Drs. Pat Brady, Carina Dabney, and Hilton Israelson helped a patient uncover her smile through orthodontics
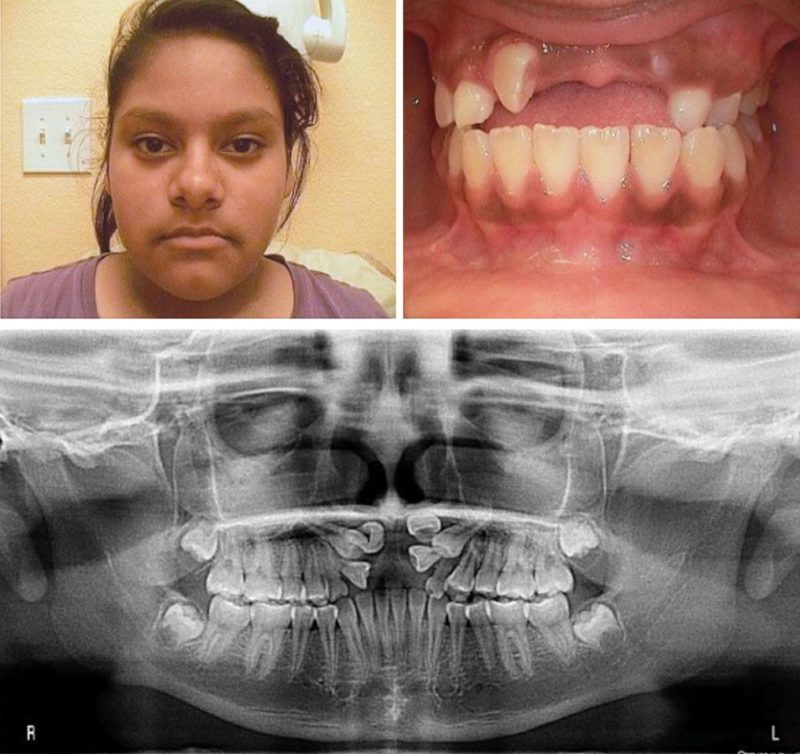 Figure 1: Initial photos and panoramic X-ray
Figure 1: Initial photos and panoramic X-ray
On August 20, 2014, a 13-year-old patient presented to our office for orthodontic treatment with this chief complaint: “I don’t want to smile because I don’t have any front teeth.” Her mother further confided that her daughter’s education has been severely impeded as she refused to attend school because of her appearance. The initial examination revealed a Class I posterior occlusion, and teeth Nos. 6, 8, 9, 10, and 11 were impacted, while No. 7 was partially erupted and lying parallel to the floor of the nose (Figure 1).
The treatment plan called for the exposure and bonding of attachments to all of the impacted teeth and bonding the remaining teeth in the maxillary and mandibular arches. Initially, the plan was to use distraction osteogenesis to advance the maxilla and hopefully stimulate growth of alveoli for the impacted teeth. Such surgical distraction proved unnecessary, however, as treatment progressed. Simply uncovering, extrusion, and advancing the teeth with their alveoli eventually provided the much needed support for the upper lip.
A CT scan provided both orthodontist and oral surgeon enough additional data to formulate an eruption plan for the impacted teeth. The surgeon channeled the bone to expedite the eruption of each impacted tooth, while the forced eruption of the exposed teeth was achieved by using as anchorage the inner bow of a maxillary headgear appliance from which the outer bows were removed. The inner bow fitted into the headgear tubes of the molar bands and was tied in place with ligature wires. The anterior part of the adapted headgear bow was notched to accommodate elastic threads that tied to the uncovered, impacted teeth. A continuous edgewise maxillary arch wire consolidated the rest of the maxillary dentition to minimize reciprocal effects from the extrusion of the impacted teeth (Figure 2).

Figure 2: Modified headgear inner bow and exposed impacted teeth
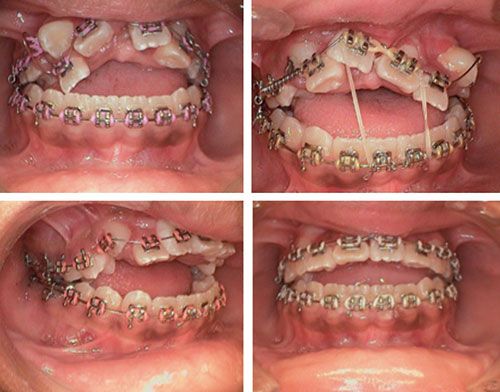
Figure 3: Exposed teeth erupted enough to receive brackets
As treatment progressed and the teeth continued to erupt, brackets were added allowing more control. At this time tooth No. 8 was now discovered to be rotated 180° and possessed a dilacerated root. It was decided by mutual agreement between the orthodontist and oral surgeon to leave the tooth in its unrotated position (Figure 3).
As the teeth erupted, the headgear bow was advanced downward and forward. The headgear bow was discarded once the teeth had sufficiently erupted to use anterior box elastics to the maxillary and mandibular incisors. A vertical elastic was applied to the impacted maxillary canine to aid its eruption. As soon as the maxillary arch had been aligned, anterior box elastics were used to close the bite.
At this point, the patient was referred to a periodontist for sulcus deepening amid concerns regarding the attached gingiva over the maxillary central incisors. Once the periodontal tissue had stabilized, the ortho-dontic therapy was completed, and tooth No. 8, which remained unrotated, was reconstructed by filling in the lingual surface of the tooth with composite to give the appearance of a normal incisor facial surface (Figure 4).

Figure 4: Treatment outcome photographs. Note the temporarily composite-augmented lingual surface of the maxillary left
central incisor that awaits further periodontal and cosmetic intervention
On February 1, 2017, after a period of 2 years and 6 months, treatment was completed, and the patient no longer hesitates to smile, and she attends school regularly. In addition to its general dentists and specialty teams, Bear Creek Family Dentistry of Dallas, Texas, donated their staff, facilities, and services to make this treatment possible.
 Pat Brady, DDS, MS, has more than 40 years of experience as an orthodontist. He is a past president of the Greater Dallas Association of Orthodontists and has had academic appointments at the Baylor College of Dentistry and UT Southwestern School of Medicine. He is a former Captain of the United States Air Force and is certified by the American Board of Orthodontics. Dr. Brady also did original research on nitinol wire.
Pat Brady, DDS, MS, has more than 40 years of experience as an orthodontist. He is a past president of the Greater Dallas Association of Orthodontists and has had academic appointments at the Baylor College of Dentistry and UT Southwestern School of Medicine. He is a former Captain of the United States Air Force and is certified by the American Board of Orthodontics. Dr. Brady also did original research on nitinol wire.
 Carina Lynn Schwartz-Dabney, DDS, MD, PhD, has 14 years of experience as an oral surgeon. Dr. Dabney’s practice includes extractions, pre-prosthetic services, biopsies, expose and bond, frenectomies, orthodontic anchorage, bone grafts, and implants. Dr. Dabney attended both the University of Dallas, Irving, and the University of Illinois, Champagne-Urbana, before earning her Doctor of Dental Surgery degree from Baylor College of Dentistry in 1993 and her PhD in Craniofacial Biology in 2001. Dr. Dabney has previously served as an assistant professor at the University of Texas Southwestern Medical School. Her current professional memberships include the AAOMS, North Texas Society of Oral and Maxillofacial Surgeons, Texas Society of Oral and Maxillofacial Surgeons, Omicron Kappa Upsilon, and Tripartite ADA, TDA, and Dallas County Dental Society. Dr. Dabney has also been published in numerous books and journals.
Carina Lynn Schwartz-Dabney, DDS, MD, PhD, has 14 years of experience as an oral surgeon. Dr. Dabney’s practice includes extractions, pre-prosthetic services, biopsies, expose and bond, frenectomies, orthodontic anchorage, bone grafts, and implants. Dr. Dabney attended both the University of Dallas, Irving, and the University of Illinois, Champagne-Urbana, before earning her Doctor of Dental Surgery degree from Baylor College of Dentistry in 1993 and her PhD in Craniofacial Biology in 2001. Dr. Dabney has previously served as an assistant professor at the University of Texas Southwestern Medical School. Her current professional memberships include the AAOMS, North Texas Society of Oral and Maxillofacial Surgeons, Texas Society of Oral and Maxillofacial Surgeons, Omicron Kappa Upsilon, and Tripartite ADA, TDA, and Dallas County Dental Society. Dr. Dabney has also been published in numerous books and journals.
 Hilton Israelson, DDS, MS, is a periodontist who specializes in treating the soft tissues and bone surrounding the teeth and in placing dental implants. In addition to private practice, he has been an educator to other dentists for over 40 years and has participated in numerous periodontal research studies. He is a Diplomate of the American Board of Periodontology, the highest status awarded to a periodontist for knowledge and clinical expertise. A native of South Africa, Dr. Israelson received his degree as a general dentist in 1973 from the University of the Witwatersand, Johannesburg, School of Oral Health Sciences. He then came to the United States for his periodontal specialist training and residency and graduated from Tufts University School of Dental Medicine in Boston with a certificate in periodontology.
Hilton Israelson, DDS, MS, is a periodontist who specializes in treating the soft tissues and bone surrounding the teeth and in placing dental implants. In addition to private practice, he has been an educator to other dentists for over 40 years and has participated in numerous periodontal research studies. He is a Diplomate of the American Board of Periodontology, the highest status awarded to a periodontist for knowledge and clinical expertise. A native of South Africa, Dr. Israelson received his degree as a general dentist in 1973 from the University of the Witwatersand, Johannesburg, School of Oral Health Sciences. He then came to the United States for his periodontal specialist training and residency and graduated from Tufts University School of Dental Medicine in Boston with a certificate in periodontology.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
