Editor’s intro: Dr. Bryan Lockhart’s solution to the many challenges to treatment for this patient involved a multi-faceted approach to treatment.
Dr. Bryan Lockhart addresses this patient’s skeletal Class III malocclusion, while correcting the anterior crossbite and obtaining positive overjet
Introduction

The adult orthodontic patient often presents a special set of complexities that requires careful analysis and diagnosis. Complications include missing teeth, heavily restored teeth, and periodontal issues (to name a few). Another factor to consider is compliance, especially when modalities such as elastics are required. This is critical because growth cannot be manipulated to aid in the correction of the malocclusion as it can in growing patients. Furthermore, adult patients often require more “coaching” as a lot of them do not like the social distractions that elastics can cause, and treatment time is extremely important. Adult patients want to be in treatment for the shortest time possible without compromising on the results. All of these factors must be taken into consideration before undergoing treatment with adult patients.
Case presentation/diagnosis
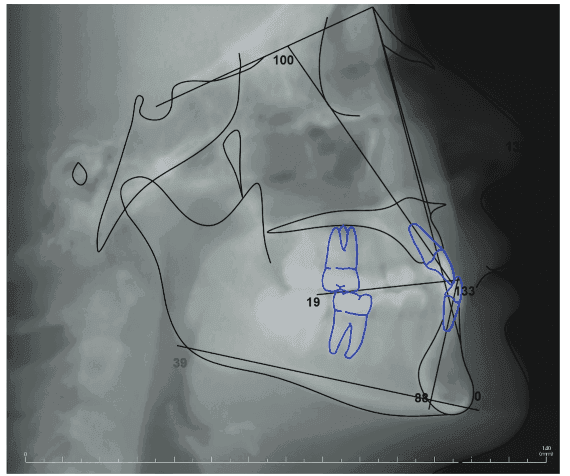
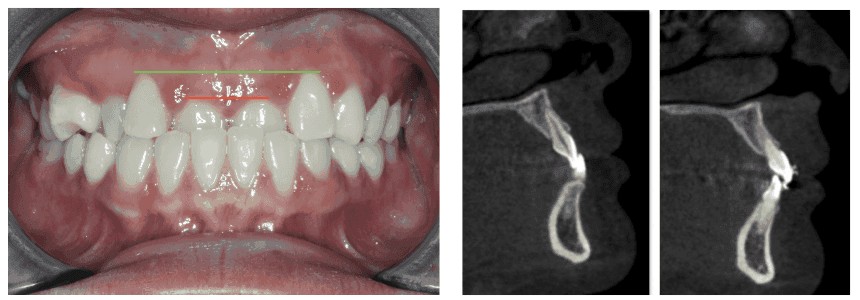
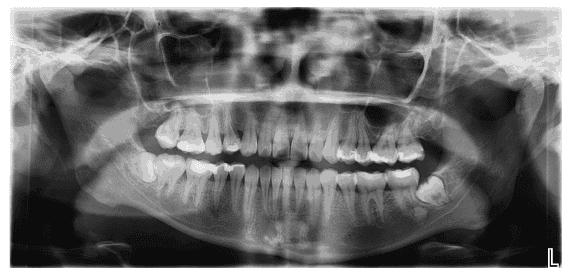
This case will look at a situation where a 22-year-old adult female (Figures 1A and 1B) expressed her chief concern of not liking how her two front teeth fit behind her lower front teeth. She has a Class III concave profile with a mildly retrognathic maxilla (Figure 2) and normal face height with balanced facial thirds. Dentally, she maintains a Class III molar relationship with an accompanying anterior crossbite involving her maxillary central incisors and maxillary right canine. Her maxillary and mandibular incisors are retroclined with a mandibular curve of Spee of 3 mm. Additionally, she presents with supra-erupted maxillary central incisors, and a maxillary right first premolar that is rotated nearly 90 degrees. Finally, the patient also has uneven gingival zeniths in her maxillary anterior region, mainly in part to the supra-erupted central incisors (Figure 3).
This case is particularly interesting because the patient presents with a mild skeletal Class III malocclusion that was too minimal to warrant orthognathic surgery. This issue caused us to search for alternative solutions to camouflage a skeletal discrepancy by incorporating dental movements only. Camouflage treatment can be particularly challenging because we are not able to correct the true cause of the malocclusion, which limits us to simply “mask” the discrepancy. Managing her expectations was critical because she wanted a “perfect” smile which is limited by periodontal support, shape, size, and color of her teeth. Helping her understand that we were treating her skeletal issue nonsurgically was paramount in allowing us to deliver a result that she could be happy with.
Treatment objectives
- Correct the anterior crossbite
- Resolve maxillary and mandibular crowding
- Correct molar classification to Class I
- Improve torque of the maxillary incisors
Treatment alternatives
- Surgery: Maxillary premolar extractions and LeFort 1 maxillary advancement
Treatment plan
The non-extraction treatment plan involves aligning her maxillary and mandibular teeth, and correcting the anterior crossbite via proclination and intrusion of the maxillary central incisors. This plan will aid in leveling the gingiva in the maxillary anterior region. The excessive lower curve of Spee will be corrected by leveling the lower arch along with Class III elastics for sagittal correction.
Treatment plan sequencing
The patient was given the option of treatment with either metal braces, clear/ceramic braces, or clear aligners. The patient opted for ceramic braces because she was concerned about her potential noncompliance with clear aligners, but still wanted a more esthetic option than metal braces.
The patient was bonded with Symetri™ Clear brackets (Ormco), MBT prescription .022 slot. I chose Symetri for ceramic brackets because it’s not as bulky as other options, and the edges are smooth instead of sharp and rough.
Bite turbos for disarticulation were placed on the lower central incisors at the initial appointment. Light wires (0.014 nitinol) were used for a longer period to align her maxillary right first premolar in an effort to minimize exacerbating recession of No. 5. Lingual buttons were placed on the lingual of the first and second maxillary right premolars, and power chains were placed to help derotate her maxillary first premolar.
Archwires were advanced to 0.018 NiTi and Class III elastics from maxillary first molars to lower cuspids; light 1/4 medium were worn. Archwire sizes were increased to .021″ x .025″ NiTi to gain more buccal crown torque on her maxillary incisors, and the elastics sizes were increased to 3/16 heavy on the right side only. The proper angulation was obtained while preserving bone facial to the roots of the central incisors shown in Figure 4.
Overall, a nice occlusion was obtained, and her arch form was improved as well.
Having a reliable bracket system designed for refined strength to express the correct amount of torque, and a motivated patient with elastic wear led to great improvement in her smile, a solid bite, and a very happy patient (Figure 5). We were able to debond her Symetri brackets in one piece without them shattering, which was incredibly convenient for us and our patient (Figure 7). The patient was referred to an oral surgeon for the extraction of her lower third molars (Figure 6).


Conclusion/critiques
I consider this case a success because we were able to achieve our goal of camouflaging the mild skeletal Class III malocclusion by obtaining Class I molars, correcting the anterior crossbite, and obtaining positive overjet. The patient was in treatment for 19 months, which in my opinion, was good enough to reach our goals and not have the patient in treatment any longer than she wanted to be. She was originally quoted a 22-24 month time frame so she was happy to be done in 19 months.
Although I’m thrilled with the outcome of this case, there are a couple of things that could have been done better. The occlusion on the right side could have been settled more, and her midlines aren’t optimally coordinated. I think a little more time with elastics could have corrected this, but the patient was delighted with the progress and was ready to complete treatment. In addition, more facial root torque of tooth No. 6 was needed, and gingival contouring from teeth Nos. 6-11 would’ve benefited the esthetics of the case, but she declined.
The many challenges to treatment sometimes are based in patient perception on esthetics. Read a study called, “The perception of orthodontists and laypeople on the esthetics of teeth treated with Icon® resin infiltration for the resolution of white spot lesions after the removal of fixed orthodontic appliances” for a discussion of treatment of white-spot lesions.
 Originally from Decatur, Georgia, Bryan Lockhart, DDS, attended the University of North Carolina at Chapel Hill for dental school. He attended a 1-year General Practice Residency at Montefiore Medical Center in New York before obtaining his Certificate in Orthodontics from Jacksonville University in Jacksonville, Florida. Dr. Lockhart furthered his learning by attending Jacobi Medical Center for an Orthodontic/Orthognathic Surgical Fellowship. Dr. Lockhart is well versed in fixed appliances as well as clear aligners and has developed his own clear aligner brand, Dualine. Dr. Lockhart is a member of SAO, AAO, and is board-certified with the American Board of Orthodontists (ABO). He has two orthodontic offices in Charlotte, North Carolina, where he practices with his wife, Dr. Lauren Lockhart.
Originally from Decatur, Georgia, Bryan Lockhart, DDS, attended the University of North Carolina at Chapel Hill for dental school. He attended a 1-year General Practice Residency at Montefiore Medical Center in New York before obtaining his Certificate in Orthodontics from Jacksonville University in Jacksonville, Florida. Dr. Lockhart furthered his learning by attending Jacobi Medical Center for an Orthodontic/Orthognathic Surgical Fellowship. Dr. Lockhart is well versed in fixed appliances as well as clear aligners and has developed his own clear aligner brand, Dualine. Dr. Lockhart is a member of SAO, AAO, and is board-certified with the American Board of Orthodontists (ABO). He has two orthodontic offices in Charlotte, North Carolina, where he practices with his wife, Dr. Lauren Lockhart.
Disclosure: Dr. Lockhart has no financial conflicts of interest in this article.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
