Dr. Bruce Goldstein discusses how SureSmile® technology provides the practitioner with tools to treat patients with greater efficiency and accuracy
3D imaging has become a very popular diagnostic aid in the orthodontic profession. This technology has allowed us to accurately visualize teeth and their relationship to the surrounding bone. Visualization is only part of the equation: The real benefit is to be able to use these diagnostic aids to help guide treatment.


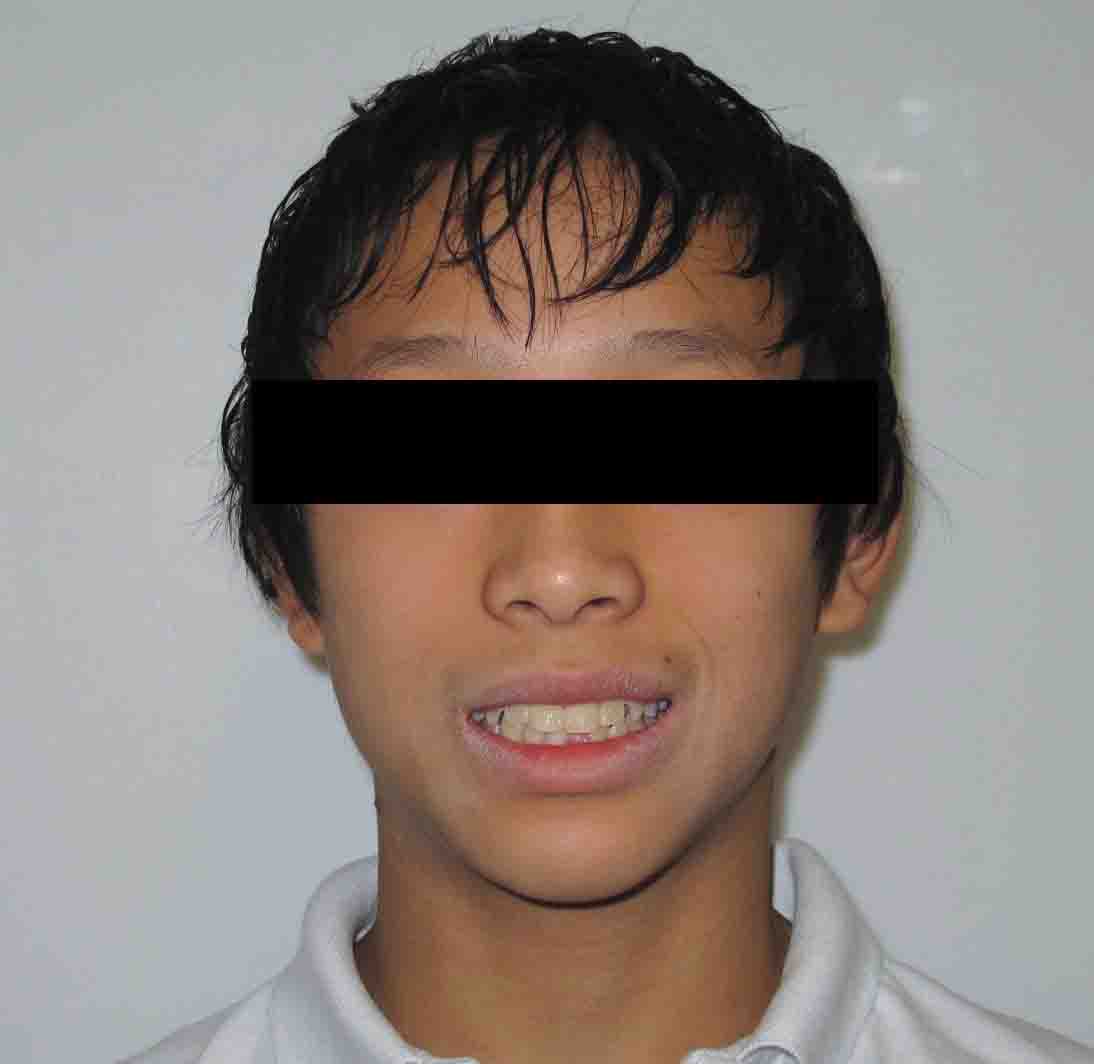
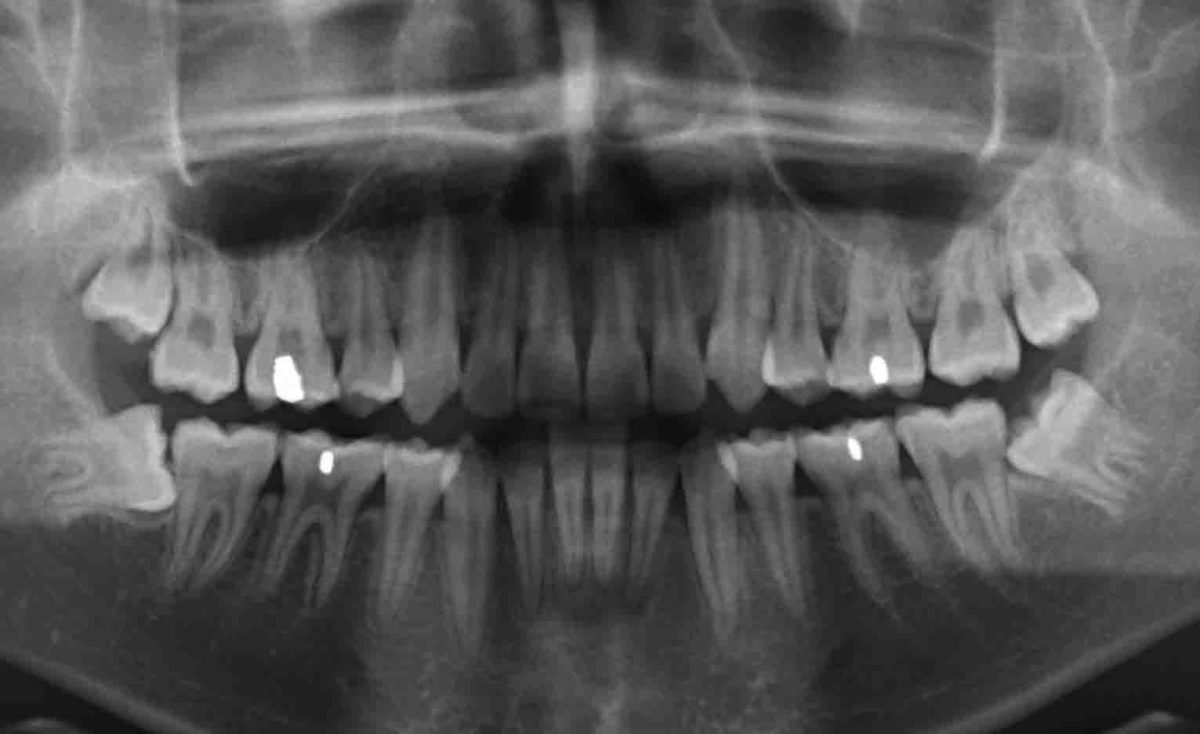
Figure 1

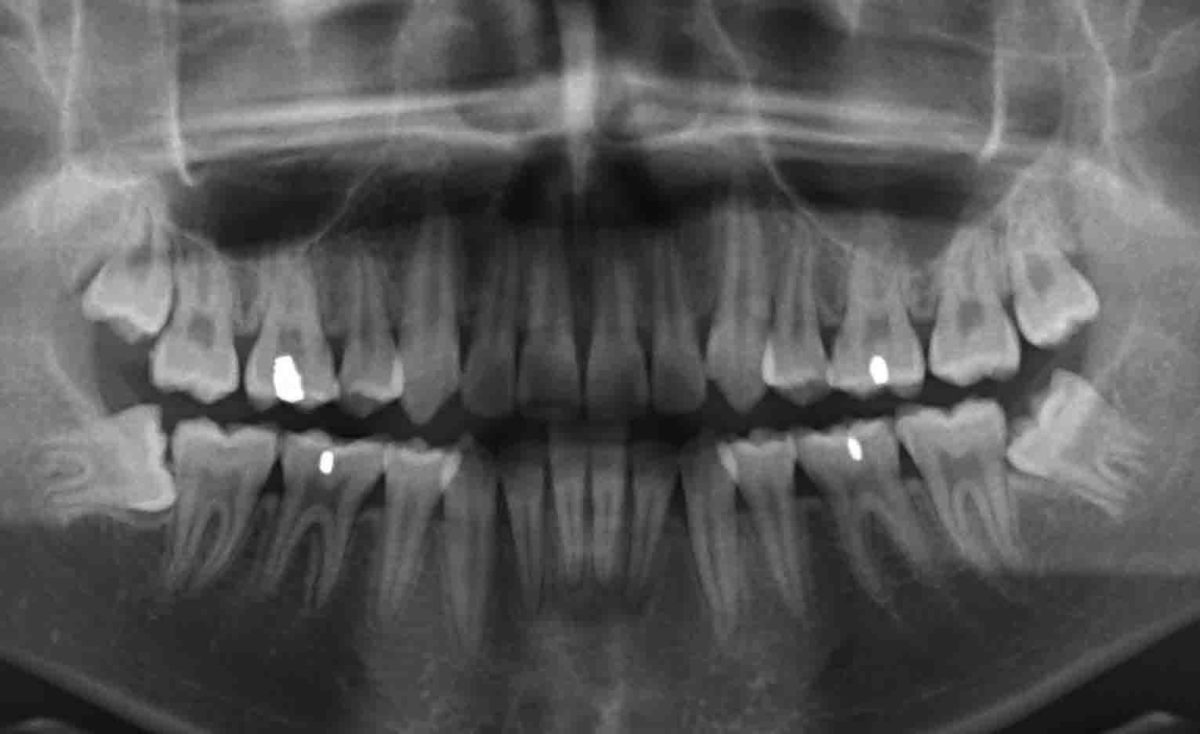

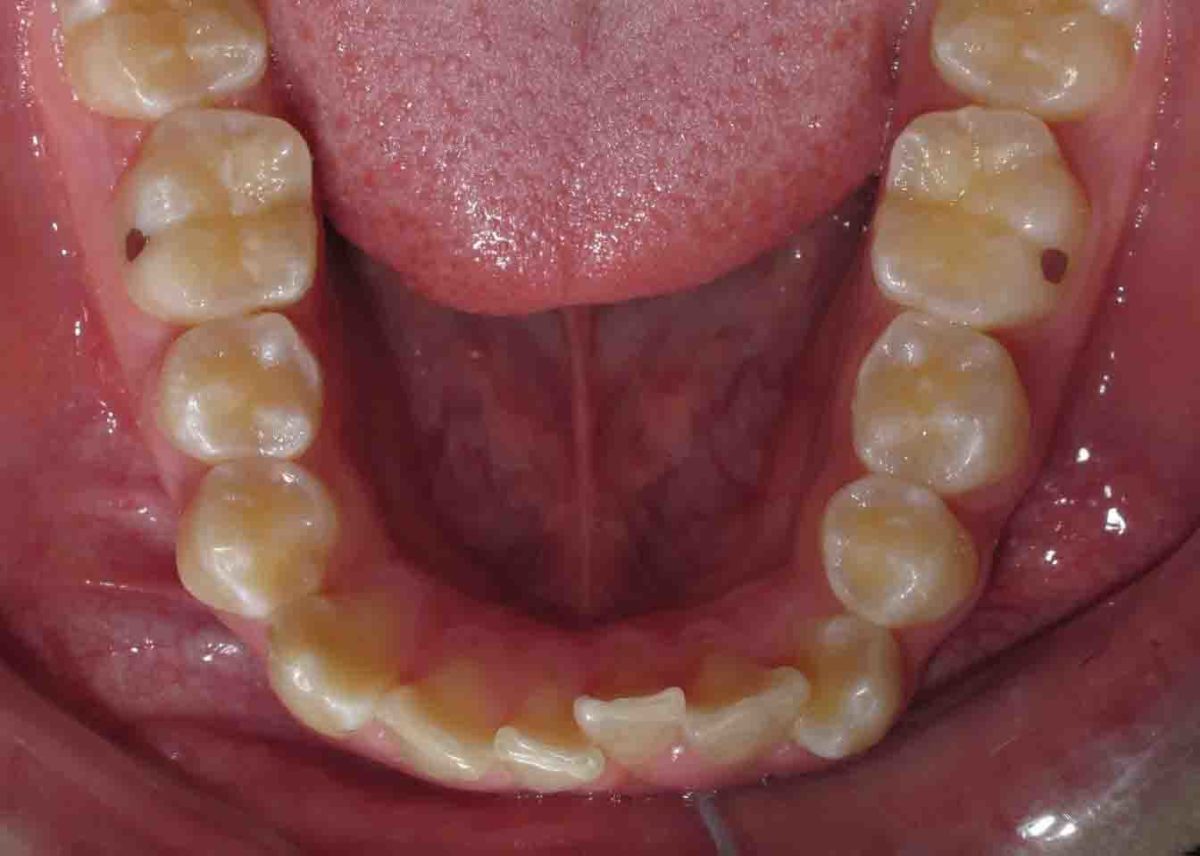



Figure 2: Pretreatment records
SureSmile® is the only comprehensive system that blends the best diagnostics available with accurately prescribed therapeutics. SureSmile technology provides the practitioner with the tools needed to treat patients with greater efficiency and accuracy.
Patient KD will serve as an example of how 3D imaging, along with SureSmile technology, can improve treatment results for our patients.
More accurate diagnosis. Better treatment results.
Initial observations
Patient KD, a 14-year-old male, presented with a Class I bimaxillary protrusive malocclusion (Figure 1). He had severe lower crowding, a maxillary cant, and lip incompetence. Third molars were impacted, and gingival tissue on the lower anteriors was very thin.
Treatment
A discussion with the patient and parent regarding treatment options was performed at a consultation (Figure 2):
- Option 1: Extract first bicuspids, eliminate crowding, and reduce dental protrusion.
- Option 2: Attempt non-extraction treatment and reevaluate after initial leveling and alignment were achieved.
A decision was made to attempt non-extraction treatment and reevaluate in 4 months. Extraction of third molars was recommended. The decision was made to wait until after active treatment was completed.
February 2011
Full fixed appliances were placed with bands on the upper second molars and the lower first molars. Bonded .022 MBT brackets (Unitek) were placed on all remaining teeth. Also, .016 NiTi wires were placed to allow for initial leveling and alignment.
April 2011
Copper NiTi wires (17 x 25) were placed to allow for proper leveling.



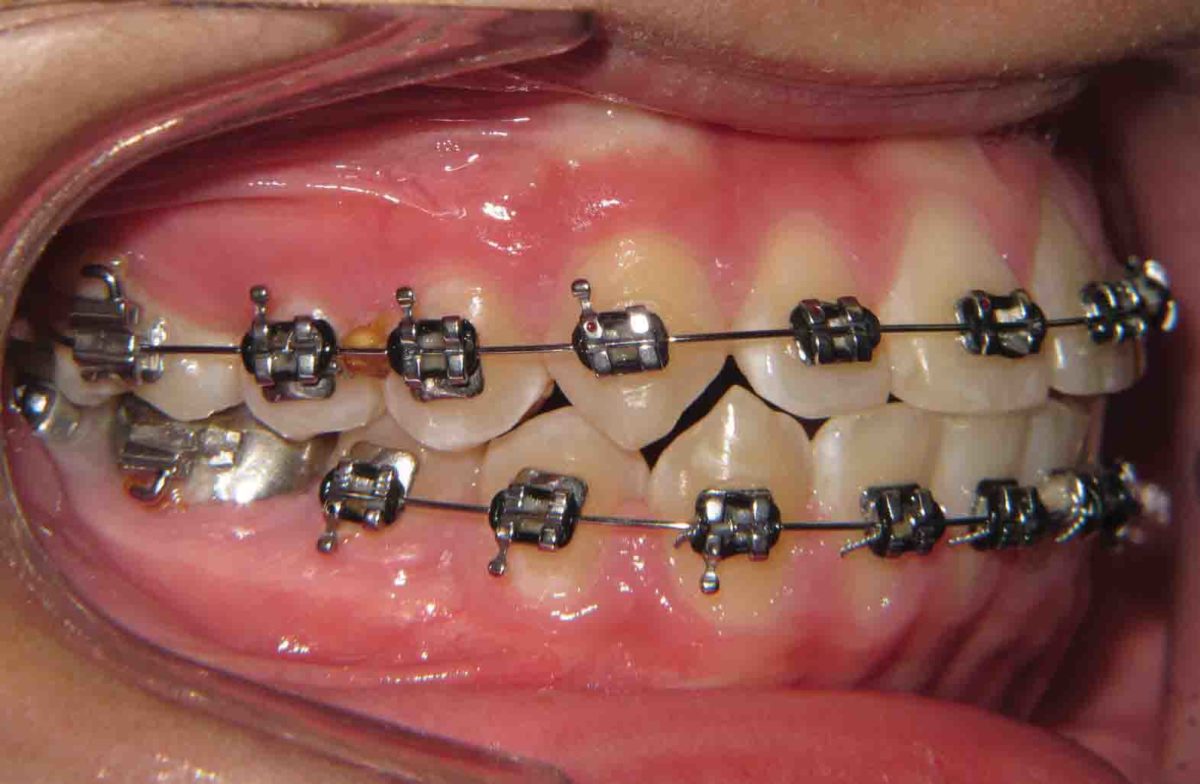
Figure 3





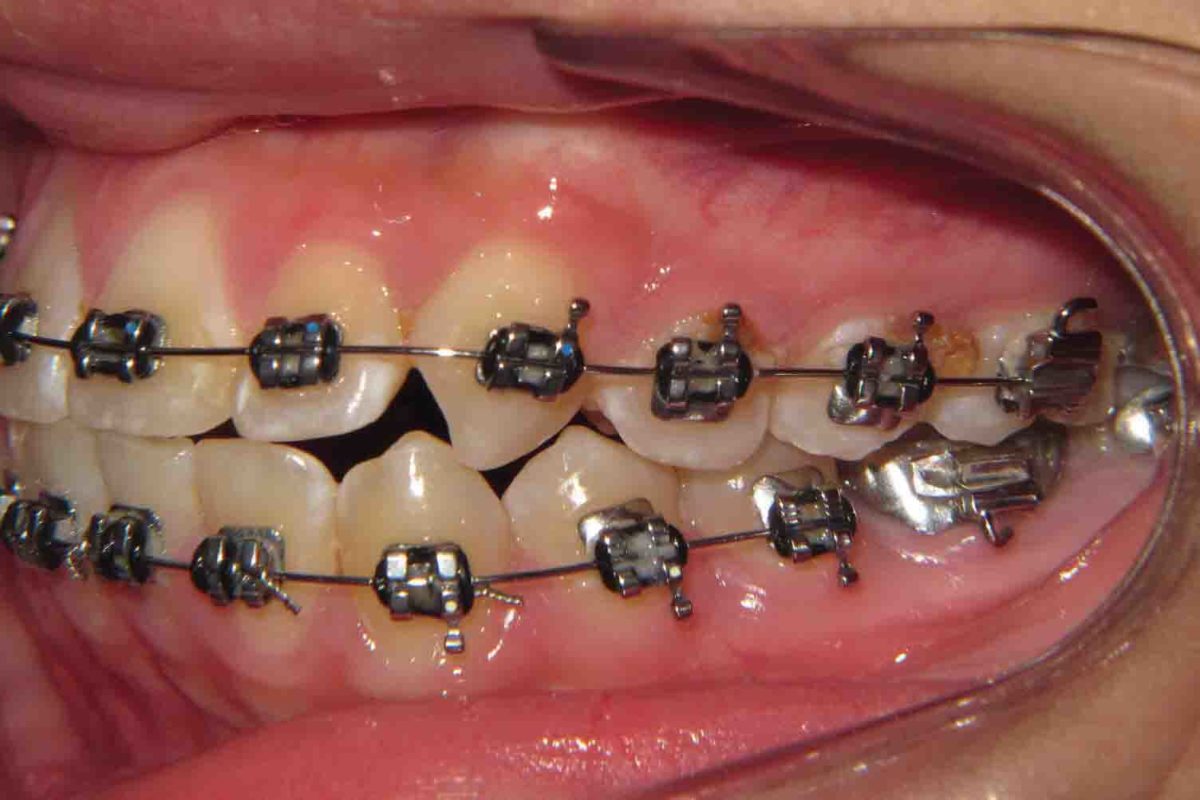
June 2011
Progress records were taken. This included a new cephalometric radiograph along with new photographs. After tracing the lateral ceph, it was obvious that the upper and lower anteriors were proclined. After a discussion with the parent, a decision was made to extract the four first bicuspids. Our goal was to reduce lip strain and the dental protrusion. Wires were removed, and a treatment request was sent to the oral surgeon (Figure 4).
July 2011
After extractions were performed, Patient KD presented. An .018 stainless steel wire, with stops mesial to the upper first molars, was inserted. A power chain was placed from the upper cuspids to the upper first molars to start retracting the cuspids. A round wire was used to allow for easier sliding mechanics, and a stop was placed for anchorage purposes. A 17 x 25 TMA lower archwire was inserted. We laced the lower 3-3 together with ligature wire. A power chain was placed from lower 3-5 to help protract lower posterior teeth.
September 2011
A 19 x 25 TMA closing loop archwire was inserted on the upper arch. A gable bend was placed distal to the upper lateral incisors. This was to be used to maintain torque control on the upper anterior teeth as space closure was completed. The closing loop archwire was activated, and power chain was placed from the upper cuspids to the upper molars. The lower archwire stayed intact, but a new power chain from the lower cuspids to the lower molars were placed. Class II elastics (¼”, 4 ½ oz.) were started. The elastics were used to help with anchorage.
November 2011
The upper closing loop archwire was activated. Reverse curve of Spee was developed into the lower archwire. Power chain from lower cuspids to the lower molars were replaced. Class II elastics were continued at nighttime only.


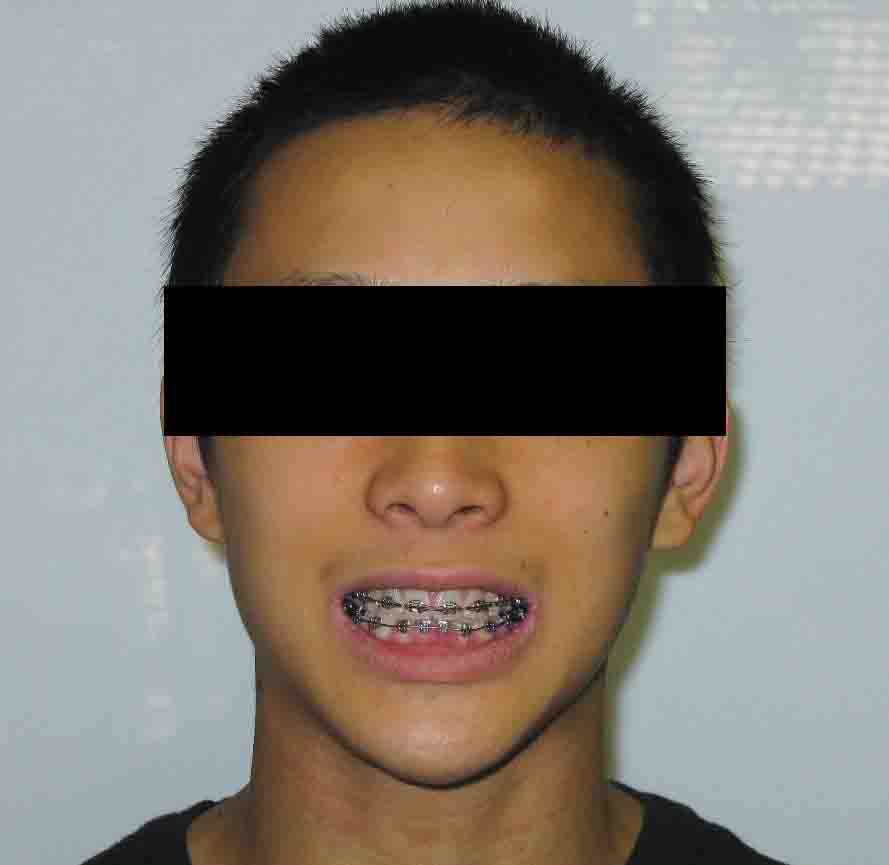
Figure 5

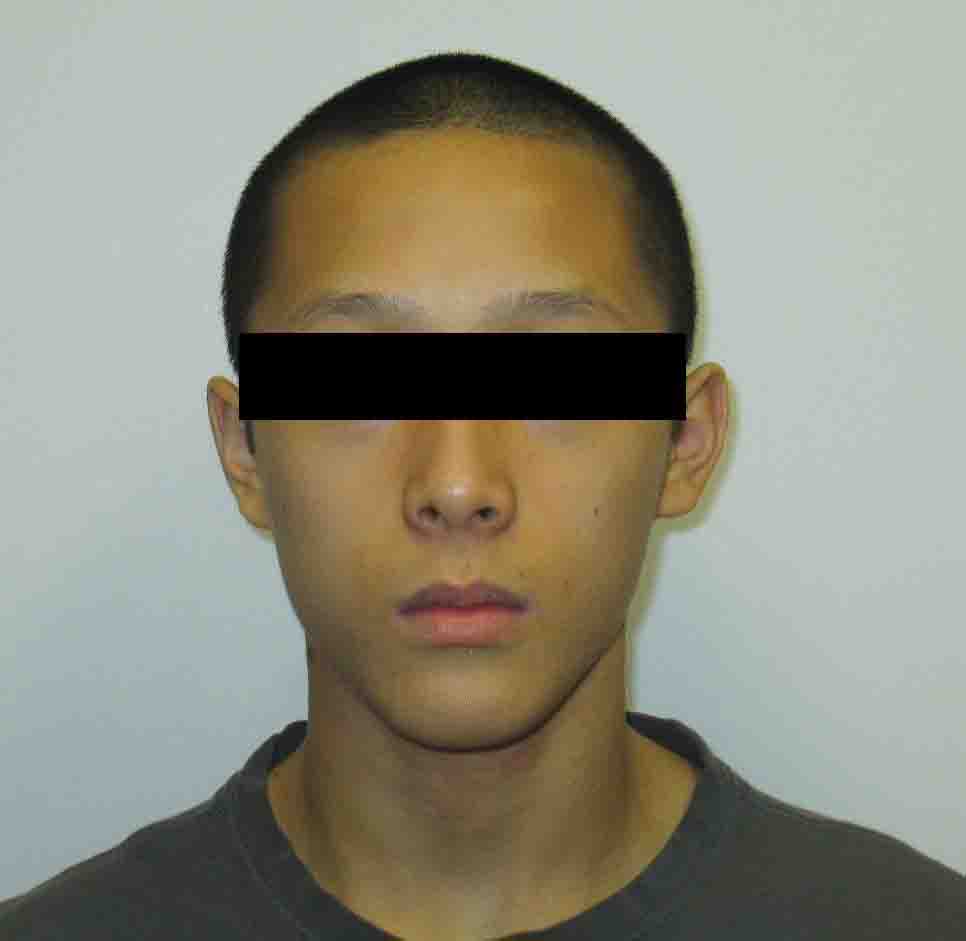
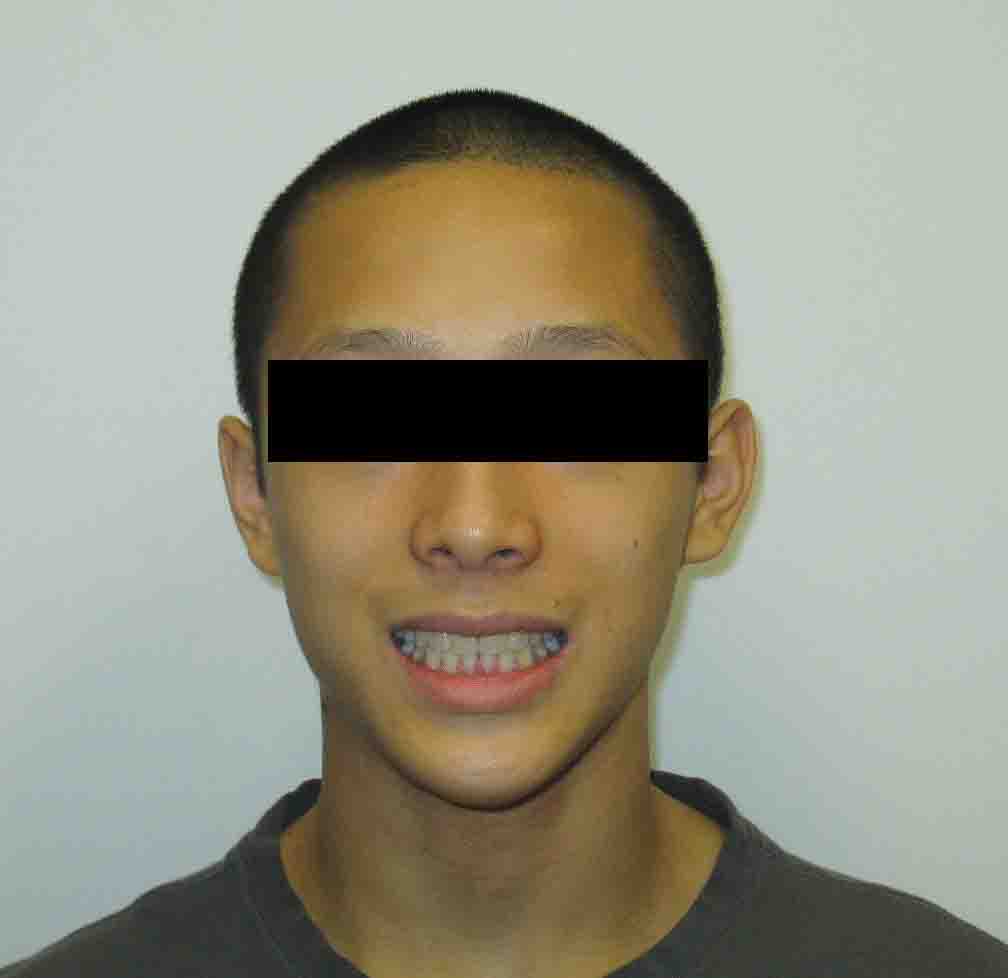
Figure 6
January 2012
The upper closing loop archwire was activated. The lower wire was retied. Nighttime elastics were continued.
March 2012
Treatment progressed as planned. New records, including photographs and a CBCT scan (SureSmile) were obtained. The photographs showed that the posterior occlusion was developing as planned. No signs of periodontal recession were noted. The CBCT scan data was electronically sent to Orametrix to convert the data into a virtual therapeutic model. The model revealed significant thinning of the bone around the maxillary cuspids and the lingual of the lower incisors. These issues would not have been exposed using traditional diagnostics.
A therapeutic setup was performed to position teeth in the most ideal functional and esthetic position possible. This included placing the roots of the upper cuspid and lower incisor teeth into the proper relation with the supporting alveolar bone. After obtaining the setup, robotically-bent archwires were displayed for my review. SureSmile provided us with the ability to “read the wire.” By superimposing the archwire over the brackets, we were able to evaluate how the wire will move teeth. After my approval, archwires were fabricated to align teeth into the prescribed position. Appropriate torque and angulation were built into the archwires to help achieve the desired results. The ability to visualize where the roots should be placed, and the ability to move them into the proper position enhanced our treatment results (Figure 7).


Figures 7A-7F: Records taken at SureSmile scan. E. Therapeutic model. F. Final treatment plan — setup complete
May 2012
SureSmile wire placement
We placed, and fully engaged, upper and lower 19 x 25 copper NiTi SureSmile wires that were custom-bent using SureSmile’s robotic technology. These wires were based on our virtual plan and conformed perfectly to our prescription.
July 2012
Modification appointment
We confirmed that the movement from the wires placed 8 weeks earlier had fully expressed. A clinical exam along with photographs were used to evaluate the need for any modifications required to finish treatment. Adjustments were made to the first set of SureSmile archwires, and new wires were fabricated. We re-tied the archwires and scheduled KD’s next visit (Figure 8).


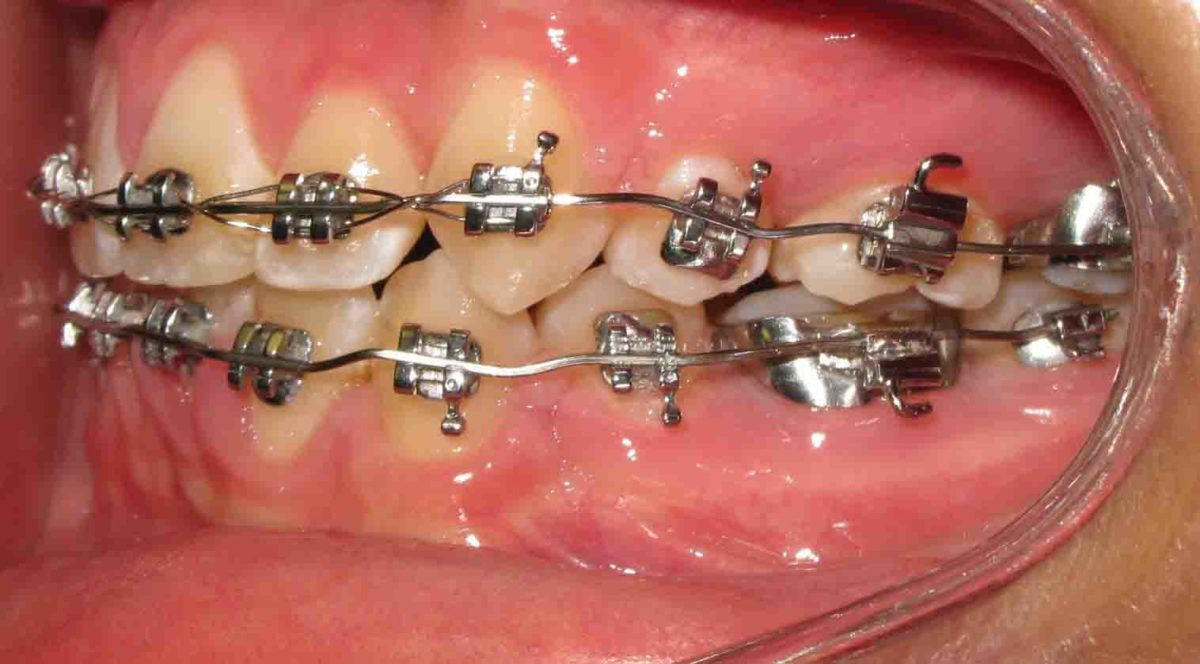
Figure 8: Progress photos taken for modification of the SureSmile archwires
August 2012
Modified wires placed
New 19 x 25 SureSmile copper NiTi wires were placed.
October 2012
We performed a check for deband appointment and then retied the archwires.
November 2012
We removed patient KD’s appliances and placed a mandibular fixed retainer from bicuspid-to-bicuspid. A maxillary Essix retainer was delivered at the same appointment. Patient KD was asked to wear the upper Essix retainer for 12 hours per day (Figure 9).





Figure 9: Final records
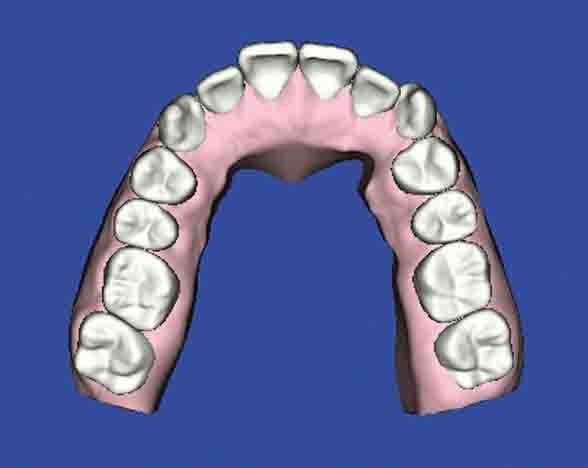
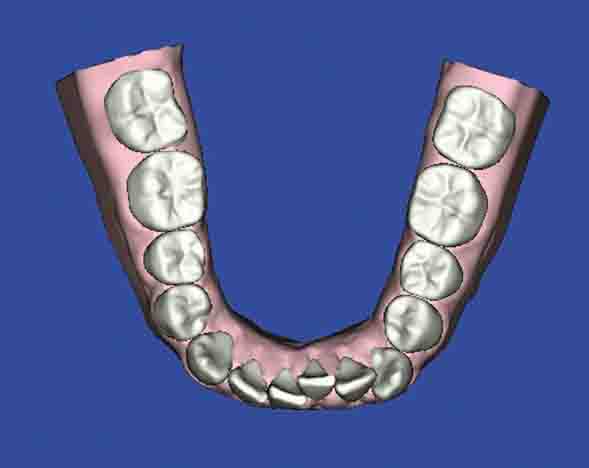
Figure 10: Initial patient model and Figure Figure 11: Initial patient model
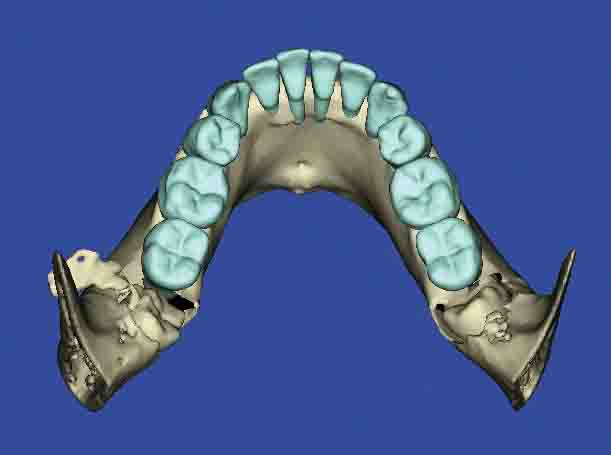
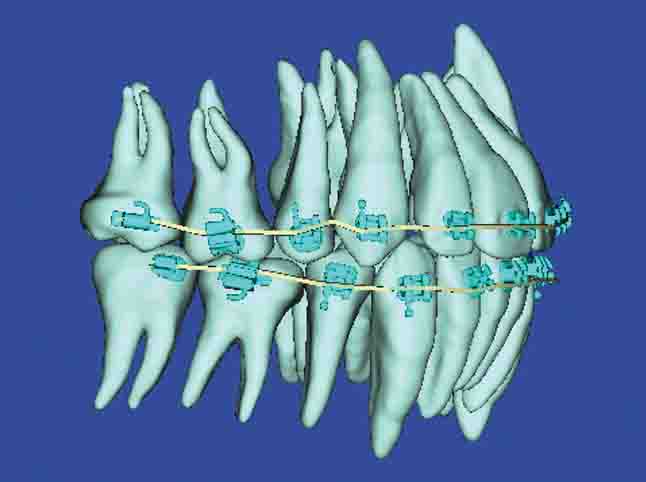
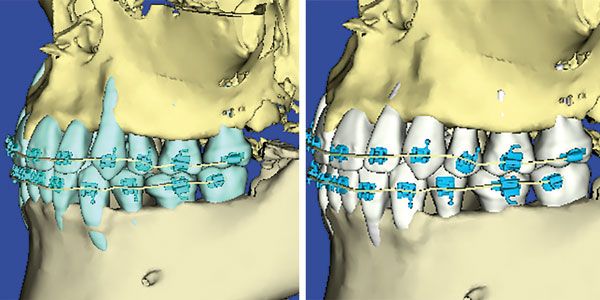
Figure 12: Lower incisor bone-level therapeutic scan and Figure 13: Read the wire. Note the medial inclination of the second bicuspid

Figure 14: Final patient right buccal — second bicuspid inclination corrected
Conclusion
Treatment for patient KD took 21 months. His cooperation was outstanding, which made our treatment progress as planned. The first 5 months of treatment were used in attempting a non-extraction approach. After extraction of the bicuspids, treatment became more efficient. Using SureSmile technology, it took us approximately 10 months to close spaces and 6 months to finish. Had we extracted initially, treatment would have been completed in approximately 16 months.
It is interesting to note that SureSmile treatment is often associated with faster treatment, but it would really be more accurately characterized as the most efficient orthodontic modality available to the profession. It is not just about speed; it’s about achieving the optimal result. SureSmile treatment helps me to “just do the right thing” for our patients.
The ability to use technology to help us achieve superior results for our patients is what SureSmile is all about. Being able to see potential problems and having a mechanism for dealing with these problems is what separates SureSmile from any other treatment modality. With patient KD, we saw how the thin bone around the upper cuspids and lower incisors would have gone unnoticed with conventional diagnostics. More importantly, we had the ability with SureSmile therapeutics to focus our mechanics on reducing these problems.
Summary benefits of SureSmile:
- The ability to provide exceptional therapeutics based on 3D imaging.
- Allows maximum control of individual tooth movement which significantly improves treatment efficiency.
- Better Treatment = Better Health.
A concluding thought
The question is: “How are you going to get teeth where you want them to be?”
The answer is SureSmile.
This article was originally published in SureSmile Clinical Report newsletter.
 Bruce Goldstein, DDS, MS, is a Diplomate, American Board of Orthodontics, who practices in Scottsdale, Arizona. Dr. Goldstein received his dental degree, Master’s degree, and Certificate in Orthodontics from the State University of New York at Buffalo. He was a clinical instructor, Department of Orthodontics at A.T. Still University. He is President Elect of the College of Diplomates of the American Board of Orthodontics. He started offering SureSmile treatment in October 2006 and has completed more than 4,000 cases.
Bruce Goldstein, DDS, MS, is a Diplomate, American Board of Orthodontics, who practices in Scottsdale, Arizona. Dr. Goldstein received his dental degree, Master’s degree, and Certificate in Orthodontics from the State University of New York at Buffalo. He was a clinical instructor, Department of Orthodontics at A.T. Still University. He is President Elect of the College of Diplomates of the American Board of Orthodontics. He started offering SureSmile treatment in October 2006 and has completed more than 4,000 cases.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
