Dr. Duane Grummons discusses how CBCT equips the orthodontist regarding unerupted teeth, facial asymmetry, craniofacial anomalies, temporomandibular (TMD) disorders, airway conditions, TAD planning, and true root information in the region of interest (ROI).
 Dr. Duane Grummons discusses how CBCT equips the orthodontist regarding unerupted teeth, facial asymmetry, craniofacial anomalies, temporomandibular (TMD) disorders, airway conditions, TAD planning, and true root information in the region of interest (ROI).
Dr. Duane Grummons discusses how CBCT equips the orthodontist regarding unerupted teeth, facial asymmetry, craniofacial anomalies, temporomandibular (TMD) disorders, airway conditions, TAD planning, and true root information in the region of interest (ROI).T he AAO recommends orthodontic screening by age 7. To get adequate diagnostic jaw and bite information, the use of low-dose CBCT imaging is often indicated and preferred.
We know enough about its application to consider it the imaging of choice for comprehensive orthodontic treatment.1 This reveals eruption guidance and jaw imbalance decisions and airway/TMJ problems that influence facial growth and development. Patient age is less important since imaging relates to the individual needs and timing. Clinicians establish imaging goals and select the optimal imaging modality to answer clinical questions.
The imaging goals and prescribed need for a low dose, limited field of view (FOV) CBCT scan should be determined after a careful clinical examination. The doctor first evaluates to determine any cone beam imaging need, rather than all patients getting a scan. CBCT is the preferred imaging modality considering patient risks (radiation dose) while also recognizing the implications of not utilizing CBCT and having incomplete diagnostic information.
New thinking and imaging perspectives
Perhaps we as a profession, should change the pretreatment records as a result of technological changes in our profession with CBCT. The standard of care has been elevated such that 3D imaging should be an essential part of certain imaging decisions.2 We should image wisely and always adhere to the ALARA principle. We can obtain a CBCT scan for patients in the range of 27 µSV-80 µSV; less with i-CAT FLX.
Infrequently, do we prescribe a full field of view (FOV) scan at any high resolution or with a long scan time. Such low-dose scans are typically less than full mouth dental X-rays.3
The i-CAT data set equips the clinician to focus on the patient’s individual needs and identify the appropriate imaging parameters, such as whether to capture a limited field of view (FOV) 8 x 8 or 16 x 8, or a single arch or region, versus a full-volume scan. 3D panorals are undistorted4 and make a significant difference, so 81% less errors occur compared to 2D panorals.5
We can focus on an impacted tooth with less radiation. If we are evaluating the airway and/or obstructive conditions, this requires moderate FOV pharyngeal anatomic information with certain specific volumetrics utilizing i-CAT, Anatomage, and/or Dolphin 3D software for computations and assessment, which 2D X-rays do not provide.
Low-dose 3D images
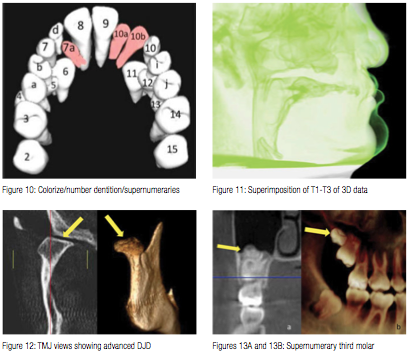
Primary advantages of low dose, limited FOV CBCT are accuracy of image geometry, reliability of measurements, localization of ectopic teeth, and assessment of root resorption.
While achieving quality 3D images is important, capturing scans responsibly with the lowest radiation dose possible is a priority. Clinicians must make prudent decisions about their imaging options for the best diagnostic information for their patients and practices. Practitioners can make evidence-based decisions to prescribe cone beam imaging technologies for acquiring vivid diagnostic images. Low-dose volumes are useful for tasks such as midtreatment assessment of orthodontic patients for root position and angulation within the arch. Our main diagnostic focus includes jaws, alveolar bone around teeth, TMJ, and airway. 3D renderings are the “steak,” not just the “sizzle.”
Daily ambient radiation equals 8 microsieverts (4-7 days in the sun).3 Dental full-mouth X-rays are about 150 µSv and more radiation than a low-dose CBCT scan.3,6 I recommend to keep a 2D ceph and panoral unit for routine orthodontic situations. For our new patients, 2D digital screening images are prescribed for 25%, and 3D CBCT scan for 75%. Of our scans captured, 90% are 5-second scans, and 10% are 9-second or other scans.
 Second opinions
Second opinions
We welcome other opinions, so patients can compare our 3D technology and knowledge base to colleagues. Being “smart” is believing half of what you hear; “brilliant” is knowing which half to believe. Patients become inspired and enthusiastic about treatment with us as they perceive our 3D strengths, which set our practice apart from the competition.
Patients immediately discover and experience the difference between our depth of analysis and information, compared to the quick screening cursory orthodontic exam that occurs in many offices. Often, we treat the outliers — the patients with abnormal conditions. After patients have gone to other doctors seeking an opinion, we regularly find undiagnosed problems in our 3D scan after thorough new patient evaluation. Patients value this.
Once we discover the complete situation and analyze diagnostics, we can explain and visualize findings with the patient, report back to colleagues, and co-manage these conditions. We outline a course of effective and efficient orthodontic therapy for each challenging case and make it clinically navigate/flow well.
Structural analysis
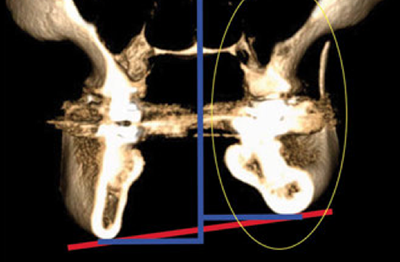
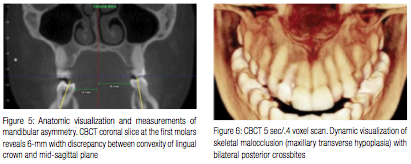
CBCT data and anatomic cranial base superimposition areas make it possible to visualize and specify Class II and Class III asymmetric craniofacial structural etiology. Treatment progress and therapeutic changes can be measured and viewed by visualizing, evaluating, and comparing maxillo-mandibular structures. CBCT in orthodontics equips clinicians regarding problems with erupting teeth, facial asymmetry, craniofacial anomalies, temporomandibular joint (TMJ) dis-orders, airway obstruction, TAD strategies, and root resorption.
 Game changer
Game changer
Cone beam DICOM imaging data and 3D renderings provide exceptional information and exquisite 3D images revealing the craniofacial structures and the mal-occlusions we treat. Treatment changes and comparatives can be truly captured, created, viewed, measured, analyzed, and convincingly visualized. If a treatment challenge is not going according to plan, we can scan to identify and specify why, and then modify our clinical approach.
Discovery and visualization
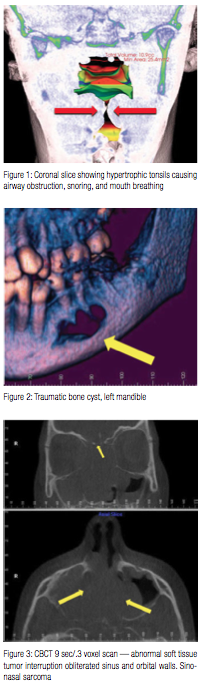
i-CAT imaging allows us to see true clinical anatomy that would not be visible with 2D imaging. In the TMJ region, this includes pathosis, undiscovered fractures, and degenerative conditions. We have found lesions or tumors in the airway and sinuses that extend into the cranial base of the skull and put life at risk. Some frustrated patients have visited multiple doctors with a problem. From the cone beam scan, we have discovered the issues that allowed the specialist to understand the etiology of an abnormal condition. We can help identify and co-manage these conditions. Tumors in jaws and cysts around teeth must be treated first, before orthodontics can begin. 3D imaging helps me outline a course of orthodontics for the challenging case, and so therapy navigates well.

Airway issues
Regarding 3D airway and sleep-disordered breathing or obstructive pharyngeal conditions, clinicians can do harm by doing nothing. “Nobody ever died from crooked teeth” — say that to the man who fell asleep at the wheel. Some ENT and sleep doctors tell patients that what we identify on our i-CAT CBCT scans is what they primarily trust and rely upon. This has helped immensely to improve our clinical effectiveness, best patient care, and referral relationships.
Nasal breathers have greater airway volumes.7 RME maxillary orthopedic growth modification is effective for increasing nasal airflow.8 The oropharynx and nasopharynx volumes of Class II subjects are significantly lower than other groups.9
Education and communication
Patient education is an important part of our practice, and teaching about radiation exposure is a priority. We don’t wait for patients to ask. We educate them before an image is taken. We explain and demonstrate the FOV and scan resolution we select as best and safe for individual needs. We explain by comparing the radiation from a scan to the everyday environment, like an extended airplane flight or weekly ambient radiation, which typically is more than one low-dose limited FOV scan.
 3D users must be ready to inform our peers about radiation comparisons as well. If another colleague says that the panoramic image is good enough, we must know deeply about 3D imaging to explain the difference between radiation and distortion from a 2D X-ray versus a 3D scan, and compare the benefits of 3D cone beam images for diagnosis and treatment planning. This technology keeps getting better. The 3D CBCT from i-CAT™ (the i-CAT™ FLX) offers a QuickScan+ feature that captures a full-dentition 3D scan without distortion.
3D users must be ready to inform our peers about radiation comparisons as well. If another colleague says that the panoramic image is good enough, we must know deeply about 3D imaging to explain the difference between radiation and distortion from a 2D X-ray versus a 3D scan, and compare the benefits of 3D cone beam images for diagnosis and treatment planning. This technology keeps getting better. The 3D CBCT from i-CAT™ (the i-CAT™ FLX) offers a QuickScan+ feature that captures a full-dentition 3D scan without distortion.
Anywhere Dolphin, ScreenFlow, and Dropbox communications
We improve communications with such tools as colorization and different trans-lucencies to depict the 3D anatomy and its influence upon the course of treatment. Digital communications: email by AnywhereDolphin.com is HIPAA compliant; Dropbox.com or Box.com (DICOM and image file sharing), CDs, flash drives, GoToMeeting, Skype, MAC ScreenFlow, video messaging, and live video chat are used.
3D imaging photo overlays accurately depict the smile dynamics and facial anatomy. Video clips are better for soft tissue smile animation and dynamics of the smile. Relax the smile to repose; animate the smile fully; and return to neutral. This displays the teeth and muscular function during speech and smiling.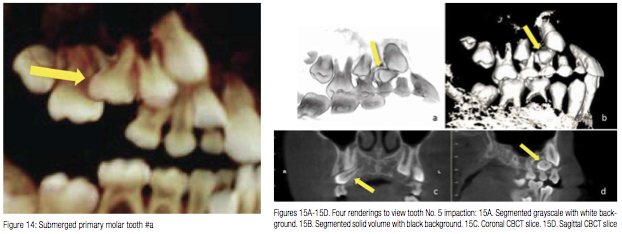
Concluding remarks
When considering the safety zone of X-ray exposure, it helps to compare to our ambient exposure of 8µSv per day. The radiation exposure for a round-trip flight from San Francisco to New York is approximately 72µSv, about equal to one CBCT scan.10 We do not disregard any risk of dental X-rays. However, when we discuss the move in orthodontic imaging from traditional pan/ceph to CBCT cone beam volumetric tomography (CBVT), there should not be disagreement about exposure risk. The risks of medical imaging at effective doses below 50,000 microsieverts for single procedures are too low to be detectable and maybe nonexistent.11
i-CAT is known for its low-dose radiation, a fact appreciated by patients. The diagnostic benefits of CBCT have been clearly substantiated by research and clinical circumstances. A primary benefit of CBCT is in seeing the anatomic truth. You don’t know what you can’t see. How else can you visualize airway, TMJs, transverse relationships, buccal-lingual widths of bone, and teeth/root positions all in one simple low-dose scan? There is no comparison.12 The transformation of my clinical practice with i-CAT CBCT 3D is extraordinary.
Imaging goals and CBCT protocol seek answers to specific clinical questions utilizing a precise and exquisite display of relevant anatomical representation. Individualized patient findings are closely analyzed by the clinician. Each of us has huge capacity to continuously learn and achieve to become brighter and better. One is not a successful clinician until fullest efforts have been made to become the best one can be in providing the finest individualized patient care. The future is now. Together, we lead the way with i-CAT cone beam and related technologies in modern orthodontic practice. Stay out in front — the lead dog has the best view in the race. See you at the top!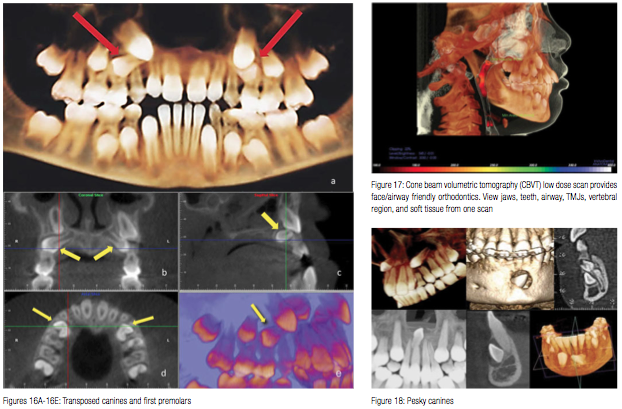
References
1. Larsen BE. Cone-beam computed tomography is the imaging technique of choice for comprehensive orthodontic assessment. Am J Orthod Dentofacial Orthop. 2012;141(4):402, 404, 406.
2. Curley A, Hatcher DC. Cone beam CT — anatomic assessment and legal issues: the new standards of care. J Calif Dent Assoc. 2009;37(9):653-662.
3. Unites States Nuclear Regulatory Commission. Radiation Dosage. https://www.nrc.gov/.
4. Haney E, Gansky SA, Lee JS, Johnson E, Maki K, Miller AJ, Huang JC. Comparative analysis of traditional radiographs and cone-beam computed tomography volumetric images in the diagnosis and treatment planning of maxillary impacted canines. Am J Orthod Dentofacial Orthop. 2010;137(5):590-597.
5. Granlund CM, Lith A, Molander B, Gröndahl K, Hansen K, Ekestubbe A. Frequency of errors and pathology in panoramic images of young orthodontic patients. Eur J Orthod. 2012;34(4):452-457.
6. Ludlow JB, Walker C. Assessment of phantom dosimetry and image quality of i-CAT FLX cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2013;144(6):802-817.
7. Alves M Jr, Baratieri C, Nojima LI, Nojima MC, Ruellas AC. Three-dimensional assessment of pharyngeal airway in nasal- and mouth-breathing children. Int J Pediatr Otorhinolaryngol. 2011;75(9):1195-1199.
8. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;15;27(4):761-766.
9. El H, Palomo JM, Airway volume for different dentofacial skeletal patterns. Am J Orthod Dentofacial Orthop. 2011;139(6):e511-e521.
10. Carlson S, Graham J, Harrell WE Jr, Lin EY, Molen A, Womack WR. The truth about CBCT radiation. Orthotown. 2011;Sept:62-68.
11. American Association of Physics in Medicine, December 13, 2011.
12. Grummons D. Innovations for CBCT with 3D Diagnosis and Orthodontic Planning and Treatment. Orthotown. September 2012;50-53.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
