Drs. Domingo Martin and Jorge Ayala illustrate treatment using the FACE concept of orthodontic treatment

In the September/October 2016 issue of Orthodontic Practice US, we introduced the FACE (Functional and Cosmetic Excellence) concept of orthodontic treatment and its importance in achieving function and esthetics. We also explained the treatment goals and the key factors that make up the goals.
[userloggedin]
After the introduction to the FACE treatment philosophy, we explained that the FACE Evolution bracket* was developed by some of the key members of the FACE group. This bracket was developed by clinicians for clinicians. In the article, we gave the many reasons for the development of a new bracket system. In retrospect, the main reason was the need for a bracket system that took function into account, and this is the first of its kind.
In the second part of the article, we will further explain the necessity for changing the original Roth prescription. The rationale for the many changes in the prescription makes sense to experienced clinicians. We also introduce the concept of “working tube,” something that many clinicians will like, and more importantly, the need for this type of bracket in our toolboxes. We also announced the “working bracket” and its multiples uses, and why we need this in many instances to obtain our functional and esthetic occlusal goals.
 Prescription for work and prescription for finish
Prescription for work and prescription for finish
FACE Evolution incorporates a new concept into orthodontic biomechanics: working prescription and finishing prescription. The work prescription consists of using specific tubes and brackets for their temporary use in certain situations with the purpose of attaining certain aims (Figure 11A).
The prescription for finish is obtained with the use of the standard FACE Evolution prescription — a good finish in a high percentage of cases — without needing to bend the arches. In some situations, because of minor anatomic variations, the necessary adjustments should be performed (Figure 11C).
Working tubes
 By varying the mesiodistal position of the tubes, we can modify the rotation values and the anchorage values to tackle cases of minimum, medium, and maximum anchorage. Therefore, the tube will have three vertical guides (Figure 12) that enable us to locate the tube more mesially for cases of maximum anchorage, or more distally, for cases of minimum anchorage, and a central framework for cases of medium anchorage and finishing stage. These guidelines will coincide with the main vestibular sulcus as indicated. Tubes with markings became available in 2016 (Figures 12A-12C).
By varying the mesiodistal position of the tubes, we can modify the rotation values and the anchorage values to tackle cases of minimum, medium, and maximum anchorage. Therefore, the tube will have three vertical guides (Figure 12) that enable us to locate the tube more mesially for cases of maximum anchorage, or more distally, for cases of minimum anchorage, and a central framework for cases of medium anchorage and finishing stage. These guidelines will coincide with the main vestibular sulcus as indicated. Tubes with markings became available in 2016 (Figures 12A-12C).
With the same tube, we can therefore attain three different anchorages (standard, +4°, and –4°), simply and efficiently; the necessary inventory is also simplified, so this is like having three different prescriptions in the same tube.
As its name indicates, the prescription for work is the one with which we can perform specific actions — for example, distalization or retrusion of the six anterosuperior teeth or mesialization of the posterior segments — by increasing or reducing the anchorage.
Once the required aim is obtained, in this case closure of the spaces, we will switch to the prescription for finish by positioning the tubes in the usual way.
Working brackets
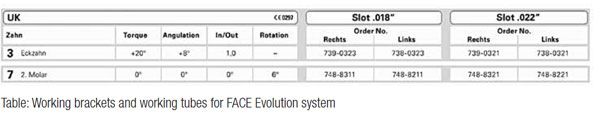
For cuspids, the working bracket with 20° positive torque will enable us to place these teeth in the required position to be subsequently replaced with the standard torque bracket or bracket with the final prescription.
For the mandible, the molar torque of –30° operates efficiently in most cases, although at times not in the case of second molars. Indeed, in a lower percentage of cases, the second lower molar “tips” toward the lingual region, especially in those cases with an accentuated curve of Spee.
The explanation appears to reside in the fact that when attempting to access these molars and given that the apices are in relation to the compact bone of the external oblique line, this undesired effect would occur, which is difficult to resolve. Therefore, FACE Evolution proposes a working tube with 0° of torque, which once the molar torque has been corrected, should be replaced with the prescription’s standard finishing tube.
Active system and hybrid system
It is difficult to come to an agreement in regard to which self-ligating system has more advantages and less disadvantages. Various papers conclude that sliding mechanics are favored for the use of passive self-ligating brackets, but control of the root position could be comprised. They also confirm that the sliding resistance (SR) is necessary when we have to produce torque and correctly position the root for correct finishing.
The wish to minimize resistance to friction should be moderated because of the need to control movement of the teeth. In the new FACE Evolution, we have opted to take the advantages of both parts by means of two versions: the active system and the hybrid system.
The active system gives us more control: During subsequent treatment stages, sliding resistance (SR) increases along with the size of the arch. This provides better three-dimensional control and fills the sulcus to produce a torque force that correctly positions the root and the crown.
The hybrid system provides the clinician with the best combination of low friction and control, especially in cases with extractions. A recent study performed by Dr. Douglas Knight on 400 finished patients concluded that the duration of treatment and number of appointments of 200 patients treated with the hybrid system reduced by 15%.
Clinical cases
Case 1 by Dr. Domingo Martín
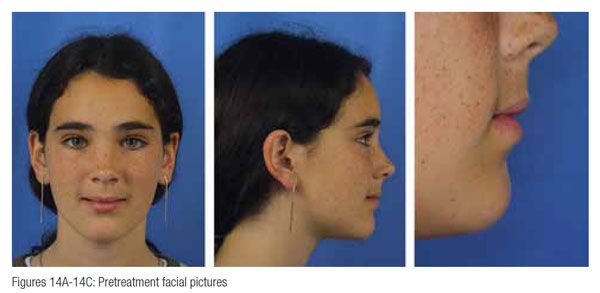
(Figures 14–22)
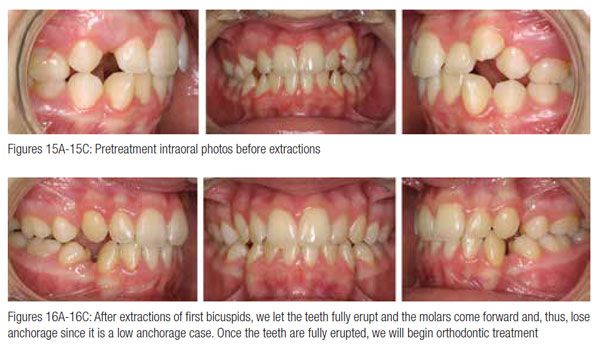
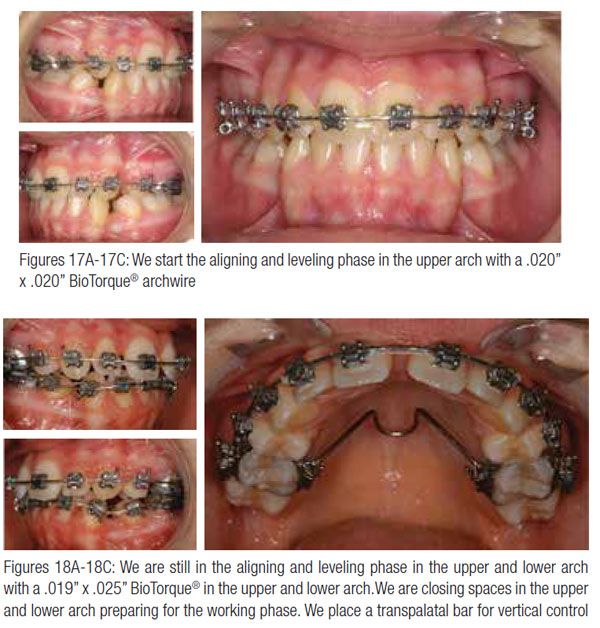
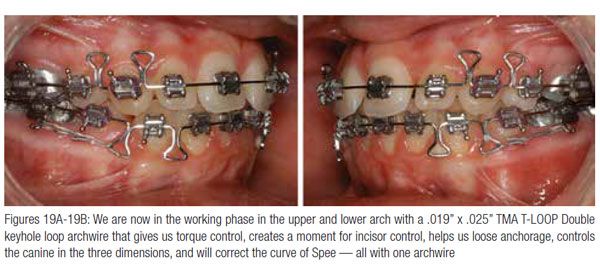
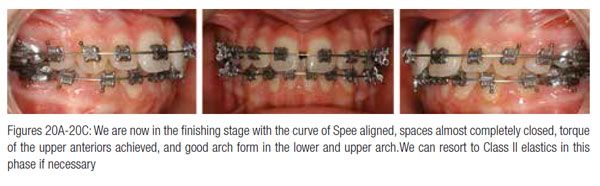
A 13-year-old female presented with severe space deficiency, and with her skeletal anatomy, we decided to extract four bicuspids and close spaces, maintaining her upper teeth forward, not retruding the upper lips, and obtaining a good functional occlusion.


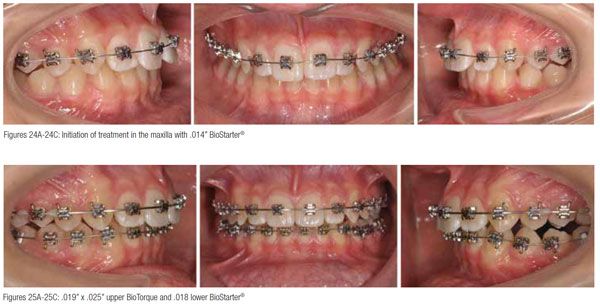
Case 2 by Dr. Jorge Ayala (Figures 23–27)

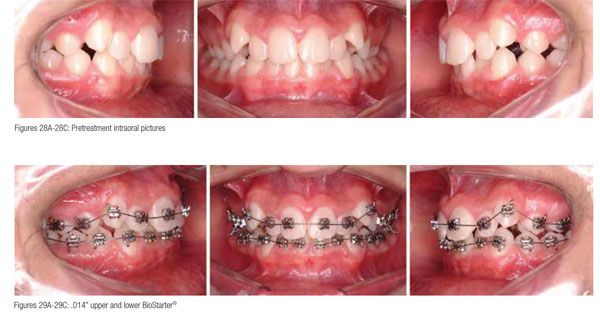
 Case 3 by Dr. Jorge Ayala (Figures 28–31)
Case 3 by Dr. Jorge Ayala (Figures 28–31)
 * Fa. FORESTADENT
* Fa. FORESTADENT
 Dr. Domingo Martin has a BA from the University of Southern California and an MD and DDS from the University of the Basque Country in Spain. He also earned a Master in Orthodontics from the University of Valencia in Spain. He has a diploma in orthodontics by the FACE/Roth Williams Center for Functional Occlusion and has postgraduate work in Bioesthetic Dentistry from the OBI Foundation for Bioesthetic Dentistry. Dr. Martin gives courses and conferences all over the world, and he has a private practice limited to orthodontics in San Sebastián, Spain. He is also a FACE Member.
Dr. Domingo Martin has a BA from the University of Southern California and an MD and DDS from the University of the Basque Country in Spain. He also earned a Master in Orthodontics from the University of Valencia in Spain. He has a diploma in orthodontics by the FACE/Roth Williams Center for Functional Occlusion and has postgraduate work in Bioesthetic Dentistry from the OBI Foundation for Bioesthetic Dentistry. Dr. Martin gives courses and conferences all over the world, and he has a private practice limited to orthodontics in San Sebastián, Spain. He is also a FACE Member.
Dr. Jorge Ayala has a medical degree from the University of Chile with a specialty in Orthodontics and Maxillar Orthopedics from the University of Chile. He is Director of the FACE/Roth Williams Center for Functional Occlusion from Latinoamérica and a professor of the FACE/Roth Williams Center for Functional Occlusion in California. He runs a private practice limited to orthodontics in Santiago de Chile. He is the author of numerous articles and publications and speaker at national and international courses and conferences.
Disclosure: Drs. Martin and Ayala are consultants for Forestadent.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
