CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This clinical article aims to discuss the aspects of CBCT imaging that improve treatment planning and diagnostics.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking this quiz to earn 2 hours of CE from reading this article.
- Correctly answering the questions will demonstrate the reader can:
- Identify the uses of CBCT technology.
- Identify common rendered images.
- Realize why using CBCT technology would be beneficial in patients with dentoalveolar boundaries.
- Recognize the importance achieving low radiation dose for CBCT imaging without losing diagnostic image quality.
- Realize the different aspects of multi-planar reconstruction.
- Identify various diagnostic aspects of 3D analysis.

Dr. Jay B. Burton discusses the aspects of CBCT imaging that improve treatment planning and diagnostics
CBCT has changed everything in my practice life — from treatment planning to treatment options to mechanotherapy, and even evaluation of treatment results. At this point, it is honestly difficult for me to imagine practicing without it. In discussions with other doctors about using CBCT, the topic of impacted canines frequently arises, even though less than 5% of orthodontic patients have an impacted tooth.1 It seems unnecessary to purchase a CBCT machine if this is the primary or only reason. If this is the case, patients with impacted teeth could be sent to an oral surgeon who has a CBCT and will share his/her copy of the volume, which usually will already be captured as a part of treatment protocol.
Some of the most obvious uses for CBCT technology are in maxillofacial dysmorphology and orthognathics. These applications include craniofacial and orthognathic issues, TMJ, airway, and cases involving pathology. Other indications focus on the anomalies of dentition — specifically, indications for impacted teeth, supernumerary teeth, and wisdom teeth evaluation/impactions.
Another more recent application since the advent of skeletally fixated expanders are for patients with transverse discrepancies. Of particular concern, and perhaps even overlapping with the topic of dentoalveolar boundaries, would be whether or not orthodontists are able to use traditional rapid maxillary expanders in patients needing expansion or whether a skeletally fixated expander should be used. These decisions can now be made with information regarding the amount of bone located on the buccal of the teeth to which the appliance would be attached.
The question of these dentoalveolar boundaries is significant as we can now consider the limitations to treatment specifically in the AP and transverse dimensions. One example is the patient who may need extractions due to bimaxillary protrusion. Orthodontists can consider the amount of bone available in the direction the teeth are to be moved and even simulate the tooth movement revealing exactly how much bone would be present if that treatment plan were carried through. Orthodontists must also now consider the possibility and/or reality that, in many cases, there may be a lack of bone in the direction we would like to move the teeth, resulting in the question of whether or not the patient should be treated. When considering these boundaries, we also must consider morphology for cases that will involve dental implants, bone grafts, or temporary skeletal anchorage devices.
Radiation dose
Radiation dose is always a concern for orthodontists, especially since many ortho-dontic patients are children. CBCT in orthodontics has become more of a possibility since the advent of Ultra Low Dose™ (ULD) technology developed by Planmeca — one example of a manufacturer that offers this type of low dose imaging while maintaining the diagnostic image quality necessary for effective treatment planning.2
CBCT offers more information about the patient than 2D radiography is able to provide. While under our care, the less radiation that the patient is exposed to, the better. It is now possible to take a full field of view (FFOV) CBCT with less radiation than a traditional 2D digital pan and ceph.2 The 3D unit from Planmeca that uses Ultra Low Dose technology has changed the way I personally approach orthodontic treatment. The Ludlow, Koivisto 2014 study noted, “An average reduction in dose of 77% was achieved using ULD protocols when compared with standard protocols. While this dose reduction was significant, no statistical reduction in image quality between ULD and standard protocols was seen. This would suggest that patient doses can be reduced without loss of diagnostic quality.”2
It is important to me to have the ability to use and maintain ALARA protocols, while retaining as much image quality as possible. Just because a lower radiation dose may be achievable, it does not mean that it is diagnostically acceptable. Many of the treatments discussed in this article become relevant only after obtaining the information garnered by a CBCT. Some would say that 2D should be used first, and when indicated, a 3D CBCT should be taken. My response to that is, “Why would you over-irradiate your patients when you can take a 3D CBCT with less radiation than even a 2D pan?”
This article focuses on the practical and beneficial uses of this technology. The discussion will focus on the use of multi-planar reconstruction (MPR) for general diagnostics/pathology/incidental findings. Attention will be given to when and how this technology can be used and recommended. A fully integrated intraoral scan, taken with an intraoral scanner (Emerald™ by Planmeca in my office), allows for a streamlined approach to diagnosis and treatment planning as well as the ability to virtually simulate treatment with respect to the patient’s individual anatomy.
Rendered/reconstructed images
The number of different types of reconstructed images possible is limited only by the clinicians’ need and imagination. Orthodontists can view any part of the volume in three planes of space to localize and better visualize that which they are interested in seeing. Specific rendered images useful for orthodontic diagnosis and treatment planning purposes will be discussed as well.
Multiplanar reconstruction (MPR)
Figure 3 shows a multiplanar reconstruction (MPR) view in three planes of space: coronal, sagittal, and axial as well as a 3D reconstructed view of the skull. This is really the starting point from which to begin examining each case. Many orthodontists who use 3D-imaging technology begin their diagnostic/treatment planning process by first examining the information from all of the slices in each plane prior to even thinking about orthodontic diagnosis and treatment decisions (as these can be distractions while the clinician is looking for incidental findings and pathology). This is done for the same reasons that pans are reviewed for pathology prior to determining treatment. It is important to point out that the clinician can easily become distracted by the 3D reconstruction. When reviewing a CBCT for pathology, it is important to spend time appreciating the sagittal, axial, and coronal views. The lure of the wow factor of the 3D rendering, if the clinician is not used to manipulating these images, can be quite enticing/distracting.
Reviewing a CBCT: when and how
With regard to when and how, the author likes to review the CBCT at three distinct time points.
- Immediately after the scan is taken (quick review).
- During diagnosis and treatment planning (case workup).
- During the treatment plan consult with the patient.
By reviewing the CBCT at these three time points, clinicians can reduce the likelihood that any potentially important detail/finding will be missed.
Figure 3 shows the traditional MPR view revealing the coronal, axial, and sagittal planes. Most orthodontists are familiar with the collapsed version of these images as the PA cephalometric radiograph, the submentovertex radiograph, and the lateral cephalometric radiograph. Essentially, CBCT allows the clinician to expand out the 2D images and look at specific areas of interest as a result of being able to scroll through the various planes and slices.
CBCT for orthodontic purposes
 There has been a lot of discussion and training available to practitioners on recognizing incidental findings and pathology, but little to no training as to how to use CBCT for orthodontic diagnostic purposes. The remainder of this article will focus on meeting this need and discussing some of the important diagnostic capabilities unique to CBCT.
There has been a lot of discussion and training available to practitioners on recognizing incidental findings and pathology, but little to no training as to how to use CBCT for orthodontic diagnostic purposes. The remainder of this article will focus on meeting this need and discussing some of the important diagnostic capabilities unique to CBCT.
Integration of I/O scans into volume
A beneficial feature is registration of an intraoral scan or model scan into the CBCT volume. Given the speed with which the clinician can take an intraoral scan now, it only makes sense to do so on all new patients. With this information, we truly have a “digital patient” to treatment plan the case with, and if needed, even perform treatment simulations.
Common rendered images
Rendered panoramic view
The reconstructed panoramic view is probably the most common reconstructed image from a CBCT volume that is used for dental purposes. A point of contention regarding rendered 3D pans has been the image quality/sharpness. The quality of the rendered pan is dependent upon the resolution at which the 3D volume was taken. A traditional 2D panoramic radiograph is typically not taken with the patient in occlusion due to the limited focal trough necessary for a quality 2D panoramic radiograph. With the 3D volume for orthodontic purposes, the CBCT is generally taken with the patient in centric occlusion. This can be done because of a feature available with most 3D-imaging programs, which allows the ability to manipulate the focal trough and further refine the width of that trough to make sure that all dental structures are included. This functionality helps the clinician achieve a more meaningful image and, as a result, have fewer retakes, thereby further reducing radiation levels as a result of poor patient positioning. The benefit of the 3D pan in orthodontics specifically is that clinicians can determine the molar class and midline as a result of the volume being taken and occlusion. Granted, at the resolution of ULD/LD setting, the panoramic reconstruction won’t be as “pretty” as a 2D image, but the amount of information available from the volume will be substantially more than that of a traditional 2D pan.
This brings me to the question, Why do we as orthodontists take a panoramic radiograph anyway? Generally speaking, the purpose of the panoramic image is to provide a general overview of the teeth and bony structures, which will be involved in treatment. It is also used to confirm the presence/absence of teeth, including supernumerary/impacted teeth and for a very cursory view of the TMJ to determine if further imaging of the joint might be needed.3
Rendered lateral cephalometric view
When we think about a rendered image from a 3D volume, it is important that there is no magnification error in these images.4 Because magnification errors exist in 2D images, many of the norms that are used will have this error as part of the norm. The significance of this is minimal, though, if it is important to the clinicians that they should know that most 3D-viewing software will allow the creation of a rendered image with synthetic magnification error added. Figure 5 shows the difference between a volume rendered both with and without magnification error.
Another benefit of rendered images is that the clinician no longer has to retake an image due to poor patient positioning. This is because the 3D volume can be reoriented in any position desired by the clinician, with the most common being based on natural head position. With the rendered lateral ceph, the orthodontist can use a photo taken in natural head position to manipulate the orientation of the rendered image.
3D analysis
Orientation of the 3D volume
When reviewing the 3D volume in the multiplanar reconstruction view, it is important to first orient the volume in all three planes of space. For orthodontic purposes, the clinician should try to get this as close as possible to the patient’s natural head position.
Once the volume is oriented, I begin by reviewing the coronal and axial views, primarily looking for symmetry and/or asymmetry. Many times, pathology will reveal itself in an asymmetrical manner. Lastly, I review the sagittal view, and many times, if I see something of interest, I will hone in on that area in all three planes of space. One of the last details I look at is the 3D reconstruction to confirm what I have already seen in the sagittal, axial, and coronal views. This cannot be stressed enough. The old adage that says, “Don’t miss the forest for the trees,” is one that comes to mind when thinking of what can happen upon opening a 3D volume. There is so much information that it is very easy to get distracted.
Immediately after the volume has been taken, it should be reviewed. It is very important that all three planes of space are looked at, and that vital tissues are examined. This is where many orthodontists and dentists get intimidated. Orthodontists are traditionally trained to look at PA cephs, lateral cephs, and a submentovertex in 2D. When reviewing sagittal, axial, and coronal views, the clinician is simply looking at slices within that 2D film.
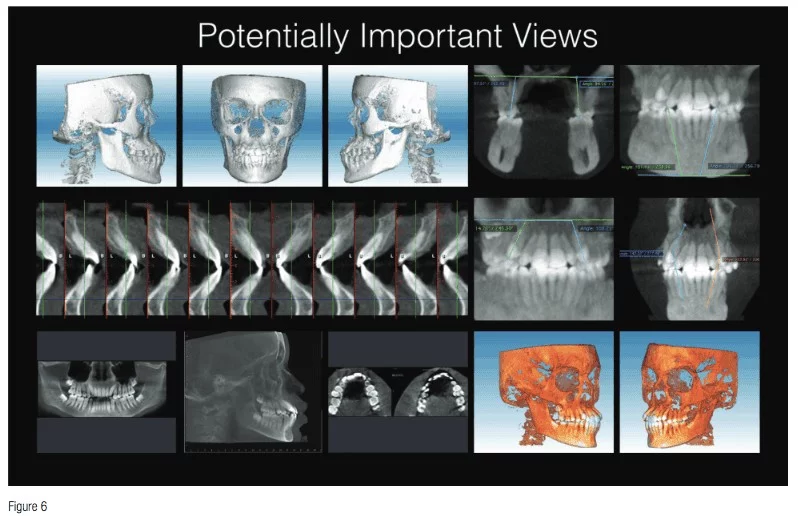
When it comes to 3D analysis, the clinician soon begins to realize the need to treat to the individual anatomy of a patient versus the historical 2D norms with which orthodontists are trained. Some university programs as well as other individuals have developed 3D analyses that pool specific views with which they have developed 3D norms. I find that it is more important to treat to the individual anatomy rather than available ethnic norms. In Figure 6, you will see views or images that I create on a regular basis, which are beneficial for diagnostics and treatment planning purposes. The top left of Figure 6 shows solid body views of the skull in the left frontal and right side orientations. Other images in the figure show intermolar and intercanine angulations and interarch-canine angulation, interincisal angles as well as alveolar bone boundaries. Also important for diagnosis and treatment planning is the reconstructed pan and reconstructed lateral ceph. Coronal reconstructions of the dentition will allow the clinician to measure intermolar and intercanine distances as well as a multitude of other images that can be used for treatment decisions.
An important point to take note of is simply the amount of information clinicians are faced with once this technology is adopted. It becomes very important to develop a systematic approach for both the review of the CBCT for incidental findings/pathology as well as for treatment planning decisions.
Conclusion
I hope that this article has provided a better understanding of the need for CBCT in orthodontics as well as how this technology can be used to better visualize anatomy for proper diagnosis and treatment planning. The comment that most frequently comes up in conversation with an orthodontist considering the purchase of a CBCT machine is not whether or not they will adopt the technology, but when they will do so. As was my personal experience, I believe that once orthodontists have used the technology on a regular basis, it becomes easy to see why they would not want to practice without it.
Now that radiation dose for 3D is less than that for 2D, it is really not a question of technology for technology’s sake; rather, it is a radiation hygiene issue that must be answered.
Dr. Duane Grummons also discussed visualizing anatomy with CBCT in his article “CBCT and 3D imaging goals for orthodontic patients.” Read his ideas on 3D imaging here.
Author Info
 Jay B. Burton, DMD, completed his undergraduate education at Bethel University and earned an MBA from The University of Tennessee at Martin, before achieving his Doctor of Dental Medicine degree at the University of Louisville. While in dental school, Dr. Burton served as class president and conducted dental mission work in Belize and the Philippines. Dr. Burton subsequently completed his Orthodontic Residency at the prestigious New York University (NYU) in Manhattan before achieving certification from the American Board of Orthodontics. Aside from his passion for making healthy smiles, Dr. Burton enjoys spending time with his wife, Sarah, and their children, Nora, Baker, and Charlotte. Dr. Burton can be reached through www.smilemaker.com.
Jay B. Burton, DMD, completed his undergraduate education at Bethel University and earned an MBA from The University of Tennessee at Martin, before achieving his Doctor of Dental Medicine degree at the University of Louisville. While in dental school, Dr. Burton served as class president and conducted dental mission work in Belize and the Philippines. Dr. Burton subsequently completed his Orthodontic Residency at the prestigious New York University (NYU) in Manhattan before achieving certification from the American Board of Orthodontics. Aside from his passion for making healthy smiles, Dr. Burton enjoys spending time with his wife, Sarah, and their children, Nora, Baker, and Charlotte. Dr. Burton can be reached through www.smilemaker.com.
Disclosure: Dr. Burton is receiving an honorarium from Planmeca for this article.
References
- Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial. Orthop. 1992;101(2):159-171.
- Ludlow JB, Koivisto J. Dosimetry of Orthodontic Diagnostic FOVs Using Low Dose CBCT protocol. University of North Carolina/University of Helsinki. Charlottesville: UNC/UH. (2014).
- Proffit, WR, Fields HW, Sarver, DM. Contemporary orthodontics. St. Louis, Mo: Mosby Elsevier; 2007
- Mah JK, Yi L, Huang RC, Choo H., Advanced Applications of Cone Beam Computed Tomography in Orthodontics. Semin Orthod. 2011,17:57-71
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
