CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to discuss the use of the Alias™ lingual appliance passive self-ligating, square-slot lingual bracket system.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions to earn 2 hours of CE from reading this article. Click here for the quiz. Correctly answering the questions will demonstrate the reader can:
- Identify instances for which fixed appliance treatment would be a more appropriate choice than removable appliances.
- Identify instances where lingual systems would be more appropriate than labial systems.
- Identify some characteristics of the Alias™ lingual appliance.
- Recognize some benefits of using this system for certain patients.

Drs. John R. “Bob” Smith and Mario Paz discuss the development and use of a square-slot, passive self-ligating, straight-wire lingual appliance
Considering the evolution of lingual orthodontics, it is worth noting that the lingual technique gained limited popularity in the United States and Canada during the early 1980s. In the intervening years — partly due to the clinical difficulties associated with it during its early development and the success of esthetic alternatives — lingual therapy has languished in North America. Educated later with improved techniques, clinicians in Europe and Asia had greater success with lingual therapy where its use has become much more common.
An October 2013 AAO survey, entitled “The Economics of Orthodontics,” found that the number of orthodontic starts in the U.S. and Canada increased 20% between 2010 and 2012 with a 14% increase in the number of adult patients over the age of 18 during that same period.1 Certainly, the tremendous growth of Invisalign® is testament to the demand for esthetic appliances and is what adults and even teens come into offices asking for. While aligners enable us to perform suitable corrections for many patients, there are times when fixed appliances are a better choice. And the conversation moves considerably in favor of fixed appliance treatment when we introduce lingual therapy.
Lingual offers a high level of care with optimal esthetics and minimal compliance issues. It can serve as an important strategy for sustained practice growth since it’s a specialist’s treatment modality, not something a GP would likely adopt. Moreover, the adult segment of the market offers tremendous growth opportunity since the penetration of it currently stands at a mere 5%.
 While Invisalign has driven a demand for esthetic orthodontic treatment in the adult and teen population, in some circumstances, a removable appliance is not able to achieve the level of care as reliably as a fixed treatment alternative (Figures 1A-1C). In such cases, if metal or clear labial braces will not satisfy the patient esthetically, lingual treatment is a powerful tool to have at the clinician’s disposal (Figures 1D-1F).
While Invisalign has driven a demand for esthetic orthodontic treatment in the adult and teen population, in some circumstances, a removable appliance is not able to achieve the level of care as reliably as a fixed treatment alternative (Figures 1A-1C). In such cases, if metal or clear labial braces will not satisfy the patient esthetically, lingual treatment is a powerful tool to have at the clinician’s disposal (Figures 1D-1F).
Additionally, patients who originally come in seeking clear removable therapy, when apprised of its compliance aspect, will often opt for lingual treatment instead. If a fixed appliance is more appropriate for their particular case, their decision for lingual is reinforced. Friends, co-workers, and spouses of our lingual patients who had clear removable treatment and struggled with compliance or learned later that fixed appliance treatment would likely have given them a superior result admit that they wish they had been given the option of lingual treatment. Being able to propose lingual treatment — the ultimate esthetic option — gives clinicians a needed and now efficient tool to fulfill these patients’ expectations cosmetically without compromising the finish.
The new Alias™ lingual appliance (Ormco) is the profession’s first passive self-ligating, square-slot lingual bracket system. Specifically, if we were to take a look at the patented .018 x .018 square slot of the Alias PSL lingual appliance, there are a number of benefits for doctors. With passive labial self-ligation, the standard .022 x .028 rectangular slot does not facilitate rotational control until placing .014 x .025 Cu Ni-Ti wires. Given the greater inter-bracket width and the .018 x .018 square slot — exclusive to the Alias PSL lingual appliance — clinicians can realize the benefits of early rotational and torque control with smaller diameter, more flexible arch wires. Because of the tight wire-bracket interface tolerances, there is less wire spin and play. The 016 x .016 Cu Ni-Ti wire is an excellent wire to gain both rotational and the first stage of torque control.
The slot provides improved torque control when reaching full-sized wires. It’s always been difficult to insert a .018 x .025 stainless steel wire in a standard lingual slot without the risk of debonding the bracket — even when the case is fully aligned and ready for this size wire. The full-size wire for the appliance is the much smaller .018 square wire, which makes insertion easier yet maintains vertical root control during final torque refinements near the end of treatment.
Moreover, the solid fourth wall of the bracket maintains torque control when retracting posterior teeth and closing spaces with a power chain. The wire can’t pull out of the slot as it can with a conventionally ligated bracket. In part, it is the way the wires insert in the posterior — going in vertically. Plus the snug fit of the .018 square wire in the .018 slot (when the self-ligating door is closed) maintains axial inclination, fostering tooth translation rather than tipping.
In terms of additional advantages, vertical wire insertion improves visualization of the wire-slot interface and simplifies wire placement. The small bracket dimensions provide more comfort with less occlusal and speech interference compared with numerous options on the market. Self-ligation appreciably reduces clinical chair time compared with steel ligation or double over-tie elastomers. There are also the inherent advantages of “straight wire”— simplified protocols with no or fewer wire bends to disrupt sliding mechanics, and easier archwire coordination and finishing.
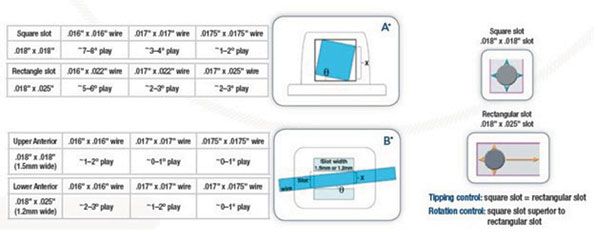
While in some cases the wire may not be a “perfectly straight wire in appearance,” it will not have sharp bends like the typical lingual mushroom archwire that greatly inhibits sliding mechanics. The goal is to maintain the straight-wire shape. Additionally, the square slot offers important advantages over the typical rectangular lingual slot — better tip control and appreciably better rotational control.
 Patients have reported the considerable comfort of Alias, which boasts rounded edges, a small shape and noticeably low profile (Figures 2A-2C). The passive aspect of this self-ligating bracket also means clinicians will see many of the same benefits associated with passive self-ligating labial appliances — better sliding mechanics with less friction for faster arch unraveling and transverse width development (Figures 3A-3C). Effective tooth translation with better mesial-distal root tip control has also been reported.
Patients have reported the considerable comfort of Alias, which boasts rounded edges, a small shape and noticeably low profile (Figures 2A-2C). The passive aspect of this self-ligating bracket also means clinicians will see many of the same benefits associated with passive self-ligating labial appliances — better sliding mechanics with less friction for faster arch unraveling and transverse width development (Figures 3A-3C). Effective tooth translation with better mesial-distal root tip control has also been reported.
 For patients, treatment length has always been of the utmost importance. Judging this bracket against time spent ligating conventional lingual twin brackets, these self-ligating lingual brackets offer tremendous time savings. While there are no studies yet on ligation time of lingual self-ligating versus other lingual bracket systems that require traditional ties, the studies of labial brackets, self-ligation versus twin brackets, have demonstrated considerable time savings. We would think the magnitude of improvement should be comparable.3,4 In our hands, it’s shown almost 50% improvement in time, which is much appreciated by the staff. Also, the use of passive self-ligating brackets forces staff to stay in arch wires until they’ve been fully expressed. Staff can’t proceed to the next larger wire unless the case is ready for it because they can’t close the brackets to secure the wire properly. This standardizes archwire progression, which they appreciate because it takes the guesswork out of it and keeps treatment on track.
For patients, treatment length has always been of the utmost importance. Judging this bracket against time spent ligating conventional lingual twin brackets, these self-ligating lingual brackets offer tremendous time savings. While there are no studies yet on ligation time of lingual self-ligating versus other lingual bracket systems that require traditional ties, the studies of labial brackets, self-ligation versus twin brackets, have demonstrated considerable time savings. We would think the magnitude of improvement should be comparable.3,4 In our hands, it’s shown almost 50% improvement in time, which is much appreciated by the staff. Also, the use of passive self-ligating brackets forces staff to stay in arch wires until they’ve been fully expressed. Staff can’t proceed to the next larger wire unless the case is ready for it because they can’t close the brackets to secure the wire properly. This standardizes archwire progression, which they appreciate because it takes the guesswork out of it and keeps treatment on track.
When patients are happy, staff is happy, and we have noticed fewer patient complaints about soreness and speech interferences with the smaller size bracket. Our staff also reports that there is a huge improvement in ease and time savings for wire changes with it because of the way the brackets open.
Long-tenured staff members, especially those who have suffered from (or even have had surgery for) carpal tunnel syndrome appreciate the ease of self-ligation. Tying steel ties or attaching elastics onto conventional lingual brackets is even more straining than it is with labial brackets.
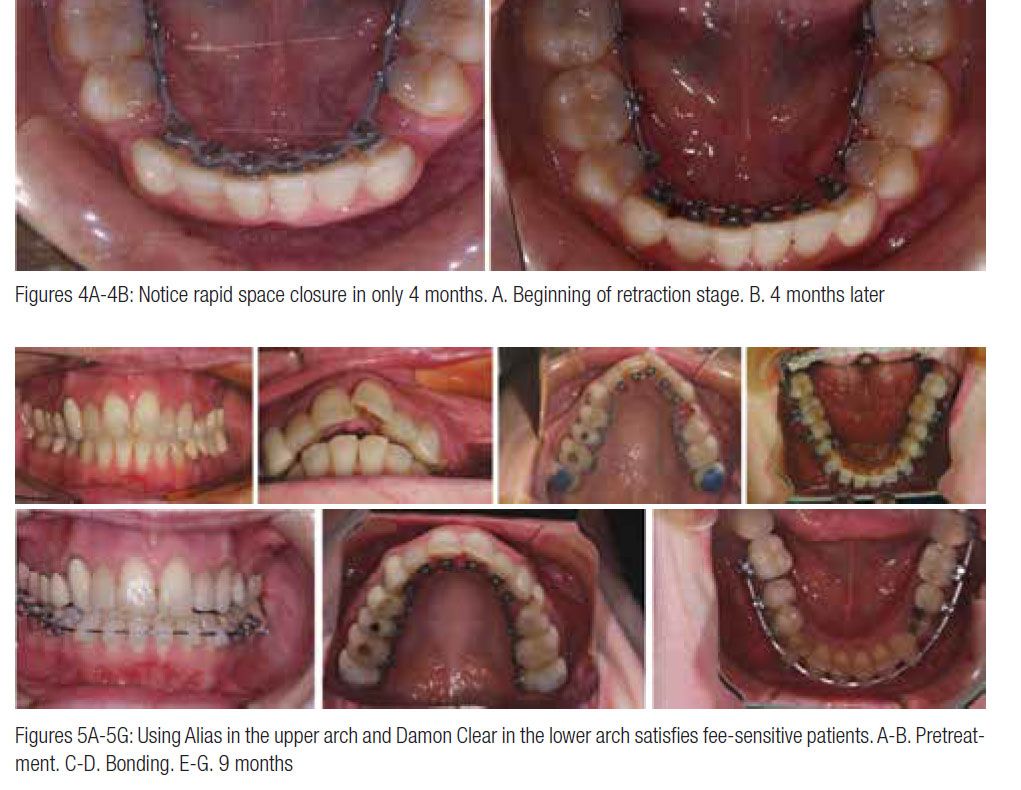
The biggest surprise with this system was the velocity of tooth movement both in nonextraction and extraction cases — even though I’ve had considerable experience with the Damon™ System passive self-ligating labial bracket with similar results (Figures 4A-4B). We’re sure to cinch back the early archwires or leave them shorter, so they have room to move distally without irritating tissue. Clinicians unfamiliar with passive self-ligation will need to be careful to use Ormco-supplied lingual archwires and follow the prescribed wire progression in order not to overpower the system and thus over-expand arches.
Because it’s a straight-wire system, we’re also able to use packaged lingual wires and shape them ourselves to duplicate a wire, if needed. While we seldom need to resort to this option, it’s a real timesaver when we do. There is considerable added expense and potential treatment delay to order and receive a replacement wire with appliance systems that provide technique-sensitive, robotically shaped wires.
For case presentations, as professionals, we educate our patients about the best approaches to solve their orthodontic challenges. Our case presentation schools patients about their condition and its degree of treatment difficulty. Through the discussion phase of the presentation, we come to agreement about the best appliance, timeline for treatment, and cost. If the patient has very high esthetic demands and rejects labial clear brackets, the choices are either clear aligners or lingual braces. The difficulty and odds of success with clear aligners steers the conversation from that point. If I feel I need a fixed appliance, then the lingual appliance is my recommendation.
We offer lingual treatment as an option in all teen and adult case presentations — even for selected Phase I treatment. Lingual therapy gives us the full capability of a fixed appliance that avoids the possible compromises with removable appliance therapy. With lingual treatment, we have the same force capabilities and treatment control as labial therapy, so we never have to settle for a compromised treatment result.
To increase patient comfort and lessen speech interferences in patients with restricted lower arches and/or considerable lower arch crowding, we sometimes recommend lingual appliances for the upper arch and esthetic labial brackets (Damon™ Clear) on the lower arch (Figures 5A-5G). We price this option more affordably than full lingual; so if the fee is a major consideration for particular patients, this combination can be quite satisfactory.
Conclusion
Being able to offer efficient lingual treatment in lieu of an esthetic labial option is vital to competing in today’s competitive market that has become extremely insistent on esthetic treatment. While patients in Southern California are certainly demanding of esthetic solutions, we don’t feel that they’re appreciably more demanding than most people across the U.S. In fact, even years ago, Dr. Jack Gorman had more lingual patients in Marion, Indiana, than doctors in larger metropolitan areas.
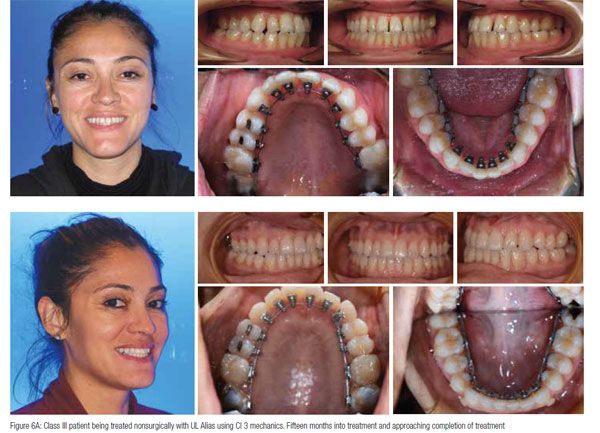
With the recent modifications made to the Alias appliance, we are continuing to notice the speed and reliability of movement. Archwire sequence used on the case described below has been as follows:
- 014CN, 016CN as initial wires
- 16 x 16 CN
- 18 x 18 CN
- 016 TMA to be used for finishing stage
We noticed decreased speech interference due to small bracket design and diminished initial discomfort from initial light forces. Excellent torque control is due to precise fit of the square archwire in the square bracket slot. Also, know the efficiency of self-ligating mechanics with its resulting freedom of movement.
 With this bracket system, there’s no need to settle for a non-fixed treatment alternative in cases where doing so could compromise treatment. Because we make this option readily available, it is rare that an esthetically demanding teen or adult patient will choose a labial option over lingual. Combine the indirect bonding setup and an efficient reliable bracket, there is no better time than now to incorporate lingual therapy into your practice.
With this bracket system, there’s no need to settle for a non-fixed treatment alternative in cases where doing so could compromise treatment. Because we make this option readily available, it is rare that an esthetically demanding teen or adult patient will choose a labial option over lingual. Combine the indirect bonding setup and an efficient reliable bracket, there is no better time than now to incorporate lingual therapy into your practice.
References
- AAO study finds adults are seeking orthodontic treatment in record numbers. Orthodontic Products. Published October 30, 2013. https://www.orthodonticproductsonline.com/2013/10/aao-study-finds-adults-are-seeking-orthodontic-treatment-in-record-numbers/. Accessed October 17, 2016.
- Scuzzo G, Takemoto K, Takemoto Y, Scuzzo G, Lombardo L. A new self-ligating lingual bracket with square slots. J Clin Orthod. 2011;45(12):682-690.
- Turnbull NR, Birnie DJ.Treatment efficiency of conventional vs self-ligating brackets: effects of archwire size and material. Am J Orthod Dentofacial Orthop. 2007;131(3):395-399.
- Chen SS, Greenlee GM, Kim JE, Smith CL, Huang GJ.Systematic review of self-ligating brackets. Am J Orthod Dentofacial Orthop. 2010;137 (6):726.e1-726.e18.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
