Leading the orthodontic sleep apnea movement
 Leading the orthodontic sleep apnea movement
Leading the orthodontic sleep apnea movementHow It All Began
Nearly two years ago, Henry Schein® Orthodontics™ set out on a mission to understand a significant unmet healthcare need of Obstructive Sleep Apnea (OSA). We proposed the hypothesis that changes to the craniofacial structure surrounding the upper airway could have a positive and lasting impact on sleep apnea.
And through our team efforts, we designed an orthodontic strategy that expands the scope of the orthodontic specialty practice (Figure 1). With proper screening, testing, diagnosis, and orthodontic treatment options, orthodontists are helping patients to breath, smile, and thrive again.
Understanding Obstructive Sleep Apnea (OSA)
We discovered that OSA is emerging as one of the most widespread and costly health issues in the United States and is known to affect more than eighteen million Americans, including men, women, and children — 85% of whom are undiagnosed.1,2 The disease is characterized by upper airway obstruction, with repeated gaps in breathing and interrupted sleep.
 People with OSA are at serious risk of medical problems such as stroke,3 heart attack,4 obesity,5 diabetes,6 and motor vehicle accidents.7 Studies show that OSA can be hereditary2, that up to 10% of children have sleep apnea, and that children with sleep breathing disorders can suffer from behavioral problems and lower IQ scores.11 Standard OSA testing and treatment options can deter some patients from being diagnosed and then treated. For example, the continuous positive airway pressure (CPAP) unit is the gold standard for OSA treatment; however, up to 70% of patients are non-compliant or find the machine too uncomfortable to use. For these patients, an alternate OSA solution is needed.
People with OSA are at serious risk of medical problems such as stroke,3 heart attack,4 obesity,5 diabetes,6 and motor vehicle accidents.7 Studies show that OSA can be hereditary2, that up to 10% of children have sleep apnea, and that children with sleep breathing disorders can suffer from behavioral problems and lower IQ scores.11 Standard OSA testing and treatment options can deter some patients from being diagnosed and then treated. For example, the continuous positive airway pressure (CPAP) unit is the gold standard for OSA treatment; however, up to 70% of patients are non-compliant or find the machine too uncomfortable to use. For these patients, an alternate OSA solution is needed.
OSA Advisory Team
In alignment with one of Henry Schein’s core values, “Doing Well by Doing Good,” we gathered a small group of experienced orthodontists from various backgrounds related to sleep apnea. Together, we formed the very first Orthodontic Sleep Apnea Clinical Advisory Team, committed to making a total-health difference in the lives of patients. We know that orthodontists are uniquely trained to identify and treat craniofacial abnormalities and guide the growth of the cranio-facial complex. So, as a team, we asked an important question — Are there potential orthodontic solutions to OSA and sleep breathing disorders that:
- Enable orthodontists to screen for OSA and breathing problems?
- Offer easier routes to diagnosis?
- Provide less invasive and more durable results?
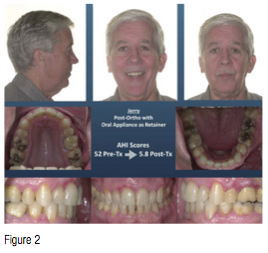 It became clear early in this venture that an estimated 50% of sleep apnea cases involve the bony structure and/or soft tissues around the airway, and by modifying this structure by slow or rapid maxillary expansion (RME/SME),8,9,10 combined orthodontics with mandibular advancement (MA, Figure 2),12,13 or maxillomandibular advancement (MMA),14,15 the orthodontist may be able to address an underlying cause of the condition. With the right information and tools, the orthodontist is ideally positioned to identify, treat, and prevent OSA in children and, perhaps, reverse the condition in adolescents and adults.
It became clear early in this venture that an estimated 50% of sleep apnea cases involve the bony structure and/or soft tissues around the airway, and by modifying this structure by slow or rapid maxillary expansion (RME/SME),8,9,10 combined orthodontics with mandibular advancement (MA, Figure 2),12,13 or maxillomandibular advancement (MMA),14,15 the orthodontist may be able to address an underlying cause of the condition. With the right information and tools, the orthodontist is ideally positioned to identify, treat, and prevent OSA in children and, perhaps, reverse the condition in adolescents and adults.
Together, we created the following mission statement:
To identify and develop the products and protocols that enable orthodontists to improve the lives of people who suffer from Obstructive Sleep Apnea. Our goal is to provide an easier, more efficient route to diagnosis, and treatment of symptoms that yield positive airway changes with more durable results. The Orthodontic Sleep Apnea approach will be a complete system, (Figure 3) intended to establish a new standard of care and an expanded healthcare role for the orthodontist.
 Why Orthodontists and Obstructive Sleep Apnea?
Why Orthodontists and Obstructive Sleep Apnea?
Orthodontists already see a large number of people with airway problems and have been trained in facial growth, development, and airway. Screening patients of all ages provides a more holistic, total-health approach to patient examinations, and opens the door to treat patients and decrease or alleviate symptoms and co-morbidities related to sleep apnea. In addition, orthodontists are well-equipped and trained to provide a solution to many CPAP intolerant patients, who are left without options, when they are not wearing their breathing device.
In 2012, the American Academy of Pediatrics stated that all children should be evaluated for snoring and sleep breathing disorders. OSA-trained orthodontists are singularly positioned to screen and treat children at a very early age, during their first orthodontic visit.
Orthodontic Strategies for Obstructive Sleep Apnea
Henry Schein Orthodontics, in partnership with the Orthodontic Sleep Apnea Clinical Advisory Team, developed the first-of-its-kind program in the orthodontic industry, including a complete, evidence-based system. Drs. Lou Chmura and David Paquette are the program instructors; both have their own personal stories to share about sleep apnea.
This program provides doctors with an understanding of sleep, sleep disordered breathing, and current diagnostic and treatment options, and a new orthodontic approach supported by protocols and products. The orthodontic approach is intended to provide patients with immediate relief from OSA, as well as changes to the airway that may address an underlying cause. We demonstrate innovative technologies and convenient, cost-effective processes to improve the diagnostic and treatment experience for patients of all ages. We also offer a robust practice integration program to help doctors get started. During the program, attendees learn:
- The physiology of snoring and sleep-disordered breathing
- Clinical signs and screening methods for identifying Obstructive Sleep Apnea
- Obstructive Sleep Apnea diagnostic and airway evaluation choices, including patient-friendly home sleep testing and cone beam technology
- How the orthodontic strategy differs from conventional treatment options
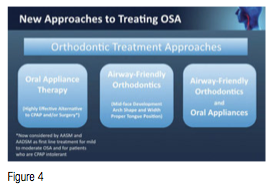
- The roles of mandibular positioning, maxillary arch development, and maxillo-mandibular advancement in airway management and patient treatment (Figure 4)
- How to partner with healthcare professionals for diagnosis, comprehensive care, and new referral sources
- How to bill medical insurance for sleep apnea treatment
- Effective patient awareness, education, and practice marketing resources
- We use training methods such as lecture, video, interactive group discussion, and hands-on exercises with FDA-cleared sleep apnea oral appliances and home sleep testing therapy.
 Moving Forward
Moving Forward
To date, we have hosted nine Orthodontic Strategies for Sleep Apnea courses across the country and are honored to have received overwhelming positive reviews and encouragement from the specialist community. We are inspired by the industry’s enthusiastic response to making a difference in the well-being of sleep apnea patients, and will continue developing our program and support as we identify new trends, technologies, and products. Our goal is to help patients Breathe, Smile, and Thrive™ — our program motto!
We believe that orthodontists should play a central role in the screening, testing, and treatment of sleep apnea patients. If we increase sleep apnea awareness, work with the medical community to ensure proper diagnosis, and provide patients with the highest standard of sleep apnea care, our mission will be accomplished.
We encourage every orthodontist to join the orthodontic sleep apnea movement and make a profound difference in the lives of their patients and community. Come join the mission.
This information was provided by Henry Schein® Orthodontics™.
References
- National Sleep Foundation. 2002 “Sleep in America” Poll. https://sleepfoundation.org/sites/default/files/2002SleepInAmericaPoll.pdf. Accessed August 8, 2014.
- Casale M, Pappacena M, Rinaldi V, Bressi F, Baptista P, Salvinelli F. Obstructive sleep apnea syndrome: from phenotype to genetic basis. Curr Genomics. 2009;10(2):119–126.
- National Institutes of Health. Sleep Apnea Tied to Increased Risk of Stroke. NIH News. 2010. https://www.nih.gov/news/health/apr2010/nhlbi-08.htm. Accessed August 8, 2014.
- Shahrokh-Javaheri MD. Basics of Sleep Apnea and Heart Failure. Sleep Apnea and CV Disease, A CardioSource Clinical Community. 2013. https://apnea.cardiosource.org/Basics/2013/02/Basics-of-Sleep-Apnea-and-Heart-Failure.aspx. Accessed August 8, 2014.
- Fritscher LG, Mottin CC, Canani S, Chatkin JM. Obesity and obstructive sleep apnea-hypopnea syndrome: the impact of bariatric surgery. Obes Surg. 2007;17(1):95-99.
- Brooks B, Cistulli PA, Borkman M, Ross G, McGhee S, Grunstein RR, Sullivan CE, Yue DK. Obstructive sleep apnea in obese noninsulin-dependent diabetic patients: effect of continuous positive airway pressure treatment on insulin responsiveness. J Clin Endocrinol Metab. 1994;79(6):1681-1685.
- Findley LJ, Unverzagt ME, Suratt PM. Automobile accidents involving patients with obstructive sleep apnea. Am Rev Respir Dis. 1988;138(2):337-340.
- Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;27(4):761-766.
- Villa MP, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath. 2011;15(2):179-184.
- Cistulli PA, Palmisano RG, Poole MD. Treatment of obstructive sleep apnea syndrome by rapid maxillary expansion. Sleep. 1998;21(8):831-835.
- Johns Hopkins Medicine. Childhood Sleep Apnea Linked to Brain Damage, Lower IQ. https://www.hopkinsmedicine.org/press_releases/2006/08_21_06.html. Accessed August 8, 2014.
- Kushida CA, Morgenthaler TI, Littner MR, Alessi CA, Bailey D, Coleman J Jr, Friedman L, Hirshkowitz M, Kapen S, Kramer M, Lee-Chiong T, Owens J, Pancer JP. Practice parameters for the treatment of snoring and Obstructive Sleep Apnea with oral appliances: an update for 2005. Sleep. 2006;9(2):240-243.
- Ferguson KA1, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep. 2006;29(2):244-262.
- Holty JE, Guilleminault C. Surgical options for the treatment of obstructive sleep apnea. Med Clin North Am. 2010;94(3):479-515.
- Lye KW, Waite PD, Meara D, Wang D. Quality of life evaluation of maxillomandibular advancement surgery for treatment of obstructive sleep apnea. J Oral Maxillofac Surg. 2008;66(5):968-972.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
