Dr. Ron Roncone discusses using Roncone PDS to have fewer appointments and shorter treatment time
What if an orthodontist were to observe the same phenomenon several thousand times?
The Same Input = The Same Output
Would this be clinically significant?
[userloggedin]
If these observations could not be found in the literature, would they be invalid?
Would we NOT be practicing evidence-based orthodontics?
I would like to mention just seven of the many observations I have made in 44 years of orthodontic practice. The vast majority have occurred since 1981. Since that time, I have taken tomographs or CBCT on “almost” every patient. I have taken frontal cephs (or CBCT) on “almost” every patient. Except for a 1½-year period (1976-1978), I have articulated all starts and all finished cases. I have treated more than 35,000 patients since 1974.
Observation 1
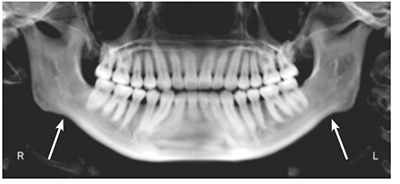
Antegonial notching of the mandible is evidence that there has been a long-term (years) hypertonicity of the masseter and medial pterygoid muscles (Figure 1).
This will impede timely orthodontic treatment at best or cause failure at worst. Easy cases turn into difficult ones.
What to do?
Initiate at least 6 weeks of full-time splint therapy along with the use of ultrasound and ethyl chloride spray before orthodontics begins. Turbos on maxillary central incisors must be used as part of the treatment plan to keep muscles relaxed and avoid posterior tooth contact.
Observation 2

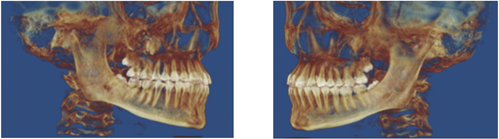
Close approximation of cervical vertebrae on the dorsal surface almost always indicates that the mandible is in a forward position to achieve maximum occlusion. Since the average person swallows between 1,700 and 2,400 times a day, this maximum intercuspation is easier to achieve with the head in a forward position. The true occlusion is either more Class II then we see or more Class III (Figure 2).
What to do?
If the mandible can easily be hinged to a first contact position, begin orthodontics with turbos or a banded Nance bite plate to unlock occlusion.
If the mandible is not easily hinged to first contact — splint and physical therapy (PT) modalities for 6-8 weeks.
This forward head position has NOTHING to do with lack of airway. With the advent of CBCT and good health history, you can be sure it is not an airway problem.
Observation 3

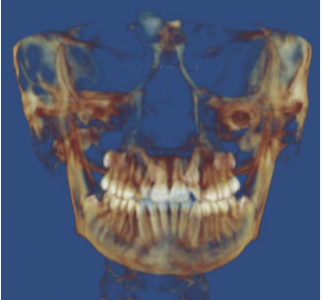
A significant majority of patients have a maxillary frontal asymmetry. This causes the mandible to grow asymmetrically as well. This causes joint problems, muscle problems, and esthetic problems. We have all seen and treated uncorrected maxillary asymmetries. We have all seen the uncomplimentary smiles where more gingival tissue is seen on one side of the arch than the opposite side — even though the teeth meet correctly (Figure 3).
What to do?
Place a fixed Hyrax appliance, and expand. Continue two forward turns, alternating with two backward turns for at least 6 weeks. These turns are alternated on consecutive days. The continuous swallowing (1,700 – 2,400 times daily) will assist in “leveling” the maxilla. I have observed this phenomenon for more than 35 years.
Observation 4
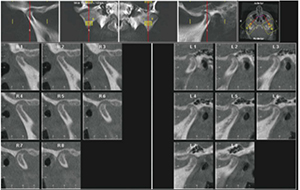
Just under 30% of children between the ages of 10 and 16 have some evidence of condylar degenerative joint disease (DJD). Most of this does not coincide with past trauma. This is why I have taken tomograms and now CBCT on almost every patient we see. Most of these young people are asymptomatic (Figure 4).
The joints shown in Figure 4 are from a 15-year-old who came in for aligner treatment.
What to do?
Take CBCT on all patients. You never know.
Observation 5
I have placed two wires initially since 1971. Since 1987, my initial wires have been .014 NiTi fully engaged with steel ligatures and then active self-ligating brackets. We see the patient at 12 weeks for a check and then reschedule him/her for another 12 weeks. If turbos are routinely used, alignment and rotations are corrected (usually 8-10 weeks), archform is complete, Curve of Spee is corrected, and molars are derotated, correcting a large number of Class IIs, and any nonparallel roots are mostly parallel.

The force of twin wires is minimal, if a tooth is significantly malaligned. Then only one of the wires is engaged initially. The other wire is engaged at the 12-week appointment. Teeth move rapidly, and discomfort is minimal (4 out of 10) when patients were asked pain levels. This was asked of each full-bonded patient over a more than 8-year period (Figure 5).
Figure 6 shows the same patient after a little over 5 months, when a rectangular wire was placed in each arch.
Appointments have been reduced significantly, and root resorption is virtually not seen. The friction or binding that we have been told to be worried about plays no part in rate of tooth movement.
What to do?
Routinely use two .014 NiTi superelastic wires initially.
Observation 6
Where it is applicable, use anterior turbos made of clear Triad® material. Why are they so important? There are a number of reasons:
- The posterior teeth do not meet, so the Curve of Spee is corrected permanently in most cases. I keep turbos on for at least 10 months. This allows the lower posterior teeth to erupt quickly, but more importantly, bone fills in at the apices of these teeth. If the posterior teeth come together 2,000 times a day, there can be no bony fill, thus causing the Curve of Spee to eventually return.
- Since the teeth do not meet in the posterior, premolar and molar brackets rarely fail.
- Since only lower incisors contact the turbos, teeth move more quickly.
- There is no wear of teeth as they transition from Class II to Class I.
- Forces of occlusion are significantly diminished; therefore, muscles stay relaxed.
- The condyles stay “hinged” in an ideal position.
Observation 7
Over the years, I have attempted many options to bring in impacted canines. Most have been successful, but they took too much time — lengthened treatment time in order to make space for the canine first and then to expose the tooth, perhaps have it passively erupt, then move the tooth in multiple directions in order to get it into the arch. Since 1991, I have used one and only one method to bring in all impacted canines. These conditions must be present:
- The use of a molar tube with 20 degrees distal rotation and 20 degrees of torque — Roncone PDS anchorage molar
- A single-strand .018 HANT wire
- A gold chain attached to the impacted tooth
In most cases, an open coil spring, etc., does not need to be used to open space.
Bringing in canines in the manner I will demonstrate in Case 1 and Case 2 has worked thus far for every patient whether labially or palatially impacted but one. The one patient commuted from the Midwest and had three other orthodontists involved who kept changing the protocol. That patient lost two teeth and needed implants.
What to do?
Case 1




What to do?
Case 2: Bilateral palatially impacted canines

There are many other observations that I believe are equally important, which this brief article does not allow. However, it might behoove orthodontists to add more weight to their observations rather than to blindly follow. The words of Nobel Prize Laureate Albert Szent-Györgyi may be appropriate:
“Discovery consists of seeing what everybody else has seen and thinking what nobody has thought.”
For more information about JSOP Courses, visit: https://www.forestadent.com/forestadent-us/Kurse/Programm/index.php?lang=us&term=xxv+session
For more details about the PDS Philosophy, visit: https://www.forestadent.com/forestadent-us/Produkte/products/PhysioDynamic.php?navanchor=10000
[/userloggedin]
[userloggedout][/userloggedout]
 Ronald Roncone, BA, DDS, MS, received his degrees in physiology from Marquette University and his postdoctoral Certificate in Orthodontics from Forsythe Dental Center and Harvard School of Dental Medicine. Dr. Roncone maintains a large practice in Vista, California, with 55% adult patients. Dr. Roncone has lectured extensively, presenting more than 1,000 seminars around the world, and is President and CEO of Roncone Orthodontics International®, which offers practice management courses as well as in-office consulting and marketing services.
Ronald Roncone, BA, DDS, MS, received his degrees in physiology from Marquette University and his postdoctoral Certificate in Orthodontics from Forsythe Dental Center and Harvard School of Dental Medicine. Dr. Roncone maintains a large practice in Vista, California, with 55% adult patients. Dr. Roncone has lectured extensively, presenting more than 1,000 seminars around the world, and is President and CEO of Roncone Orthodontics International®, which offers practice management courses as well as in-office consulting and marketing services.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
