Dr. Rohit C.L. Sachdeva reviews the benefits of suresmile
An all-digital CAD/CAM solution — suresmile® — offers the orthodontist a total solution for managing patient care.1 This technology has evolved over the past 2 decades and enables the doctor to perform 3D-image guided diagnosis, care planning, and also the ability to design personalized therapeutic devices, including indirect bonding trays,2 aligners,3 and archwires. suresmile’s value proposition to the clinician is based upon shorter treatment times and better patient outcomes. This is achieved by providing tools that enable the management of reactive care processes during orthodontic care.1
 The aim of this article is to present a summary of the results of various studies that have been conducted over the last decade to understand both the efficiency and effectiveness of suresmile. Furthermore, the present discussion is limited to reporting treatment results in response to the use of suresmile® customized archwires.
The aim of this article is to present a summary of the results of various studies that have been conducted over the last decade to understand both the efficiency and effectiveness of suresmile. Furthermore, the present discussion is limited to reporting treatment results in response to the use of suresmile® customized archwires.
suresmile® efficiency and quality
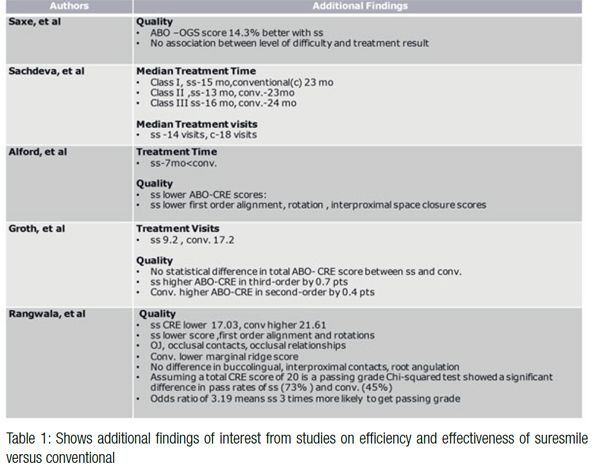
To date, five clinical studies4-8 have been conducted to evaluate suresmile efficiency and quality of treatment outcomes. The results are summarized in Figures 1 and 2 and Table 1. Although these studies are retrospective in nature and are limited in their design and methodology, it should be noted that the general trend of the results of these studies strongly suggest that treatment time with suresmile is reduced between 25%-40%. Furthermore, the treatment outcomes measured in three studies using the ABO-OGS and ABO-CRE9 indicate an improvement in treatment outcomes in a range of 10%-18%.

Accuracy of suresmile
The promise of suresmile technology is based upon a “What you see is what you get” user interface. This means that the design of the 3D virtual target setup provides the input for the personalized archwire, which in turn drives the correction of the malocclusion to its final position — i.e., the preplanned target state (Figure 3). Under the ideal circumstances, the final outcome should provide a 100% match against the virtual target setup. Therefore, a number of investigations7-9 have been conducted to study the accuracy of the final treatment outcome against the virtual target setup.
 Larson, et al.,10 and Müller-Hartwich, et al.,11 used “best fit” superimposition techniques of scanned final models of dental casts against the virtual target setup to evaluate tooth positional discrepancies in all three planes of space. Larson, et al.,10 studied a sample size of 23 patients treated with suresmile.
Larson, et al.,10 and Müller-Hartwich, et al.,11 used “best fit” superimposition techniques of scanned final models of dental casts against the virtual target setup to evaluate tooth positional discrepancies in all three planes of space. Larson, et al.,10 studied a sample size of 23 patients treated with suresmile.
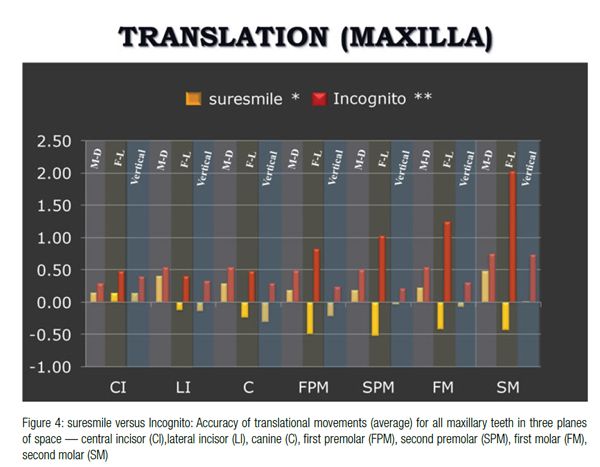
 They arbitrarily defined translational and rotational discrepancies between the final results and the virtual target setup of 0.5 mm and 2˚ for final tooth position as being clinically ”ideal.” Based upon their definition of the ideal, they found that the mesio-distal positions of all teeth except for the lateral incisors and second molars were on target. When considering the buccal (facial)-lingual tooth positions, they found that all teeth except for the maxillary central incisors, premolars, and molars, and mandibular incisors and second molars met their conditional standards of “ideal.” Vertical tooth positions were clinically ideal for all teeth except mandibular second molars. Larson, et al.,10 also found that crown torque, tip, and rotation discrepancies did not meet their standard for “clinically ideal.” The exceptions were for crown torque on mandibular second premolars and crown tip of mandibular second premolars and first molars. A summary of the results of their study is shown in Figures 4, 5, 6, and 7.
They arbitrarily defined translational and rotational discrepancies between the final results and the virtual target setup of 0.5 mm and 2˚ for final tooth position as being clinically ”ideal.” Based upon their definition of the ideal, they found that the mesio-distal positions of all teeth except for the lateral incisors and second molars were on target. When considering the buccal (facial)-lingual tooth positions, they found that all teeth except for the maxillary central incisors, premolars, and molars, and mandibular incisors and second molars met their conditional standards of “ideal.” Vertical tooth positions were clinically ideal for all teeth except mandibular second molars. Larson, et al.,10 also found that crown torque, tip, and rotation discrepancies did not meet their standard for “clinically ideal.” The exceptions were for crown torque on mandibular second premolars and crown tip of mandibular second premolars and first molars. A summary of the results of their study is shown in Figures 4, 5, 6, and 7.
 Müller-Hartwich, et al.,11 studied 26 patients and found that the median deviations for translational tooth movements were 0.19 mm – 0.21 mm and for rotational 1.77°–3.04°. They noted that the anterior teeth more precisely matched the virtual planned (target) position than the posterior teeth.
Müller-Hartwich, et al.,11 studied 26 patients and found that the median deviations for translational tooth movements were 0.19 mm – 0.21 mm and for rotational 1.77°–3.04°. They noted that the anterior teeth more precisely matched the virtual planned (target) position than the posterior teeth.
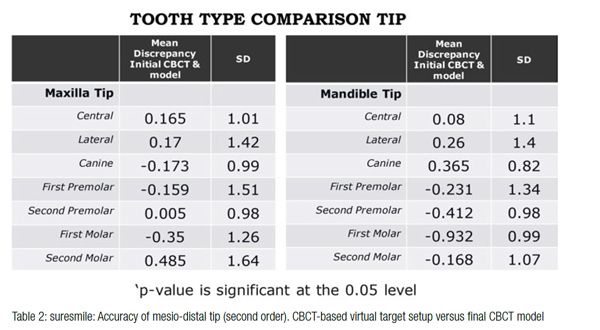 Smith12 evaluated the mesio-distal tip and facio-lingual torque outcomes on 40 consecutively treated patients by a single operator with suresmile. Final CBCT images were evaluated against the virtual target setup using “best fit” superimposition. He found that the overall mean discrepancy of the SS target models to the outcome CBCT were within ±2.5˚ and generally speaking were beyond the ±2.5˚ for the maxillary and mandibular second molars for tip, and the maxillary second molar and mandibular central and lateral for torque. Also, second-order outcomes were closer to target than torque outcomes for most tooth types. Of interest was that the mandibular teeth in general showed deviations greater than 2.5˚ of the plan. Table 2 provides a summary of the results of this study.
Smith12 evaluated the mesio-distal tip and facio-lingual torque outcomes on 40 consecutively treated patients by a single operator with suresmile. Final CBCT images were evaluated against the virtual target setup using “best fit” superimposition. He found that the overall mean discrepancy of the SS target models to the outcome CBCT were within ±2.5˚ and generally speaking were beyond the ±2.5˚ for the maxillary and mandibular second molars for tip, and the maxillary second molar and mandibular central and lateral for torque. Also, second-order outcomes were closer to target than torque outcomes for most tooth types. Of interest was that the mandibular teeth in general showed deviations greater than 2.5˚ of the plan. Table 2 provides a summary of the results of this study.
 Discussion and conclusions
Discussion and conclusions
 Discussion and conclusions
Discussion and conclusionsEfficiency and effectiveness
Current research is a first step in demonstrating the efficiency and effectiveness of suresmile. Rangawala,7 using a Chi-squared test and assuming a passing ABO-CRE score of 20, demonstrated a significant difference in pass rates for suresmile® (73% ) versus conventional treatment (45%). Expressed in terms of an odds ratio, this investigator suggested that patients treated with suresmile were 3 times more likely to achieve an ABO-CRE passing grade than those treated with conventional treatment.
A valid concern to the reader should be some of the studies presented were based on a limited patient sample and could be suspect to selection bias. However, it is important to note that the study by Sachdeva, et al., was based on a study population of 9,350 suresmile and 2,945 conventionally treated patients from 142 practices nationwide. These records were gathered from the suresmile database with the doctors’ approval. Furthermore, the doctors had no input in their selection. By the sheer volume of the patients studied and the number of practices represented, little opportunity for patient selection bias presented itself. In fact to this day, this study represents the largest-ever sample of patients studied to determine treatment efficiency of competing orthodontic treatments. The results of this study may be considered more compelling.
The studies presented here are a first step in better understanding the benefits of suresmile. Future studies from multiple academic/research centers with better designed methodologies are needed to further clarify suresmile’s impact on treatment outcomes.
As alluded to earlier, suresmile studies on efficiency and effectiveness are entirely based on the use of the customized archwires to deliver the target outcome. The question that remains unanswered to this day is whether the addition of customized brackets and indirect bonding may contribute to further gains in efficiency and effectiveness in patient care.
A recent study by Brown, et al., sheds some light on this question. They investigated the clinical effectiveness and efficiency of three different appliance systems. Three patient groups were selected and treated as follows:
- Group 1 was treated with CAD/CAM-customized orthodontic appliances (i.e., brackets, indirect bonding trays, and archwires were all customized).
- Group 2 was treated with direct techniques.
- Group 3 was treated with indirect bonded techniques.
The two latter groups used, “off-the-shelf” orthodontic brackets. Patients treated with the fully customized appliance systems demonstrated the shortest treatment time of 13.8 ±3.4 months. They found the total treatment time for the CAD/CAM group was on average 8 months shorter than for the direct bonded group, and more importantly, only about 3 months shorter than for the indirect bonded group. Furthermore, they found no statistically significant differences between the three treatment groups (P = 0.13) in terms of ABO-CRE scores. These results are very interesting from a clinical vantage point and underscore the importance of initiating in-depth studies to better understand which elements of CAD/CAM-generated appliances truly add value to patient care and the clinical practice. Is it the customized archwire, brackets, or the indirect bonding tray?
Furthermore, it raises the question of whether a CAD/CAM-customized indirect bonding tray has merit over an analog manufactured tray, or can just processing improvement through better planning mitigate the need for elaborate technology?
Accuracy
Studies presented in this article suggest that with suresmile, translational movements in 3D space can be achieved within ±0.5 mm and rotational movements (torque, tip, etc.) within 2.5˚ of the plan.
However, the results of these investigations also indicate that accuracy is diminished in the first and second molar region. A host of reasons may contribute to these discrepancies in the posterior region. These may include the use of auxiliaries, e.g., elastics, the slot archwire slop, and what I call clinical-virtual setup dissonance. This phenomenon is a result of a doctor’s overconfidence in achieving a desired outcome by planning tooth position on a virtual setup that cannot possibly be achieved biologically — simply put, unreasonable treatment goals.
For comparison purposes I have also included accuracy studies conducted by Grauer and Proffit11 on the Incognito® system for lingual orthodontic care (Figures 4-7). This system uses a platform similar to that of suresmile. The accuracy results on Incognito are based on the use of the customized bracket, indirect bonding tray, and archwire. The comparative data certainly suggests the relatively superior performance of suresmile in comparison to Incognito.
Furthermore clinicians need to be cognizant of the fact that the accuracy of a single-tooth position does not reflect upon its relative position to an adjacent tooth in an arch that determines the “fit and the look of the dentition.” To better understand this issue, let us consider the example of an upper right incisor and its neighboring tooth, the left central incisor. Let us also postulate that each of these teeth can be positioned independently within a target of ±0.5 mm in the vertical direction. As a result, there is a possibility that at the culmination of treatment, one of the incisors may be intruded by 0.5 mm, while its neighbor may be extruded by the same amount. This would result in a relative vertical discrepancy of 1 mm between the teeth, which by all standards would be considered clinically unacceptable. And herein lies the enigma in relying on the accuracy of single-tooth positions in determining the merit of a technology.
To gain better understanding of the quality of treatment outcome, investigators need to measure both tooth position accuracy in conjunction with the ABO-CRE scores for the population sample under study. In addition, better methodologies to evaluate tooth-position accuracy need to be developed. Currently, the best fit superimposition techniques used rely upon internal references. This results in an “averaging effect,” which leads to both false positive and negative results for the displacement measures.
As more studies to understand accuracy of the virtual target setup emerge, it is important that the clinical and academic community work together to establish some conditional standards for both the accuracy of tooth modeling and target response. If not, we will in time fall into the abyss of competing products with little understanding of their performance, just as we currently do with brackets whose prescriptions and slot tolerances remain unchecked. In fact even to this day, scientific evidence has yet to validate either the efficiency or effectiveness of the straightwire against standard edgewise therapy. Yet it has become the defacto gold standard for fixed appliance therapy. Maybe we are entrapped with the metaphor of the “Emperor’s New Clothes” when it comes to the straightwire appliance.
A time for reflection
“Magic mirror, on the wall, who is the fairest of them all?” — Evil Queen in “Snow White and the Seven Dwarfs”
I have been very fortunate to have been directly involved in the development of suresmile®. Furthermore, over nearly the past 20 years, I have had the opportunity to serve well over 12,000 patients in multiple practices worldwide. Therefore, I feel reasonably qualified to share some of my practical learning in the deployment and use of this system in the practice.
“The first rule of any technology used in a business is that automation applied to an efficient operation will magnify the efficiency. The second is that automation applied to an inefficient operation will magnify the inefficiency.” — Bill Gates
I do not believe that this technology or others similar to it have any value unless the clinician has a succinct answer to the following questions: “What is the problem I face in the care of my patients (in other words finding the problem first), and why?” and “How can the technology solution help?” This requires deep self-reflection, which is painful. Without the answer to this question, one is liable to fall into the trappings of “solutioneering.”
“Most of the problems in life are because of two reasons: We act without thinking, or we keep thinking without acting.” — Unknown
One should resist the temptation of jumping onto the technology bandwagon before making a needs assessment.
“The real problem is not whether machines think but whether men do.” — B. F. Skinner
The notion that “smartness” or “intelligence” is embedded in the technology is far from the truth. In other words, this technology just as all others does not offer the holy grail of effortless “push button,” “cruise control” orthodontics.
“Observe, record, tabulate, communicate. Use your five senses. Learn to see, learn to hear, learn to feel, learn to smell, and know that by practice alone, you can become expert.” — William Osler
Proper diagnosis, planning and appropriate patient management remain the bedrock of clinical skills required to achieve desirable treatment outcomes. suresmile technology relies on human cognition as input to achieve its promise of performance and reliability.
“Every person is in certain respects like all other people, like some other people, and like no other person.” — Clyde Kluckhohn and Henry A. Murray, Personality in Nature, Culture, and Society
Yes, this technology is unique in that it offers a plethora of tool sets that enable computer-aided planning, interactive communication, and computer-aided manufacturing of appliances, such as customized archwires for labial and lingual orthodontics, indirect bonding trays, and aligners. The skill the clinician needs to develop is to recognize where the value of each of this offerings lies for a particular patient and intent. To believe that there is a one-way approach in successfully using this technology for all patients is unreasonable and unrealistic.
“Plans are nothing; planning is every-thing.” — Philip Kotler
“We are what we repeatedly do. Excellence, then, is not an act, but a habit.” — Aristotle
I personally believe that the value of this technology cannot be fully extracted and provide meaningful care for a patient without developing the primary skill set for 3D design and planning. This task cannot be delegated and requires perseverance by the clinician through deliberate practice to achieve expertise. And this is where the enigma lies for the busy clinician —finding the time to learn and reflect. Change in habits is difficult!
“A superior leader is a person who can bring ordinary people together to achieve extraordinary results.” — Unknown
“What gets measured gets improved.” — Peter Drucker
Success in the use of such technologies requires a sincere effort by the leadership to evoke change in habits and skills for the entire care team. Energy, time, and motivation are vital ingredients to enable this transformation. The metaphor of Sisyphus is very applicable in describing the challenges associated with this transformation. The only way to overcome this biting challenge is to develop a much disciplined self-governed program that institutes timelines and performance metrics to measure progress.
“It’s not what you a pay a man, but what he costs you that counts.” — Will Rogers
Also, the impact on the cost of deploying such technologies and its cascade effects on the practice and patient fees requires deep appreciation.
It is my hope that by recognizing some of these issues that you, my colleagues, do not become the victims of the Icarus Paradox, a phenomenon described by Danny Miller in his book by the same name. This term refers to the sudden failure of organizations after a short run with apparent success followed by failure, which is brought about by the very elements that initially contributed to the success.
“Do as much as possible for the patient and as little as possible to the patient.” — Dr. Bernard Lown
Fiat justitia et pereat mundus. (Do the right thing, come what may.)
 Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact rcsorthocoach@gmail.com to access information.
Rohit C.L. Sachdeva, BDS, M Dent Sc, is a consultant/coach with Rohit Sachdeva Orthodontic Coaching and Consulting, which helps doctors increase their clinical performance and assess technology for clinical use. He also works with the dental industry in product design and development. He is the co-founder of the Institute of Orthodontic Care Improvement. Dr. Sachdeva is the co-founder and former Chief Clinical Officer at OraMetrix, Inc. He received his dental degree from the University of Nairobi, Kenya, in 1978. He earned his Certificate in Orthodontics and Masters in Dental Science at the University of Connecticut in 1983. Dr. Sachdeva is a Diplomate of the American Board of Orthodontics and is an active member of the American Association of Orthodontics. In the past, he has held faculty positions at the University of Connecticut, Manitoba, and the Baylor College of Dentistry, Texas A&M. Dr. Sachdeva has over 90 patents, is the recipient of the Japanese Society for Promotion of Science Award, and has over 160 papers and abstracts to his credit. Visit Dr. Sachdeva’s blog on https://drsachdeva-conference.blogspot.com. Please contact rcsorthocoach@gmail.com to access information.
- Sachdeva RC. SureSmile technology in a patient-centered orthodontic practice. J Clin Orthod.2001;35(4):245-253.
- Sachdeva RCL. BioDigital Orthodontics: Design and use of suresmile® customized 3D-printed indirect bonding trays: part 20. Orthodontic Practice US. 2016;7(2):20-34.
- Sachdeva RCL, Kubota T. BioDigital Orthodontics: suresmile® aligners, part 21. Orthodontic Practice US. 2016;7(3):26-31.
- Saxe AK, Louie LJ, Mah J. Efficiency and effectiveness of SureSmile. World J Orthod. 2010;11(1):16-22.
- Sachdeva RC, Aranha SL, Egan ME, et al. Treatment time: SureSmile vs conventional. Orthodontics (Chic.). 2012;13(1):72-85.
- Alford TJ, Roberts WE, Hartsfield Jr JK, et al. Clinical outcomes for patients finished with the SureSmile™ method compared with conventional fixed orthodontic therapy. Angle Orthod. 2011;81(3):383-388.
- Rangwala T. Treatment outcome assessment of SureSmile compared to conventional orthodontic treatment using the American board of Orthodontics grading system [thesis]. Bronx, New York: Albert Einstein College of Medicine, Department of Dentistry; 2012.
- Groth C. Compare the quality of occlusal finish between SureSmile and Conventional [thesis] Ann Arbor: University of Michigan; 2012.
- The American Board of Orthodontics Grading System for Dental Casts and Panoramic Radiographs https://www.americanboardortho.com/media/1191/grading-system-casts-radiographs. pdf. Accessed February 3, 2017.
- Larson BE, Vaubel CJ, Grünheid T. Effectiveness of computer-assisted orthodontic treatment technology to achieve predicted outcomes. Angle Orthod. 2013;83:557–562.
- Müller-Hartwich R, Jost-Brinkmann PG, Schubert K. Precision of implementing virtual setups for orthodontic treatment using CAD/CAM-fabricated custom archwires. J Orofac Orthop. 2016;77(1):1-8.
- Smith, TL. Mesio-distal tip and facio-lingual torque outcomes in computer-assisted orthodontic treatment [thesis]. https://indigo.uic.edu/bitstream/handle/10027/9911/Smith_Tharon.pdf?sequence=1. Accessed February 3, 2017.
- Grauer D, Proffit WR. Accuracy in tooth positioning with a fully customized lingual orthodontic appliance. Am J Orthod Dentofacial Orthop. 2011;140(3):433-443.
- Brown MW, Koroluk L, Ching-Chang Ko, Zhang K, Chen M, Nguye T. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am J Orthod Dentofacial Orthop. 2015;148(6):1067–1074.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
