Dr. Bradford Edgren illustrates a case study with a new Herbst-type appliance
 Introduction
Introduction
Orthodontic treatment should be designed around the patient’s total dentofacial complex, including future dentofacial growth, rather than the narrower objective of treating just the teeth and/or the occlusion. Consequently, diagnosis, treatment planning, and management of Class II malocclusions can be difficult when extraction and surgical options are not viable/practical when fully evaluating the patient in all three dimensions: antero-posterior, transverse, and vertical.
[userloggedin]
Furthermore, when considering the importance of future growth, successful treatment may become daunting. This patient presented with just such a malocclusion.
 Distalization of the maxillary dentition can be difficult, but for this patient’s malocclusion, distalization of the posterior maxillary dentition would help in the resolution of her problems. The Liberty Bielle® is a Herbst-type appliance from Rocky Mountain Orthodontics (RMO) that can be directly attached to the archwires. Because it can be directly attached to the archwires, it can be used to distalize individual maxillary teeth, reducing the proclination of the mandibular incisors.
Distalization of the maxillary dentition can be difficult, but for this patient’s malocclusion, distalization of the posterior maxillary dentition would help in the resolution of her problems. The Liberty Bielle® is a Herbst-type appliance from Rocky Mountain Orthodontics (RMO) that can be directly attached to the archwires. Because it can be directly attached to the archwires, it can be used to distalize individual maxillary teeth, reducing the proclination of the mandibular incisors.
This patient presented as a new patient exam with her mother on December 3, 2008, as a healthy 12-year 2-month-old female. Her stated chief complaint was that she had dental crowding with not enough room for her maxillary canines and that she wanted her lower teeth straightened.
Diagnosis and etiology
Intraoral examination revealed a Class II malocclusion, a left maxillary lateral incisor crossbite, a left posterior crossbite, and impacted maxillary canines. Her overbite (OB) was 15% and overjet (OJ) was 2 mm. Significant arch length deficiencies were present in both dental arches with the maxillary arch length at -10 mm and the mandibular at -7 mm. The upper arch form was significantly tapered with an anterior maxillary constriction resulting in the impaction of the maxillary canines. There was a discrepancy in the dental midlines with the lower dental midline being 3 mm to the left of the already 1 mm left displaced upper dental midline (Figure 1).

 Clinical frontal evaluation demonstrated a mesofacial facial pattern with a sym-metrical and well-balanced facial pattern for the upper, middle, and lower facial heights. A facial asymmetry to the left was noted concomitant with the lower dental midline being displaced to the left 3 mm. Lateral evaluation displayed that the patient’s lips were significantly retrusive with a concave facial profile.
Clinical frontal evaluation demonstrated a mesofacial facial pattern with a sym-metrical and well-balanced facial pattern for the upper, middle, and lower facial heights. A facial asymmetry to the left was noted concomitant with the lower dental midline being displaced to the left 3 mm. Lateral evaluation displayed that the patient’s lips were significantly retrusive with a concave facial profile.
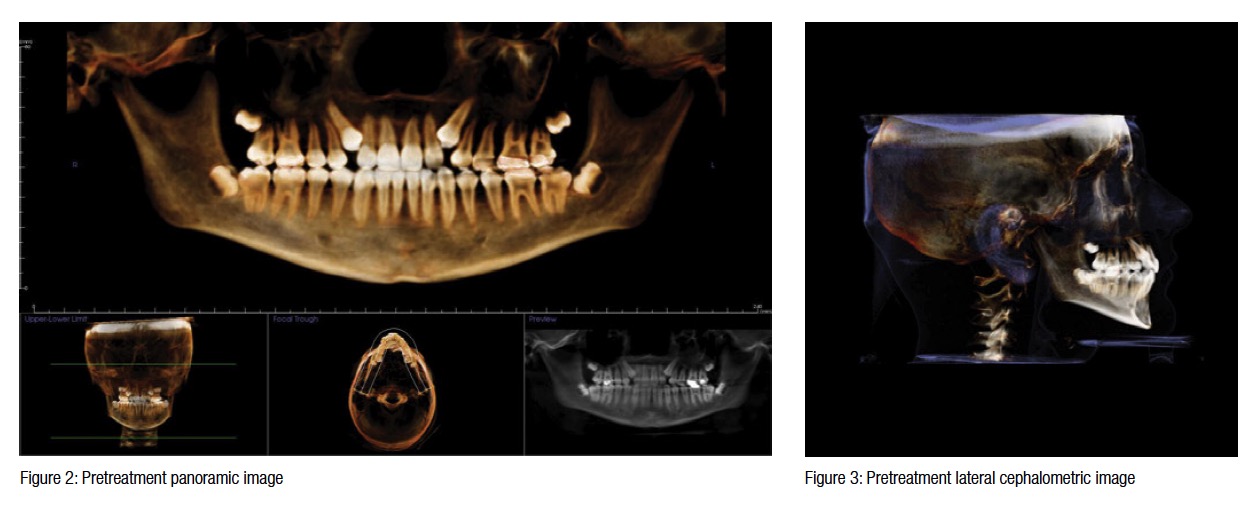
Radiographic evaluation of the panoramic image revealed bilaterally impacted maxillary canines and asymptomatic chronic sinusitis with inflammation in the left maxillary sinus. All four third molars were present and unerupted (Figure 2).
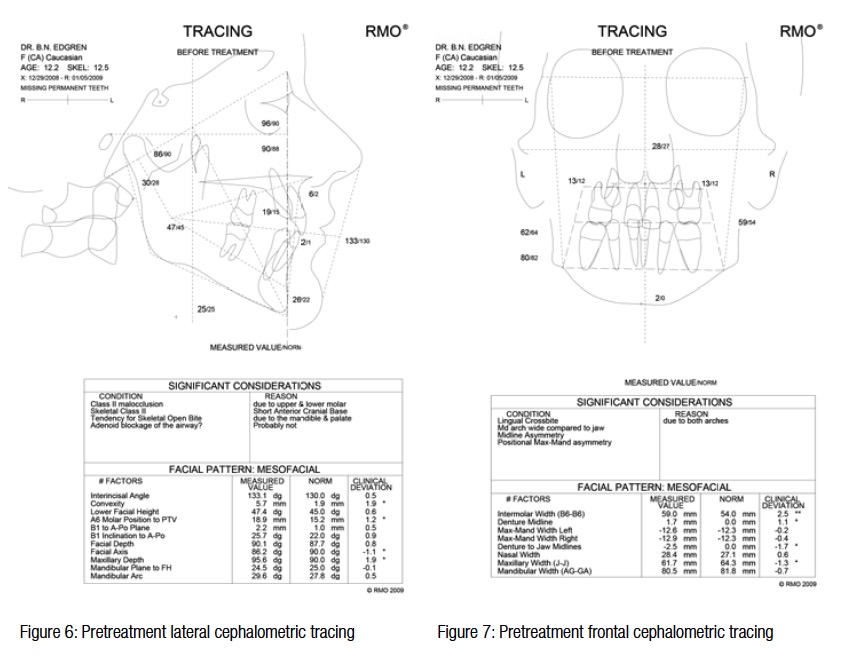
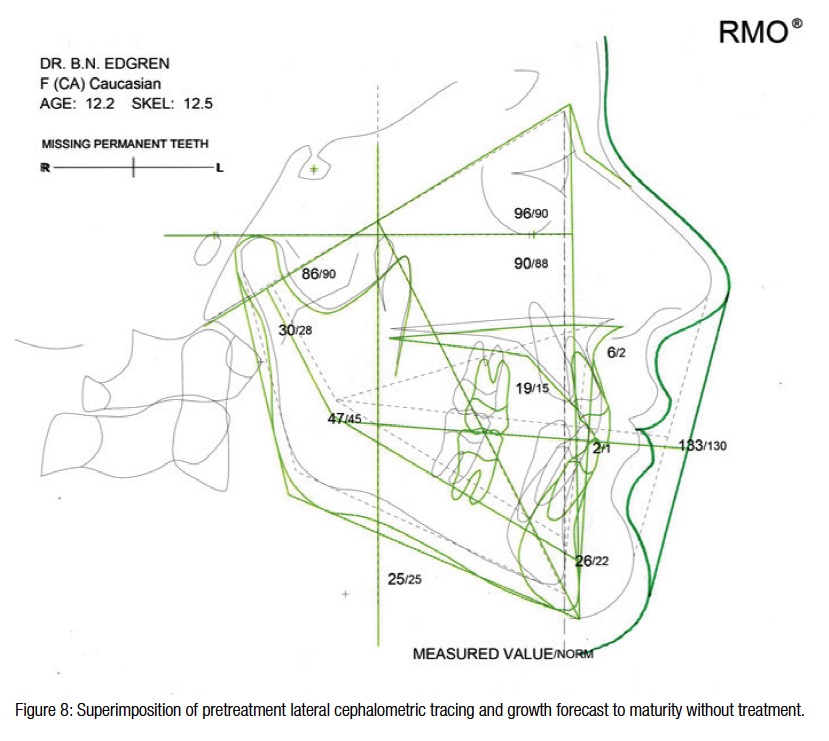
A Ricketts’ cephalometric evaluation by Rocky Mountain Orthodontics Data Services RMODS® revealed a Class II malocclusion due to both the maxillary and mandibular dentitions. A skeletal Class II component due to a short anterior cranial base and a tendency for a skeletal open bite was also present. Upper airway obstruction due to adenoid blockage was not likely. Frontal cephalometric analysis confirmed a lingual crossbite pattern due to both arches with the mandibular arch being wide compared to the mandible. The mandibular midline asymmetry was due to a left positional asymmetry of the mandible. Ricketts’ growth to maturity without orthodontic intervention revealed approximately 3 years of additional dento-facial growth (Figures 3-8).
Treatment summary
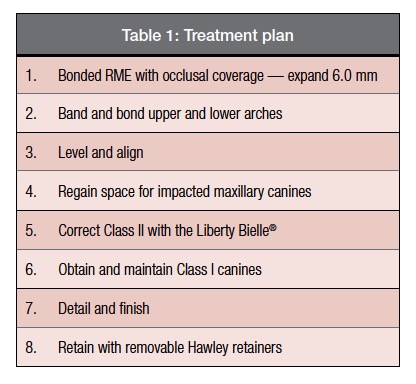
 Due to the retrusive lips and concave facial profile, a non-extraction treatment plan was recommended. Initial expansion of the maxilla with a bonded rapid palatal expander incorporating the first pre-
Due to the retrusive lips and concave facial profile, a non-extraction treatment plan was recommended. Initial expansion of the maxilla with a bonded rapid palatal expander incorporating the first pre-
molars, second premolars, and first maxillary molars was implemented to correct the left posterior lingual crossbite. After 2 weeks of single ¼ mm turns, one in the morning and one in the evening, a total of 6 mm of expansion and correction of the lingual crossbite was accomplished. Bonding of the upper incisors with RMO Minitaurus™ brackets, Andrew’s Rx, with molar tubes attached to the bonded expander at the level of the first premolars was performed 3 weeks later. The bonded expander was removed 7 months later after correction of the left maxillary lateral incisor crossbite. The remaining maxillary dentition and mandibular dentition were banded and bonded at that time. Leveling and aligning of the maxillary and mandibular dentitions continued for the next 21 months. During this period, space was regained for the natural eruption of impacted maxillary canines with the maxillary right canine being bonded 9 months and the maxillary left canine bonded 16 months after RME removal.
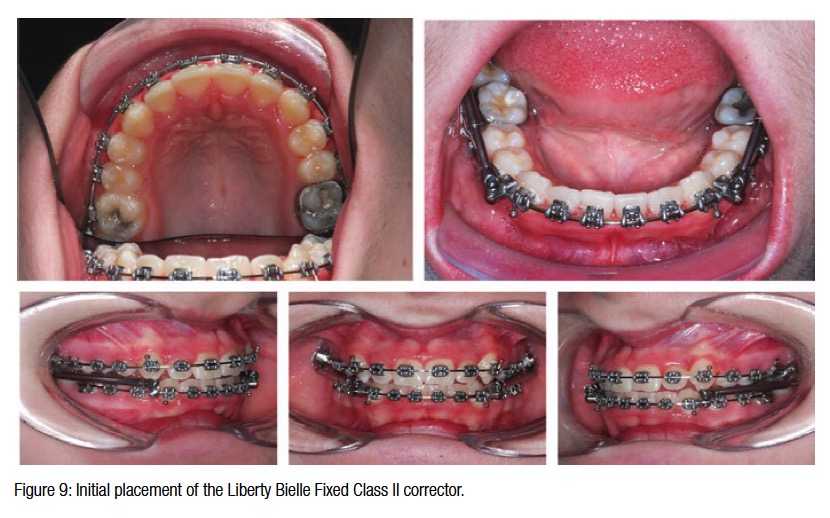
 After 27 months of treatment, the Liberty Bielle Class II corrector was placed (Figure 9). Note that the Liberty Bielle is placed mesially to the maxillary second molars. This placement provides initial distalization of the second molars with subsequent distalization of individual teeth of the maxillary dentition, minimizing protrusion of the mandibular incisors. This appliance placement also takes advantage of the remaining mandibular growth.
After 27 months of treatment, the Liberty Bielle Class II corrector was placed (Figure 9). Note that the Liberty Bielle is placed mesially to the maxillary second molars. This placement provides initial distalization of the second molars with subsequent distalization of individual teeth of the maxillary dentition, minimizing protrusion of the mandibular incisors. This appliance placement also takes advantage of the remaining mandibular growth.
 The Liberty Bielle was removed after 5 months of activation. Nine months of detailing and finishing was performed to solidify the Class II correction. A total of 41 months of treatment was necessary to accomplish a Class I mutually protected occlusion for this difficult case. Removable maxillary and mandibular Hawley retainers were fabricated and delivered 13 days after deband. The patient was instructed to wear the retainers 24 hours a day for the next 18 months and then at night indefinitely. Following deband, the patient was referred to an oral surgeon for removal of the impacted third molars. The third molars were extracted 1 month later.
The Liberty Bielle was removed after 5 months of activation. Nine months of detailing and finishing was performed to solidify the Class II correction. A total of 41 months of treatment was necessary to accomplish a Class I mutually protected occlusion for this difficult case. Removable maxillary and mandibular Hawley retainers were fabricated and delivered 13 days after deband. The patient was instructed to wear the retainers 24 hours a day for the next 18 months and then at night indefinitely. Following deband, the patient was referred to an oral surgeon for removal of the impacted third molars. The third molars were extracted 1 month later.
 Summary and conclusions
Summary and conclusions
This patient had an excellent result achieved with combined orthopedic and dental alveolar changes. Skeletal and dental treatment objectives were obtained through good mechanical control of the dentition and utilization of the remaining craniofacial growth. Expansion of the maxilla provided additional dentoalveolar width correcting the lingual crossbite and providing space for the natural eruption of the impacted maxillary canines. A nice Class I occlusal relationship, with a mutually protected occlusion, was established with appropriate overjet and overbite (Figure 10).
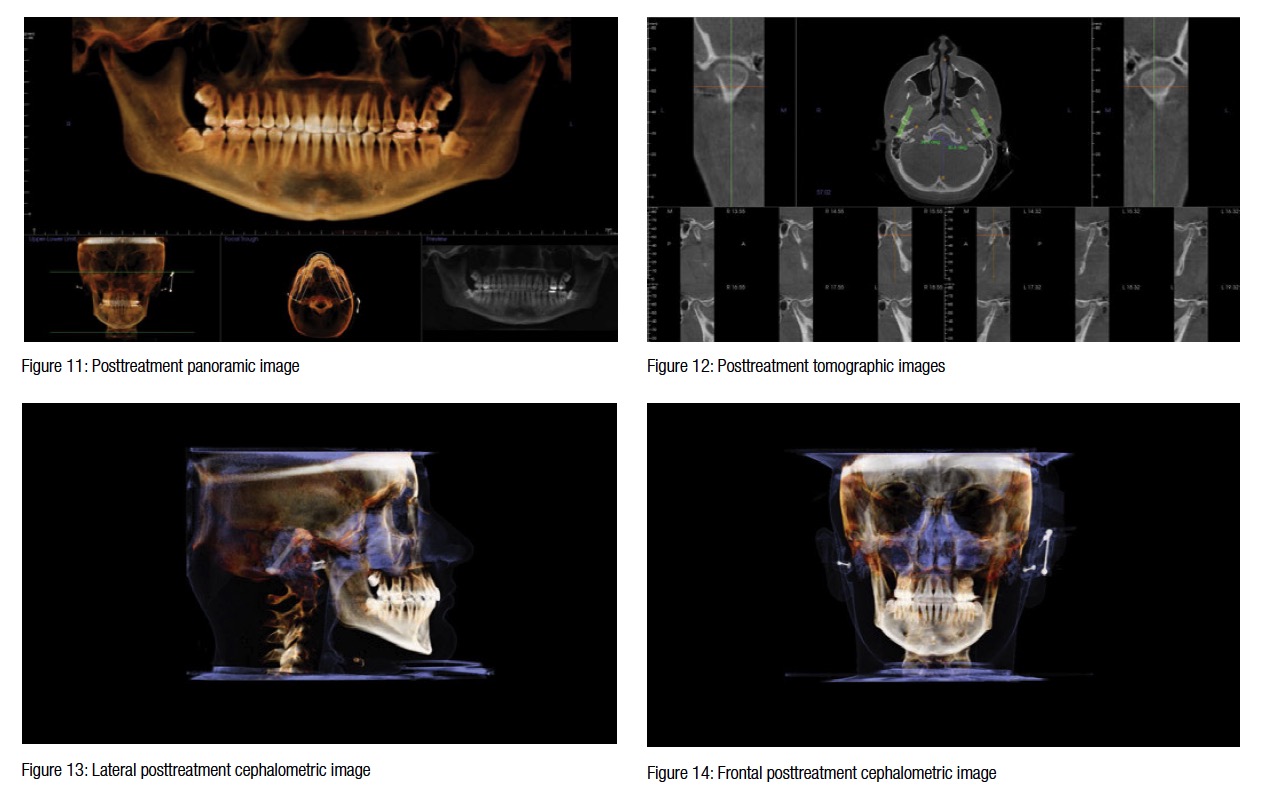
The posttreatment panoramic image displayed proper root parallelism and four impacted third molars. The left maxillary sinus displayed inflammation from chronic sinusitis (Figure 11). Tomography of the temporomandibular joints revealed that both condyles were well seated within their respective fossa (Figure 12).
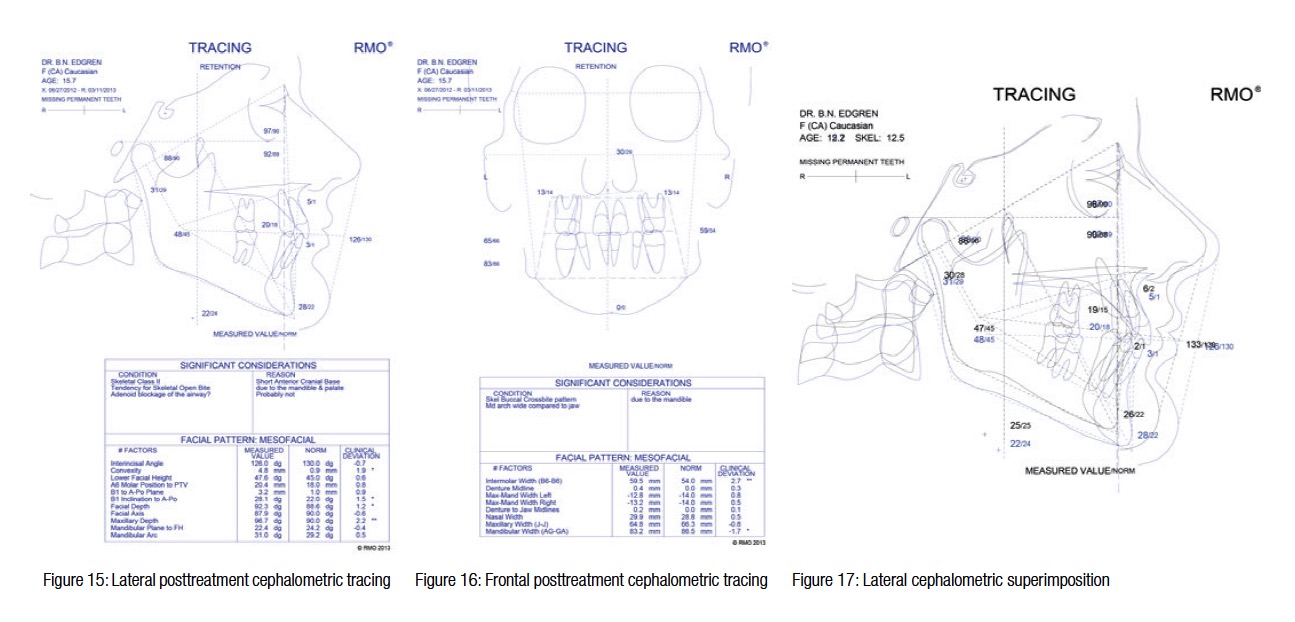
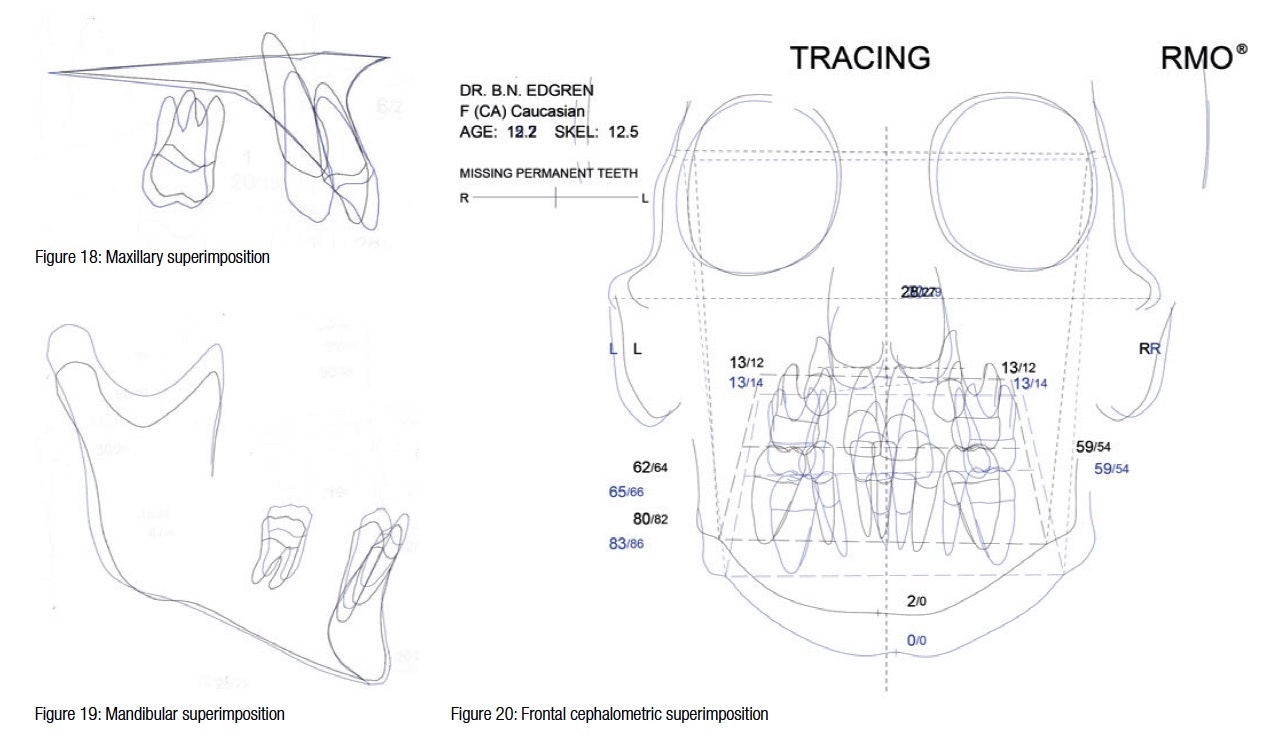
Retention cephalometric analysis revealed a Class I occlusion and resolution of the lingual crossbite (Figures 13-16). Lateral cephalometric superimposition of initial and retention cephalometric tracings demonstrated very good control of the lower incisor angulation (Figure 17). The mandibular incisor position was maintained with no additional proclination. The technique of placing the Liberty Bielle appliance just mesial of the maxillary second molars and the initial distalization of the second molars with subsequent distalization of the individual teeth of the maxillary dentition reduced the tendency for the proclination of the mandibular incisors typical of Class II correction appliances. Cephalometric superimposition of the maxilla confirmed distalization of the first molar as well as improvement in the angulation of the incisor (Figure 18). Superimposition of the mandible revealed mesial movement of the lower dentition concomitant with mandibular growth (Figure 19). Frontal cephalometric superimposition demonstrated an increase in maxillary width and an improvement in the mandibular asymmetry (Figure 20).
This new Herbst-type appliance can be used not only for orthopedic purposes but also for dental aveolar change with increased efficiency and improved results. It’s nice to have an appliance that can treat outside the box.
[/userloggedin]
[userloggedout][/userloggedout]
 Bradford Edgren, DDS, MS, earned both his Doctorate of Dental Surgery, as Valedictorian, and his Master of Science in Orthodontics from the University of Iowa, College of Dentistry. He is a Diplomate, American Board of Orthodontics, and a member of the Southwest Component of the Edward H. Angle Society. Dr. Edgren has presented nationally and internationally to numerous orthodontic groups on the importance of orthodontic diagnosis, early interceptive orthodontic treatment, CBCT, and upper airway obstruction. He has been published in AJO-DO, the American Journal of Dentistry, as well as other orthodontic publications. Dr. Edgren currently has a private practice in Greeley, Colorado. Disclosure: Currently, Dr. Edgren is not receiving compensation from RMO on this appliance.
Bradford Edgren, DDS, MS, earned both his Doctorate of Dental Surgery, as Valedictorian, and his Master of Science in Orthodontics from the University of Iowa, College of Dentistry. He is a Diplomate, American Board of Orthodontics, and a member of the Southwest Component of the Edward H. Angle Society. Dr. Edgren has presented nationally and internationally to numerous orthodontic groups on the importance of orthodontic diagnosis, early interceptive orthodontic treatment, CBCT, and upper airway obstruction. He has been published in AJO-DO, the American Journal of Dentistry, as well as other orthodontic publications. Dr. Edgren currently has a private practice in Greeley, Colorado. Disclosure: Currently, Dr. Edgren is not receiving compensation from RMO on this appliance.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
