Drs. Tomás Castellanos and Thomas Pitts introduce a new table to guide vertical placement of brackets based on the effect upon the smile arc
 Drs. Tomás Castellanos and Thomas Pitts introduce a new table to guide vertical placement of brackets based on the effect upon the smile arc
Drs. Tomás Castellanos and Thomas Pitts introduce a new table to guide vertical placement of brackets based on the effect upon the smile arcSummary
Background/objective: The correct placement of brackets is essential not only for functional but for esthetic smile success of the treatment.
[userloggedin]
The objective of this paper is to introduce a new table to guide vertical placement of brackets, based on the effect upon the smile arc.
Therefore, the table is named Guide Position Smile-Arc (GPS-A).
Materials/methods: Two tables, one for upper dentition and one for lower dentition were designed to guide the bracket placement, in order to obtain or retain the best esthetic smile arc, based on the authors´ clinical experience. The limitations of other commonly used tables (Alexander and MBT™) are presented as antecedents of the new table.
Results: Instructions to use the table are described in detail. Indications for previous dental morphology adjustment, use of positioners, and specifications for special situations are described.
Conclusions/implications: The advantages of using this guide are summarized. The clinical table provides an easy and reliable guide for clinicians to place brackets for predictable pleasant smiles and functional occlusions.
Introduction
Facial and smile esthetics are essentially inherent characteristics of the patient. Nonetheless, within morphologic-functional limits, and thanks to the advances in today´s orthodontic technology, it is possible not only to obtain an excellent occlusion but to improve patient esthetics according to his/her expectations. Planning the treatment based on facial esthetics as a purpose to protect the smile arc is parallel to a strategy to achieve occlusal purposes. The functional aim of orthodontics is always to achieve a mutually protected occlusion; that is, anterior teeth protect posterior teeth from interference during lateral and protrusive movements, and posterior teeth protect anterior teeth as well, providing an adequate contact in closed-mouth position.
The smile arc, in a frontal view, has been defined as the relationship of the curvature of the superior incisive and canine incisal edges with the curvature of the inferior lip in smiling position. In an ideal smile arc, the curvature of the superior incisal edge is parallel to the lowest smiling lip curvature. The term “consonant” describes this parallel relationship. In a non-consonant or flat smile, the maxillary incisal curvature is flatter than the inferior lip in smiling position.
According to Frush and Fisher,3 a more sharp curvature of the upper incisal edges from canine to canine is more attractive/youthful than a flatter curvature. Therefore, in individuals who don’t show curvature of the lower lip on smile, a smile arc is still the most desirable. The ideal smile arc as a guidance for anterior upper teeth indicates that the purpose should be an ideal position from canine to canine and a functional anterior bite.
Accurate bracket positioning is essential to finish treatment with an excellent occlusion and beautiful smile. Additionally, the most common reason for unnecessary delay of treatment and the discovery of difficulties in the final stage is the incorrect bonding of the appliances. The need for excessive first order bends is not due to a failure in design of the orthodontic appliances, but due to incorrect bracket positioning. When some teeth are in extreme malposition, it is not always possible to place a bracket in an ideal position during the first visit, but it is recommended to attempt to place the brackets in the best possible position to avoid further repositioning and compensatory bendings as treatment progresses.
Previously established positions for bracket placements based on tooth dimensions, as frequently taught in orthodontic courses and programs, are inappropriate for optimum esthetics. For instance, if one assumes that all patients have the maxillary central incisors located 4.5 mm above the incisal edge, lateral incisors at 4 mm, and canines at 5 mm, and the orthodontist fails to account for the relationship of incisal edges with the lower lip, the position may not adjust for the esthetic criteria needed. Customized appliance placements have as much importance as customized treatment plans.4
Dr. Tom Pitts has developed a protocol for Smile Arc Protection (SAP) bracket positions that consistently produces beautiful Smile Arcs. Dr. Tomás Castellanos has quantified this esthetic positioning by measuring the length of the teeth. Hence, this is a “Tom-Tom” production.
The vertical positioni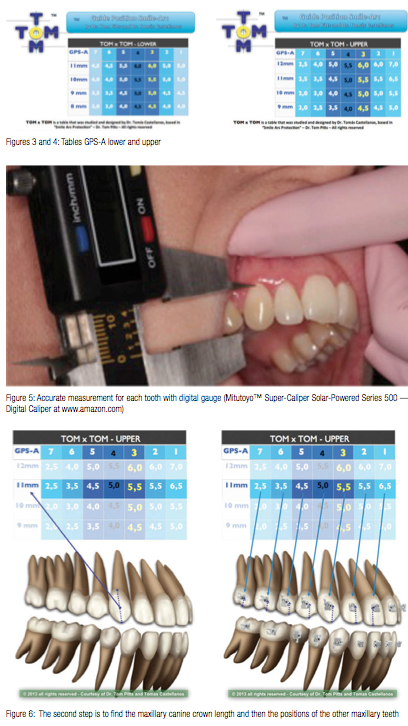 ng of brackets is a challenge for many orthodontists. This problem diminishes when positioning devices and customized tables are used to guide bracket placement, when using direct or indirect bonding.
ng of brackets is a challenge for many orthodontists. This problem diminishes when positioning devices and customized tables are used to guide bracket placement, when using direct or indirect bonding.
The Alexander technique5 uses the premolar height (X in the Vari-Simplex table for bracket heights) (Figure 1) for bracket positions in the entire arch.
For example, if the normal slot height for a premolar bracket is 4.5 mm from the occlusal cusp, the other indicated heights demonstrated by this table should be 5.0 mm for canine, 4.0 mm for lateral, and 4.5 mm for centrals.
The MBT™ table (Figure 2) offers another commonly used bracket positioning guide. It suggests average positions for brackets in the maxillary arch of 4.5 mm for the first premolar (X – 0.5 mm.), 5.0 mm for canine (X), 4.5 mm for lateral (X – 0.5 mm), and 5.0 mm for central (X).6
These and other techniques for bracket placement, based on popular tables and positioning devices, provide accuracy and high reproducibility. Unfortunately, bracket placements with these height discrepancies typically flatten the smile curve.
Flattening of the smile arc during orthodontic treatment can occur by different mechanisms. The normal alignment of maxillary and mandibular dental arches may result in a reduction of curvature of the upper incisors with respect to the inferior lip curvature.
Ackerman, et al.,4 evaluated smile arcs in treated and non-treated patients in their own practices. Almost 40% of the treated patients presented discernible changes in the smile arc with flattening of the smile arc occurring in 32%. In the control group (which was the treated group), 13% presented changes in the smile arcs, but flattening occurred in only 5% of this group. They reported no gender differences regarding smile features in treated or untreated groups.
The present article introduces a new table to guide vertical placement of brackets, based on the smile arc effect — therefore, the table is named Guide Position Smile-Arc (GPS-A) (Images 1 and 2).
Table suggested for vertical placement of brackets
Rationale
The table presented (Figures 3 and 4) is based upon a great number of clinical studies and measurements taken on plaster casts and digital models from patients treated by the team of Drs. Tom Pitts and Tomás Castellanos. Its versatility and efficacy will be the subject of other articles presenting cases successfully treated applying this table.
The table facilitates the vertical placement of brackets in positions that result in adequate smile curves, as well as mutually protected occlusions.
It takes into account occlusal morphology, such as the angle of the articular eminence that is more vertical in dolichocephalic subjects than in mesocephalic or brachycephalic patients. In dolicocephalic patients as compared to brachycephalic, the molar cusps are higher, and fossae are deeper; anterior teeth clinical crowns are longer in a cervico-incisal direction. All these characteristics indicate that more overbite is necessary to disocclude posterior teeth in eccentric movements in dolicocephalic subjects. On the other hand, individuals with shorter faces, flatter TMJ eminences, and anterior teeth with shorter clinical crowns, less overbite is necessary to disocclude posterior teeth in eccentric movements.4
Also when considering the incisal–smile arc relationship, clinicians must extrude the up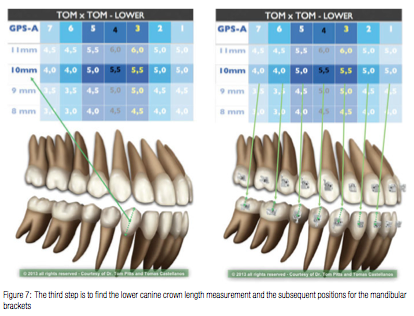 per incisors in flat smile cases or maintain the incisal smile arc when it is esthetically adequate.
per incisors in flat smile cases or maintain the incisal smile arc when it is esthetically adequate.
For a functionally adequate occlusion and esthetic smile curvature, a divergence must be kept between the occluso-gingival position of the slot with occlusal cusps or incisal edges, measured in mm, from the second molar tube all the way to the maxillary central incisor.
This divergence is important as well, considering that the difference in mm between the slot height of the central incisor and the height in mm from the second molar tube gives an idea of the amount of overbite one will obtain at the end of treatment. It also affects the occlusal plane cant.
The final overbite of any deep bite or open bite also depends on elastics, dis-articulation buttons, mini-screws, and other auxiliary elements that potentiate the expression of the bracket’s torque. Of course, mini-screws can also help enhance the maxillary incisor position by intruding the mandibular incisors when needed.
The transition point between the anterior and posterior dental segments additionally establishes the track of the smile arc, and therefore, the positioning for the whole dental arch should be planned taking this point as a clue.
When the maxillary incisors are further extruded to enhance the smile curve and enamel display, a deeper bite can be produced by increasing the overbite. To avoid this effect, the table introduces a compensation in the position of the slot of mandibular canine-to-canine brackets.
Instructions to use the table
(Figures 3 and 4)
Previous to using the table, some patients require a recontouring to provide basic ideal morphology to each tooth. This ameloplastic procedure is based in the study of plaster models and removes only the necessary minimum dental enamel.
The ameloplasty includes pronounced marginal ridges on the lingual surfaces, of incisors’ angles and incisal ridges, as well as irregular vestibular surfaces. Irregular vestibular surfaces prevent an optimum placement of brackets, which control rotations and torque.1
In most cases, canines require re- contouring to improve their role in the smile arc. This process does not interfere with their functional role of canine disocclusion.
Gingival margins are very important for anterior esthetics. Sometimes clinicians need to perform initial gingivoplasties with laser, electro-surgery, or any other similar technique.
It is important to provide the right morphology, but clinicians should not re- contour all hard and soft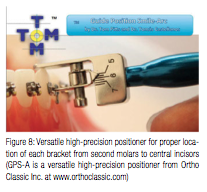 tissues, since leaving small discrepancies until the end of treatment allows for final detailing when the teeth have the best possible position.
tissues, since leaving small discrepancies until the end of treatment allows for final detailing when the teeth have the best possible position.
When teeth have fractures or abnormal wear, the teeth should be reconstructed prior to bracket bonding, in order to assure the ideal dental anatomy. Clinicians should communicate this to the patient, since future restorations may be necessary.
If the maxillary molars present high and pronounced mesopalatal cusps, they should receive recontouring to avoid interferences or early contacts. The same applies to the lingual cusps of the premolars.
After obtaining the ideal dental morphology, the heights for bracket bonding in the maxillary arch are selected as follows:
Measure the length of the maxillary canine crown, from the cusp tip to the gingival margin (after reconstruction, recontouring, or gingivoplasty).
Find this measurement in the columns of the table GPS-A (Guide Position Smile-Arc upper), and choose the adjacent number in the row. (Figure 6). The number in this file indicates the position for each bracket.
Select in a similar way the height to bond brackets for mandibular teeth: a) measure the length of the crown of the mandibular canine, from cusp tip to gingival margin (after reconstruction, recontouring, and gingivoplasty); b) find this number in the column of the table GPS-A (Guide Position Smile-Arc lower), and choose the number in the adjacent row. This number indicates the position for bonding each bracket in the mandibular area (Figure 7).
Specific considerations
The maxillary second molars must always be intruded. Its tubes are always positioned to slightly intrude these teeth to provide a negative coronal inclination and avoid functional interferences.
The discrepancy between maxillary incisors and the maxillary lateral incisor must be kept between 0.5 mm and 1 mm to allow the movement of the mandibular canine during protrusive excursions and, additionally, to improve the smile arc.
Longer incisors require a larger height difference. For those situations, the table includes two additional options.
At the level of the mandibular molars, it is important to maintain an occlusal plane that grants correct coupling with the antagonist teeth.
Individualization of the table for cases treated with premolar extraction
Today’s effective mechanics, combining the use of mini-screws with passive self-ligation appliances for en masse movement toward the place of molar extraction, has reduced the frequency of patients treated with premolar extractions. But when the orthodontist decides that it offers the best option, the table may be individualized. To do this, the anterior segment is managed as conventionally indicated in the GPS-A table, but the discrepancy between premolar and canine for every case will be 0.5 mm, and the discrepancy between premolar and molar will be 1.0 mm in every case, to avoid interferences and inadequate steps in these segments.
Use of the positio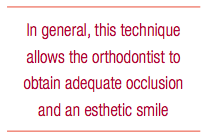 ner for vertical placement of each bracket
ner for vertical placement of each bracket
The positioning gauge that measures the height to bond the brackets is placed in a slightly different way, depending on the segment of dental arch that is being considered.
We suggest for incisor, canine, and premolar regions to use the calibrator placed at 90º respect to the tangent of the middle zone. For the molar region, it is suggested to place it parallel to the occlusal surface of each molar (tracing an imaginary line between the buccal and the lingual cuspids of each molar).
- Advantages derived from the use of this table
- A reduction of errors in positioning, which can be avoided, due to better precision,
- Reproducibility, and predictability of the bracket bonding.
- It allows a practical, standardized bonding procedure.
- Avoids bracket repositioning and/or the introduction of excessive corrective wire bends.
- Reduces chair time and unnecessary discomfort to the patient.
- Saving months of treatment, it becomes an effective tool to motivate patients.
- Allows better control of torque values.
In general, this technique allows the orthodontist to obtain adequate occlusion and an esthetic smile.
REFERENCES
1. Pitts T. Begin with the end in mind: Bracket placement and early elastics protocol for smile arc protection. Clin Impres. 2009;17(1):1-11.
2. Sarver D, Ackerman MB. Dynamic smile visualization and quantification: Part 1. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofacial Orthop. 2003;124(1):4-12.
3. Frush JP, Fisher RD. The dynesthetic interpretation of the dentogenic concept. J Prosthet Dent. 1958;8:558-581.
4. Ackerman JL, Ackerman MB, Brensinger CM, Landis JR. A morphometric analysis of the posed smile. Clin Orthod Res. 1998;1(1):2-11.
5. Alexander W. Build treatment into bracket placement. In: The 20 Principles of the Alexander Discipline. Chicago, IL: Quintessence; 2008:59.
6. McLaughlin R, Bennett J, Trevisi H. Systemized Orthodontic Treatment Mechanics. Philadelphia, PA: Mosby; 2001:60-65.
7. Echeverri E, Sencherman G. Neurofisiología de la oclusión. Columbia: Editorial Monserrate; 1991:175–189.
8. Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2):98-111.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
