Last summer, Orthodontic Practice US and Propel Orthodontics partnered to publish results from The Propel Clinical Case Challenge — “Bring Us Your Most Challenging Cases, and We’ll Bring You the Solution.” The following participating doctors are representative of the dramatic results that orthodontists can achieve.
Weddings and Propel —
An excellent treatment option
Propel is an excellent tool to meet wedding date goals without compromising treatment outcomes.
[userloggedin]
Patient diagnosis and treatment goals
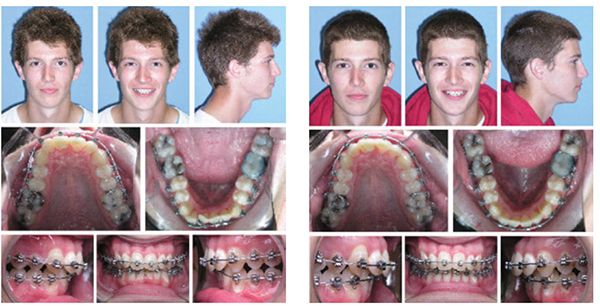
Kerry, a 25-year-old female, presented in July 2014 with Class I moderate crowding, narrow arches, and anterior open-bite tendency with a high mandibular plane angle. Treatment plan included non-extraction, upper clear Damon® brackets, and Damon Insignia brackets on the lower arch. In addition, posterior bite turbos were placed along with daily squeeze exercises to assist bite closing. Initial treatment time was estimated at 22-24 months without Propel. Brackets were placed.


December 2014: Kerry’s wedding was planned for September 2015. She requested to reduce the 22-24 month treatment to 15 months.
March 2, 2015: As a wedding gift, our office offered to add complimentary Propel procedures. I performed interproximal single Propel perforations from the first molar to the first molar in both the upper and lower arches. The posterior perforations were 5 mm, and the anterior perforations were 3 mm.

May 27, 2015: A second Propel procedure was performed at 12 weeks with the same molar-to-molar interproximal single perforations in both arches.
September 10, 2015: Treatment was successfully completed in 15 months with the assistance of Propel. Retention included a clear Essix retainer with full-time wear for the first month, followed by nighttime wear for lifetime. We also placed an upper 2-2 bonded retainer and lower 3-3 bonded retainer. Minimal incisal edge bonding was also added.
Dr. McGill shared her thoughts: “We choose to use Propel proactively and offer it in our consultations with adults and teens who are not on anti-steroidal medications. It is also a great option to use in midtreatment to help progression of stubborn tooth movements.”
A case in progress
Read about the progression of Dr. Shaw’s challenging case.
Patient diagnosis and treatment goals
Jeremiah is a 21-year-old male concerned with severe crowding and overbite.
He presented with a Class II Division 2 malocclusion, severe crowding, and a 100% overbite. The incisors were very linguoverted due to an extreme curve of Spee in the lower arch. Treatment was planned non-extraction to flare the upper and lower incisors, intrude the lower incisors to open the bite, and utilize Class II elastics to correct the overjet. With compliance, treatment was anticipated to take 22 months.
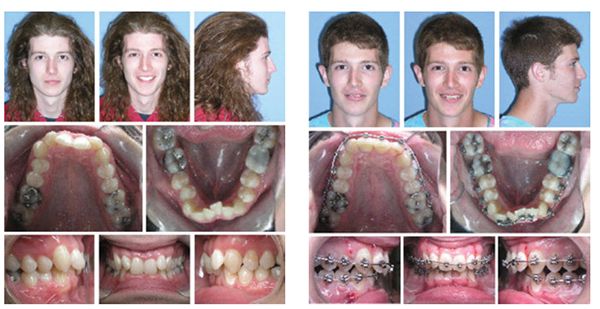

April 2, 2015: Full upper and lower SPEED brackets were placed 7-7. Archwires were fully engaged in all the brackets with an additional open coil to make space for the lower right central incisor. Bite turbos were placed on the lingual of the upper centrals to protect the lower braces and help intrude the lower incisors.
June 18, 2015: Jeremiah came in to continue opening space for the lower central. Because of the extensive amount of movement remaining, we made Jeremiah our first unplanned Propel patient. Perforations were made with the Propel Excellerator interproximally from the distal of the cuspids forward according to the standard protocol of two to three vertical perforations. In hindsight, I probably should have gone at least to the distal of the second bicuspids. Post Propel, Jeremiah experienced some short-term numbness and tenderness but felt fine after a few hours.
July 16, 2015: There was great progress in the alignment and rotations and significant leveling of the lower arch. The open coil was compressed to help rotate the lower right central incisor.
August 3, 2015: Jeremiah returned to have a bracket rebounded, and we were actually able to reengage the central incisor into the archwire. Typically, we’d need 6-8 weeks to get enough movement to engage this tooth, but it was ready 18 days after activating the coil spring.
September 22, 2015: All the rotations were fully corrected, and overbite was reduced to 40% during these 3 months! We inserted 19 x 25 finishing wires with all brackets easily engaged. Class II elastics were started on these wires to begin reducing the overjet that had developed from flaring the upper incisors.
November 12, 2015: (7 months after treatment initiated) A 19 x 25 TMA was placed in the lower arch. Overbite is ideal; lower arch is level. We engaged these finishing wires 5 months after accelerating with Propel. Originally, we had hoped to be able to insert these after 1 year.
January 21, 2016: We removed his bite turbos since the overbite was completely corrected, and the incisal edges were cosmetically recontoured. We continued Class II elastics on the right side only to coordinate the midlines. Final detailing was started. His treatment progress continues to be exceptional!
Dr. Shaw shared his thoughts about the progress results: “I wasn’t sure what to expect even after extensive research. I was astonished by the incredible tooth movement we achieved in a short period of time.”
Missing bicuspid site closure?
Closing large extraction sites (or in this case congenitally missing teeth) can present extended treatment times and difficult mechanics. Dr. Yarascavitch initiated Propel and mini-screw anchorage with amazing results.
Patient diagnosis and treatment goals
Virginia’s consultation and treatment started in March 2014 at age 14. She had a Class II Division 1 malocclusion with a retrognathic facial type and long lower face height, mild upper and lower crowding, minimal overbite and overjet, multiple retained primary teeth, including primary second molars, missing adult second premolars, lingually ectopic lower adult canines, and an upper-right crossbite.
My initial plan was full fixed orthodontics, trimming the lower primary molars to smaller proportions and keeping them as long as possible eventually replacing with implants. Early in treatment, the primary molars were creating difficulty in establishing a good occlusion. Virginia did not want implants and wished to close spaces. After much deliberation with Virginia and her primary dentist, lower second primary molars were removed December 2014.
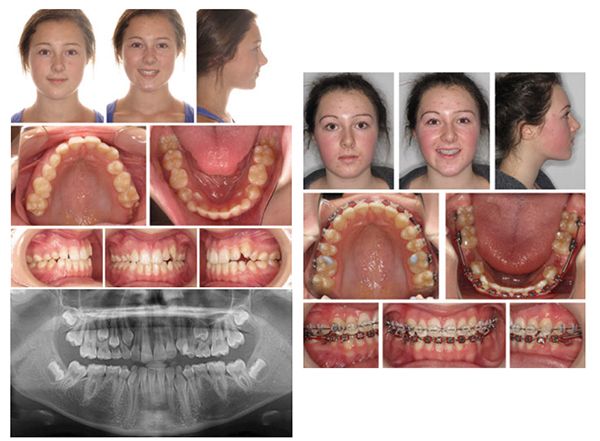


January 7, 2015: Virginia had the lower second primary retained molars recently removed. After 10 months, I was losing upper and lower incisor torque using conventional mechanics and Class III elastics. I planned to place lower TADs to help protract molars, correct incisor torque, and re-establish normal overjet.
October 1, 2015: Virginia expressed frustration regarding treatment time, and I told her we’d try Propel. There had been some slow space closure with mini-screws. I placed a single perforation mesial and distal to the lower first molars on the buccal alveolus. Space-closing coils were placed from the indirectly screw-anchored lower premolars to the first molars, and light Class III elastics were used to support movement along a rounded 17 x 25 SS archwire.
October 28, 2015: Four weeks after Propel, the lower-right first molar moved 2 mm mesial. The lower-left first molar moved 1.5 mm mesial; the lower-right second molar moved 2 mm; and the lower-left second molar moved 1.5 mm. Gingiva was healthy, and no abnormal discomfort was noted.
December 1, 2015: Eight weeks after the first Propel procedure, the space mesial to the lower-left first molar was eliminated, and the lower-right and left second molars protracted a large distance. The lower-right first molar moved an additional 1 mm; and the lower-left first molar moved 1.5 mm. Lower second molars continued to move mesially (1 mm right; 1.5 mm left). The panoramic shows bone remodeling distal to the lower first molars, and gingival attachment was healthy. A second Propel procedure was performed just mesial to the lower 7’s.
January 2016 Update: The lower first molars were protracted successfully, and the lower second molars were simultaneously protracted more than 4 mm over the course of 12 weeks. Only minor spaces remain, and I expect that in February 2015, all lower spaces will be closed. Virginia’s case will only require minor finishing/settling, and she’s delighted to be done ahead of schedule.
Dr. Yarascavitch noted, “I have done more cases for ‘problem teeth,’ but I hope to start some full Propel Micro-osteoperforation (MOP) cases for accelerated overall treatment from the start as a general protocol.”
[/userloggedin]
[userloggedout][/userloggedout]
 Jean Seibold McGill, DDS, MS, PC
Jean Seibold McGill, DDS, MS, PC
Easton, Pennsylvania
Dr. McGill is a graduate of Northwestern University Dental School, completed her orthodontic residency at the University of Michigan, and is a Diplomate of the American Board of Orthodontics. She has been in private practice since 1995, is one of the top providers of Insignia in the United States, and lectures to other orthodontists on the Insignia System. She currently serves as a Clinical Assistant Professor, Department of Orthodontics, Rutgers School of Dental Medicine.
 Randall L. Shaw, DDS, MS
Randall L. Shaw, DDS, MS
Livonia, Michigan
Dr. Shaw received his DDS degree from the University of Michigan. He completed an Orthodontic Residency at Washington University in St. Louis. He serves as faculty and a Clinical Advisory Board member for suresmile® and is in full-time private practice in Livonia at Drs. Shaw & Jane Orthodontics.
 Marc Yarascavitch, DDS
Marc Yarascavitch, DDS
Huntsville, Ontario
Dr. Yarascavitch completed his dental degree at the University of Toronto in 2008 and his master’s degree in 2010 in the Graduate Orthodontics Program. He has successfully completed his orthodontic specialty examination and practices orthodontics in Muskoka, Ontario.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
