, The Crown Publishing Group, a division of Random House: New York, NY; 2011.
- Lundstrom AF. Malocclusion of the teeth regarded as a problem in connection with the apical base. International Journal of Orthodontia, Oral Surgery and Radiography. 1925;11(12):1109-1133.
- Hayes JL. Orthodontics, chapter 10. In: Owsley DW, Jantz, RL, eds. Kennewick Man: The Scientific Investigation of an Ancient American Skeleton. College Station, TX: TAMU Press; 2014.
- Johanson DC, Edgar B. From Lucy to Language. 1st ed. New York, NY: Simon & Schuster; 1996.
- Hayes JL. In search of improved skeletal transverse diagnosis. Part 2: A new measurement technique used on 114 consecutive untreated patients. Orthodontic Practice US. 2010;1(4):34-39.
- Hayes JL. A new regimen of phase I care applied to anterior open bite — 10 case studies: an etiology proposed by the strategy of triangulation. Orthodontic Practice US. 2012;3(3):18-26.
- Hayes JL. A new regimen of Phase I care applied to potential canine impactions. Orthodontic Practice US. 2013;4(3):44-51.
- Hayes JL. In search of the etiology of malocclusions — a common discovery technique is proposed. Orthodontic Practice US. 2018;9(5):60-64.
- Hayes JL. In search of … [etiology of malocclusions]. Orthodontic Practice US. 2019;10(3):1.
- Hayes JL. Williamsport Orthodontic Study. Penn Ortho Alumni database. 2009.
- Price WA. Nutrition and Physical Degeneration. Price-Pottenger Nutrition Foundation, ed. 8th ed. Lemon Grove, CA: Price-Pottenger; 2007.
- Gonzalez AG Gonzalez AG, López AF, Fernández ST, Ocampo AC, Valencia JE. Sensitivity and specificity of a radiographic, tomographic and digital model analysis for determining transverse discrepancies. Revista Mexicana de Ortodoncia. 2018;1(6):26-32.
- Lincoln A. Quote Investigator. Quote attributed to Abraham Lincoln by 1862. Variants since 1825. https://quoteinvestigator.com/2015/11/15/legs/. Accessed February 23, 2020.
- Hayes JL. Problems with RCT design. Am J Orthod Dentofacial Orthop. 2009;136:143-144.
- Koletsi D, Pandis N, Polychronopoulou A, Eliades T. What’s in a title? An assessment of whether randomized controlled trial in a title means that it is one. Am J Orthod Dentofacial Orthop. 2012;141(6)679-685.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
