Editor’s intro: Cervical-pull headgear can be cumbersome and inconvenient for patients. Dr. Jack Fisher achieved the headgear effect using skeletal anchorage devices.
Dr. Jack Fisher discusses a treatment alternative to headgear
Introduction
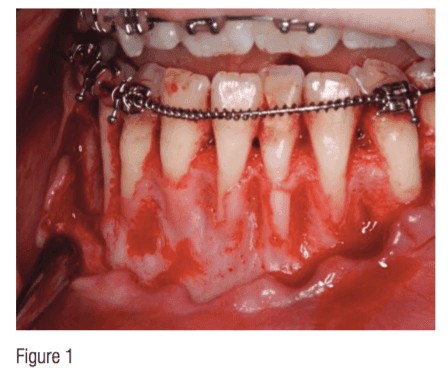 For many years, orthodontists have used cervical-pull headgear to treat Class II patients. However effective headgear can be, most patients hate the idea of wearing this appliance. This has led to an increase in the use of functional appliances as well as Class II corrector, all of which inevitably procline mandibular anterior teeth. After looking at many CBCTs, with particular interest in the alveolar boundaries of mandibular incisors, it is noted that often there is little-to-no bone into which to procline mandibular anterior teeth, which is one reason that gingival grafting is so common in adults who have had treatment when they were younger (Figure 1).
For many years, orthodontists have used cervical-pull headgear to treat Class II patients. However effective headgear can be, most patients hate the idea of wearing this appliance. This has led to an increase in the use of functional appliances as well as Class II corrector, all of which inevitably procline mandibular anterior teeth. After looking at many CBCTs, with particular interest in the alveolar boundaries of mandibular incisors, it is noted that often there is little-to-no bone into which to procline mandibular anterior teeth, which is one reason that gingival grafting is so common in adults who have had treatment when they were younger (Figure 1).
The perio/ortho relationship is now at the forefront of most orthodontic practices looking at CBCT as well as the potential need for augmentation of the mandibular anterior region, which is being discussed more frequently. In a Class II situation where clinicians want to maintain or improve the mandibular incisor angulation, they must depend upon growth as well as a distalization effect of the maxillary arch.
Case study
This case will look at a situation where a “24-hour headgear” was used. This treatment modality employs the use of skeletal anchorage devices to distalize the maxillary arch and to allow for mandibular growth to occur. In this case, a 12-year 8-month-old male presented with the chief complaint of “I have crooked teeth and an overbite” (Figure 2). His medical history was insignificant, and he had no previous orthodontic treatment. He presented with a mild Class II brachycephalic skeletal profile (ANB 4°) with mild maxillary prognathia (SNA 86°). Dentally, he presented with a Class I Division 1 incisor relationship. Midlines are coincident, and the mandibular left first molar was in buccal crossbite. He has 5 mm of overjet and 5 mm of overbite. The patient had mild crowding in the maxillary anterior and no crowding in the mandibular anterior. The curve of Spee is 2 mm, and the mandibular incisors were proclined (IMPA 106). He had a concave facial profile and an obtuse nasolabial angle. A TMJ exam revealed no joint sounds, and joints were asymptomatic. The patient had balanced maxillary and mandibular facial heights, and his lips were competent. He showed 100% of incisors upon smiling with 1 mm of gingival display and a concave facial profile with an obtuse nasal labial angle of 103°.

Radiographic analysis
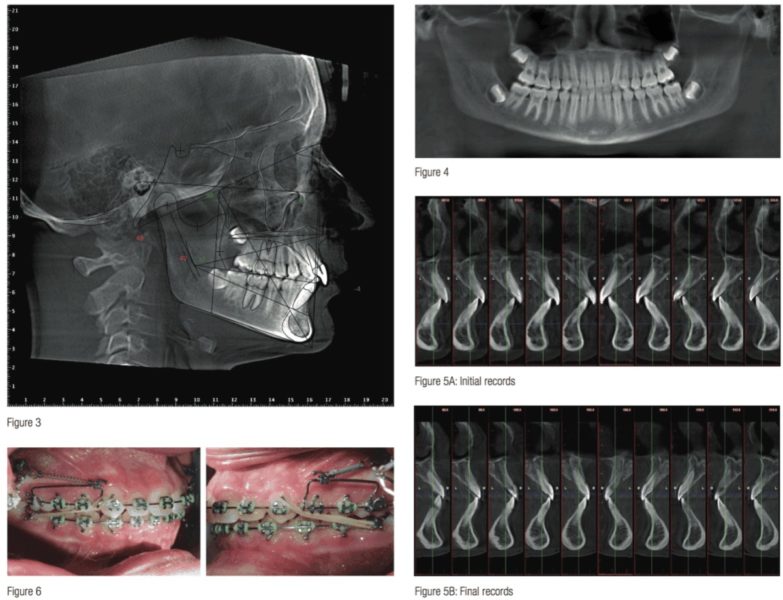
Once the patient exam had been completed, it was determined that a CBCT should be taken to evaluate bone dimensions for diagnostic purposes and to identify the best location for TSAD placement. CBCT analysis revealed limited alveolar boundaries on the buccal and lingual of the mandibular anterior teeth. The buccal and lingual cortical plates of the alveolar processes were generally thin, particularly around canines and mandibular anterior teeth (Figure 4). Thicker cortical regions were present palatal to maxillary incisors. Currently, the author is using the Planmeca ProMax® 3D Mid, which allows for an Ultra Low Dose™ CBCT Full Field Of View (FFOV) to be taken with less radiation (~15 microsieverts) than traditional 2D pan/ceph radiography.
A lateral cephalometric radiograph was reconstructed. Cephalometric analysis revealed a hypodivergent mild Class II skeletal pattern with well-balanced maxillary and mandibular facial heights, increased concavity, and moderately proclined mandibular incisors with maxillary incisors in a relatively normal position (Figure 3).
The panoramic radiograph was reconstructed from a CBCT. Panoramic analysis revealed no pathology, and third molars were developing normally.
Model analysis revealed a Class II molar relationship on the left and right with moderate overbite and overjet. The maxillary midline is coincident with facial midline, and the mandibular midline is coincident with the maxillary midline. The curve of Spee is moderate. Transversely, the mandibular left first molars and buccal crossbite.
Treatment objectives
The treatment objectives established were to maintain the transverse and vertical dimensions as well as A-point other than where normal growth would be concerned, as well as to reduce increased over jet and overbite while alleviating the crowding present. The treatment aimed to correct the Class II molar relationship to a Class I molar relationship and maintain coincident midlines. Treatment planned for improved facial profile and to allow for growth of the mandible to occur.
Treatment alternatives
Three treatment options were presented to the patient:
- Traditional headgear to restrain maxillary growth and to allow for mandibular growth to occur.
- Extract maxillary first premolars and close space.
- Place temporary skeletal anchorage devices to distalize/restrain the maxillary arch while allowing for mandibular growth.
Treatment plan/progression
The above treatment options were presented to the patient, and risks and benefits of each option were discussed. The patient opted for non-extraction treatment with placement of temporary skeletal anchorage devices to hold the maxillary arch during the peak adolescent growth phase allowing for a “headgear effect” to occur. The bracket prescription used was MBT. Maxillary archwires were progressed to a 20 stainless steel with cinch backs. It was at this time that the skeletal anchorage devices would placed and 200g springs used with sliding yokes bilaterally (Figure 6). This was left in place for 5 months until the Class II molar relationship was corrected. At this point, the mandibular arch was bracketed, and wires were progressed. Before moving to stainless steel in the mandibular arch, an Ultra Low Dose dental-only (LFOV) scan was taken to evaluate the roots and bracket placement after level and aligning had occurred prior to moving to stainless steel posted archwire with tie backs. The case was finished with a 16 x 16 heat active NiTi wires with common ties from canine to canine, 20 segmental stainless. The case was finished with vertical elastics in the pyramid configuration, and the case was finished as planned. The total treatment time was around 17 months. (Figure 7)

Cephalometric superimposition revealed that the maxillary molar position was relatively maintained with slight distalization, while the maxillary incisors were retracted bodily, slightly. In the mandibular arch, molar position was maintained, and the mandibular incisors were retroclined from 106° to 92° IMPA due to the coupling effect of the maxillary and mandibular incisors as a result of mandibular growth. Growth was a major factor in this case; both the vertical and sagittal dimensions revealed normal growth (Figures 8-10).
The case was evaluated for four first bicuspid extractions as well as headgear and/or the removal of only first bicuspids. The non-extraction treatment using skeletal anchorage to the maxillary arch was successful. This technique would not have been as successful in a dolichofacial skeletal pattern. The mandibular incisors retroclined unexpectedly. This occurred due to the strong muscle pattern and the horizontal growth pattern, which was very good.
Analysis of final records reveal that the posterior crossbite was eliminated. Class I occlusion was achieved, and mandibular incisor position was improved. Overjet and overbite were both reduced. Upon review of final records, the clinician can see the patient’s chief complaint has been resolved, and posterior crossbite has been alleviated. Critically speaking, I would say one of the major factors for success in this case was mandibular growth.
Besides the headgear effect, orthodontists are using other creative treatment therapies. Check out “An unusual orthodontic therapy,” by Drs. Pat Brady, Carina Dabney, and Hilton Israelson here.
 Jack Fisher, DMD, completed his orthodontic training at the Medical College of Georgia in 1982. Since then he has been in the full-time practice of orthodontics in Kentucky and Tennessee. He has lectured both in the United States and internationally. Dr. Fisher is a member of the Southern Association of Orthodontics and the American Association of Orthodontics. He is presently a faculty member in the orthodontic department at The University of Tennessee. Dr. Fisher has taught a 2-day cadaver course for the insertion and use of temporary skeletal anchorage devices for 8 years. He has written several articles on the use of these devices. He recently has developed and taught a course on the use of CBCTs for the diagnosis and treatment of orthodontic patients.
Jack Fisher, DMD, completed his orthodontic training at the Medical College of Georgia in 1982. Since then he has been in the full-time practice of orthodontics in Kentucky and Tennessee. He has lectured both in the United States and internationally. Dr. Fisher is a member of the Southern Association of Orthodontics and the American Association of Orthodontics. He is presently a faculty member in the orthodontic department at The University of Tennessee. Dr. Fisher has taught a 2-day cadaver course for the insertion and use of temporary skeletal anchorage devices for 8 years. He has written several articles on the use of these devices. He recently has developed and taught a course on the use of CBCTs for the diagnosis and treatment of orthodontic patients.
Disclosure: Dr. Fisher is a key opinion leader for Planmeca.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
