InBrace lingual braces is providing orthodontists with a new and efficient category of orthodontic treatment.
Dr. Hany Youssef discusses a new lingual braces system with increased efficiency and profitability
Introduction
A goal of orthodontic treatment is to achieve excellent treatment outcomes with optimal efficiency. Treatment efficiency may be measured by several different metrics such as chair time, doctor time, and overall treatment time. Often once treatment efficiency metrics are determined, they can then be used to calculate treatment profitability. Many orthodontic practices may then evaluate and use this information to adjust their treatment modalities, mechanics, and/or workflows to optimize their efficiency and profitability.
In the current orthodontic landscape, many orthodontic practices have started moving toward a more digital and proactive treatment workflow using computer-aided design and computer-aided manufacturing (CAD/CAM) technology to improve their clinical predictability and treatment efficiency.1–4 A new CAD/CAM orthodontic treatment modality to penetrate the orthodontic market is the InBrace™ system, which was designed with treatment efficiency in mind.5 This article will explore the different features of InBrace that improve treatment efficiency and will present a hypothetical treatment efficiency and profitability model to compare InBrace with other standard orthodontic treatment modalities.
Programmed Non-Sliding Mechanics (PNM)
The InBrace system is a new category of orthodontic treatment that fundamentally diverges from the traditional edgewise or straight-wire appliances, which use sliding mechanics. While sliding mechanics works efficiently on the labial side with traditional braces, a general consensus is that optimal treatment efficiency has not been achieved with sliding mechanics on the lingual side as it is more difficult and time-consuming because of inaccurate bonding, difficulty with insertion, ligation, adjustment, and disengagement of the archwire, limited visibility, and small interbracket distance.6–12
To resolve some of these inconveniences with early iterations of lingual appliances, CAD/CAM technology was applied to fabricate customized lingual brackets and archwires.13–15 However, this generation of lingual orthodontic treatment still did not resolve the issue of small interbracket distance and introduced a new complication of inefficient bracket replacement, which required a new custom bracket to be ordered, refabricated, and shipped if a replacement bracket was needed. In addition, customizing both the bracket and archwire led to significantly higher lab and hardware costs compared to any other treatment modality, including clear aligners. These higher fees were often passed on to patient fees, which decreased the economical access patients had to this treatment modality. Thus, even with the introduction of CAD/CAM technology, there was minimal adoption of these previous versions of lingual appliances.16
The InBrace system was designed as a behind-the-teeth treatment modality that resolves the inconveniences of all previous versions of lingual appliances. The InBrace system significantly improves treatment efficiency and minimizes clinician intervention by using their proprietary Gentleforce™ technology to apply a new paradigm in orthodontic mechanics that has been termed Programmed Non-Sliding Mechanics (PNM). With PNM, light and continuous forces are generated from a shape memory change that is programmed into nickel-titanium (NiTi) archwires that are capable of simultaneously moving each tooth to their digitally planned position in all 6 degrees of freedom: in/out, up/down, rotation, tip, torque, and even open or closed spaces. This leads to automation in treatment and minimizes the need for clinician intervention. In contrast, sliding mechanics often relies on a more inefficient force mechanism, heavy and interrupted forces in order to overcome unpredictable frictional forces. Heavy and interrupted forces lead to undermining resorption, which is a more inefficient mode of tooth movement compared to the light and continuous forces used in PNM, which results in frontal resorption.17
Designed for efficiency
Another component of PNM that improves treatment efficiency is the InBrace appliance design. The InBrace archwire, termed a Smartwire®, is a programmed, multi-loop, NiTi archwire that is custom designed and digitally produced for each patient using the provider’s approved InBrace Digital Setup. Smartwires are comprised of two types of customized loop systems: Locking Loops and Interproximal Loops (Figure 1).
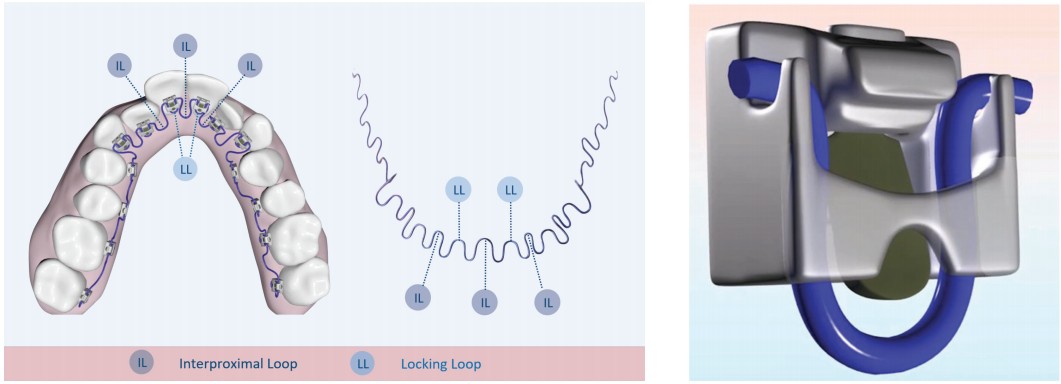
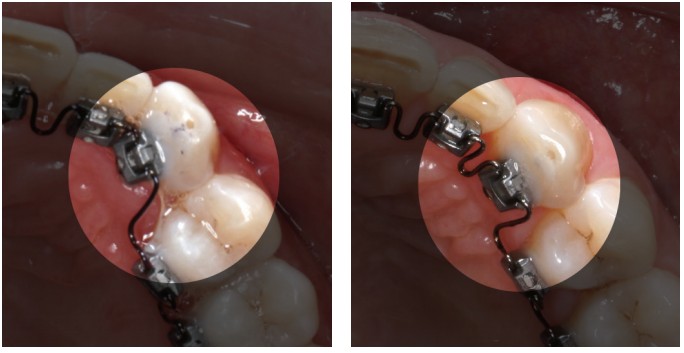
Locking Loops are designed to fit within the InBrace bracket, and it is surrounded by walls on the mesial and distal surfaces, unlike a traditional edgewise bracket with a horizontal slot. Because of the interaction of the Locking Loop with the mesial and distal walls of the bracket, the Locking Loop does not slide when opening or closing spaces resulting in friction-free tooth movement (Figure 2). This non-sliding and friction-free tooth movement potentially improves treatment efficiency by removing the unpredictable force loss due to the variable of friction.18 In addition, Locking Loops create a third-order couple with the InBrace brackets, resulting in torque expression from the beginning of treatment.5
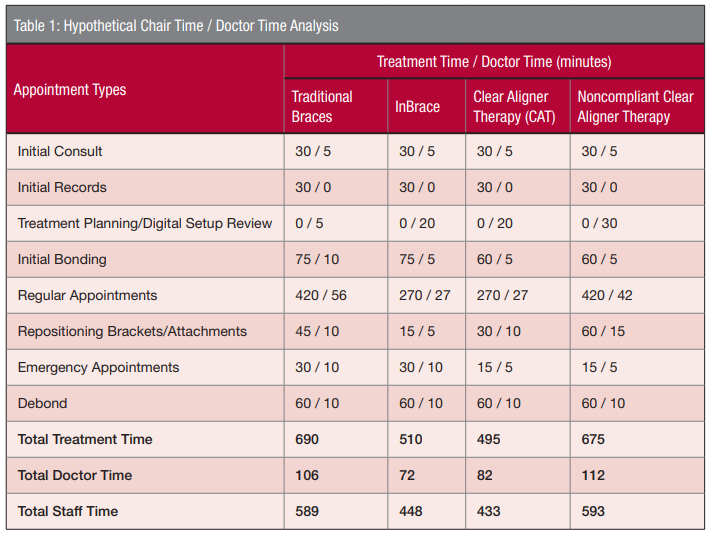
The Interproximal Loops are located in between each tooth, and they effectively increase the length of the Smartwire between brackets by greater than 3 times that of a normal lingual straight-wire appliance. This significantly increases wire flexibility and solves one of the major pain points of traditional lingual appliances: short interbracket distance.8 With the increased wire flexibility, it improves handling during engagement and disengagement of the Locking Loops and brackets. In addition, this increased wire flexibility enables light and continuous forces in all 6 degrees of freedom, including opening and closing spaces, which has the potential to be far more efficient than heavy, interrupted forces that often require more frequent and manual activations (Figure 3). A final benefit of the Interproximal Loops is that they allow patients to floss normally with no interproximal wire obstruction.
In addition to being designed to prevent sliding and enable friction-free tooth movement, the InBrace brackets have several other features that support treatment efficiency. The InBrace bracket is self-ligating and designed with a vertical insertion channel, which improves visualization and handling during the engagement and dis-engagement process leading to swift Smartwire changes. Also, all InBrace brackets are designed with zero prescription since all customization is built into the Smartwires. This allows for immediate and simple bracket replacement when needed, whereas other customized lingual bracket systems require a much more complicated process because the custom bracket would need to be ordered, refabricated, and shipped to an office. The zero-prescription nature of the InBrace brackets also allow them to be designed as low profile as possible which maximizes tongue space and minimizes speech impediments and tissue irritations. Furthermore, the use of zero-prescription brackets significantly reduces the lab cost to a comparable price to clear aligners, which greatly improves the economical access of behind-the-teeth orthodontic treatment to potential patients.
Treatment efficiency and profitability comparison
In recent years, the two major categories of orthodontic treatment that have dominated the current orthodontic market are traditional braces and clear aligner therapy (CAT). The treatment efficiency between these two categories has been compared in several studies with findings that typically show CAT is more efficient but has significantly greater material costs.19–21 These studies also concluded that treatment efficiency and profitability with these two treatment modalities are also dependent on the experience of the orthodontist. Based on these conclusions, a reasonable speculation is that there is not a significant difference in profitability between traditional braces and CAT on average. A significant difference in profitability is likely seen only in orthodontic practices that specialize more heavily in one treatment modality over the other.
With the automation and treatment efficiency built into the InBrace system that has been described thus far, a potential hypothesis is that there is also no significant difference in profitability between InBrace, traditional braces, and CAT on average, and orthodontists who specialize more in InBrace could even see a greater profitability than with the other two treatment modalities. This hypothesis is further supported by the compliance-free nature of InBrace compared to CAT, which will have a mixture of compliant and noncompliant patients that will affect its average efficiency and profitability. To examine and illustrate this hypothesis, hypothetical chair time, doctor time, and profitability analyses were performed.
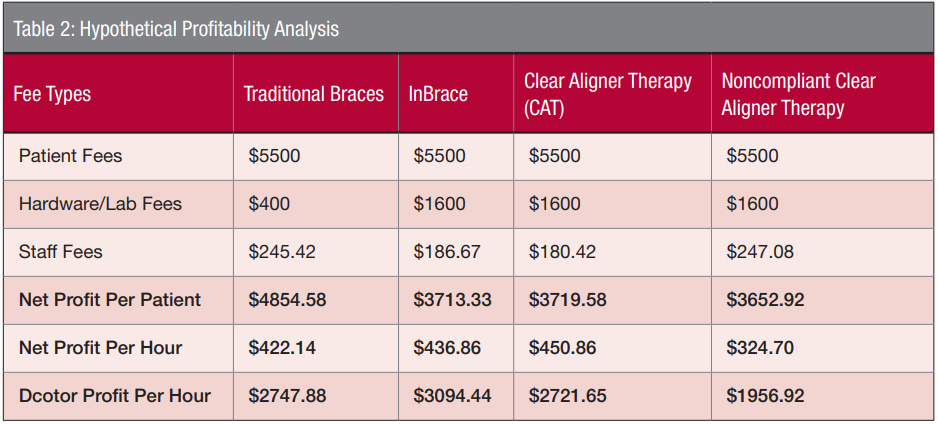
In this hypothetical chair time analysis of the average 18-month orthodontic case, total chair time was modeled for all three treatment modalities (Table 1). Because CAT is highly dependent on compliance, and most orthodontists have experienced a small but significant number of patients who are noncompliant with their clear aligner wear, noncompliant CAT was also modeled. In this model, consistent with previous reports, chair time was significantly higher for traditional braces primarily based on the number of regular appointments modeled for each category (14 for traditional braces and noncompliant CAT and 9 for InBrace and CAT).19–21 All regular appointments for each treatment modality were modeled to take 30 minutes. InBrace and CAT were modeled to have fewer appointments because CAD/CAM orthodontic treatment modalities tend to reduce the number of appointments and allow for longer appointment intervals.1–5,19
Other significant differences in treatment time between the treatment modalities include repositioning brackets/attachments and emergency appointments. Traditional braces often require some bracket repositions since the original bracket position is often manually placed based off of clinical judgment, while CAT typically requires removing and replacing attachments at refinements. In contrast, InBrace, which has digitally positioned brackets transferred by an indirect bonding tray, typically requires minimal repositioning. However, InBrace as a fixed appliance system will likely experience a similar number of emergency appointments as traditional braces, while CAT rarely experiences emergency appointments.15
In this hypothetical analysis of the average 18-month orthodontic case, doctor time was also modeled (Table 1). Similarly, the major difference is found at the regular appointments where on average, 4 minutes per appointment was modeled for traditional braces and 3 minutes per appointment was modeled for InBrace and CAT. Traditional braces were modeled as having more average doctor time per appointment because manual adjustments to the archwires are often needed toward the end of treatment. The other significant difference in doctor time was in the treatment planning/digital setup review. CAT likely requires the most time for this step because additional factors need to be evaluated such as clear aligner staging and attachment design. Based on the calculated doctor time, total staff time can also be calculated by subtracting the total doctor time (minus treatment planning/digital setup review time, which the staff is not involved with) from the calculated total chair time shown in Table 1.
 Based on the hypothetical chair time and doctor time models for the average 18-month orthodontic case, profitability can be calculated for each treatment modality (Table 2). An equal patient fee of $5,500 was modeled for all three treatment modalities, though InBrace and CAT can generally command a higher patient fee in the orthodontic market. An equivalent lab fee was modeled for InBrace and CAT, and the same staff fee per hour ($25/hour) was modeled for all three treatment modalities. With the exception of noncompliant CAT, this model showed that traditional braces, InBrace, and CAT all potentially have a similar net and doctor profit per hour once hardware/lab and staff fees were accounted for. InBrace could potentially see a greater doctor profit per hour because of reduced digital setup review time needed compared to CAT, especially when CAT and noncompliant CAT are averaged together. While this is only a hypothetical model, based on the thoughtful development of PNM and the InBrace appliance design to maximize treatment efficiency, InBrace has the potential to achieve a similar or better profitability than traditional braces and CAT as shown in this hypothetical model.
Based on the hypothetical chair time and doctor time models for the average 18-month orthodontic case, profitability can be calculated for each treatment modality (Table 2). An equal patient fee of $5,500 was modeled for all three treatment modalities, though InBrace and CAT can generally command a higher patient fee in the orthodontic market. An equivalent lab fee was modeled for InBrace and CAT, and the same staff fee per hour ($25/hour) was modeled for all three treatment modalities. With the exception of noncompliant CAT, this model showed that traditional braces, InBrace, and CAT all potentially have a similar net and doctor profit per hour once hardware/lab and staff fees were accounted for. InBrace could potentially see a greater doctor profit per hour because of reduced digital setup review time needed compared to CAT, especially when CAT and noncompliant CAT are averaged together. While this is only a hypothetical model, based on the thoughtful development of PNM and the InBrace appliance design to maximize treatment efficiency, InBrace has the potential to achieve a similar or better profitability than traditional braces and CAT as shown in this hypothetical model.
 Conclusion
Conclusion
 Conclusion
ConclusionPrevious iterations of lingual ortho-dontic treatment likely have not been able to penetrate the orthodontic market due to decreased treatment efficiency and profitability for orthodontists, especially if pricing patient fees at costs similar to traditional braces or CAT.22 As described in this article, InBrace is a fundamentally different category of behind-the-teeth treatment through its use of Gentleforce technology to apply PNM, so its proposed treatment efficiency has the potential to achieve a similar profitability to traditional braces and CAT on average, and orthodontists who specialize more in InBrace could even see a greater profitability than with the other two treatment modalities.
As evidenced by the growing number of starts in the United States, the orthodontic market is not a zero-sum game, and there are countless prospective orthodontic patients that are currently not being captured by traditional braces and CAT. InBrace was developed by orthodontists, for orthodontists, to help expand their patient pools through its new “Smile Now” category of orthodontic treatment that potentially provides orthodontists a behind-the-teeth treatment option with improved efficiency, predictability, and profitability.
From a patient perspective, InBrace serves the needs of countless unserved patients who have previously opted out of orthodontic treatment because they either did not want a visible appliance or did not want the commitment of compliance. Therefore, this “Smile Now” category may bring in a new group of patients into orthodontic offices that were not interested in traditional braces and CAT because it provides these new patients with a more hidden and compliance-free option where they can continue smiling immediately after InBrace bonding without their peers knowing that they are undergoing orthodontic treatment. This expansion of the orthodontic patient pool should not only help grow InBrace patient starts, but also could potentially have a ripple effect to grow traditional braces and CAT patient starts. Overall, the InBrace system has the potential to benefit the orthodontic community and expand the orthodontic patient pool by providing orthodontists with a new and efficient category of orthodontic treatment.
InBrace lingual braces provide another technique to increase efficiency in the orthodontic office. Increasing efficiency in scheduling is important for practice success too. For more insights on improving efficiency, read “Dr. Amy B. Jackson’s “The power of efficiency,” here: https://orthopracticeus.com/the-power-of-efficiency/
 Dr. Hany Youssef is a Board-certified orthodontist. He obtained his Doctor of Dental Surgery from University of Southern California (USC), completed his residency in orthodontics at USC, and is currently a clinical adjunct professor for USC’s graduate orthodontics department. He is in private practice in Tustin, California.
Dr. Hany Youssef is a Board-certified orthodontist. He obtained his Doctor of Dental Surgery from University of Southern California (USC), completed his residency in orthodontics at USC, and is currently a clinical adjunct professor for USC’s graduate orthodontics department. He is in private practice in Tustin, California.
Disclosure: Dr. Youssef is a speaker for InBrace™.
- Brown MW, Koroluk L, Ko C-C, et al. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am J Orthod Dentofac Orthop. 2015;148(6):1067-1074.
- Moreira FC, Vaz LG, Guastaldi AC, English JD, Jacob HB. Potentialities and limitations of computer-aided design and manufacturing technology in the nonextraction treatment of Class I malocclusion. Am J Orthod Dentofac Orthop. 2020;159(1):
- Aldrees AM. Do customized orthodontic appliances and vibration devices provide more efficient treatment than conventional methods? Korean J Orthod. 2016;46(3):180.
- Saxe AK, Louie LJ, Mah J. Efficiency and effectiveness of SureSmile. World J Orthod. 2010;11(1):16-22.
- Tong H, Weissheimer A, Pham J, Lee R, Redmond WR. Lingual Orthodontics Redefined with Automation and Friction-Free Mechanics. J Clin Orthod. 2019;53(4):214-24.
- Gorman JC, Smith RJ. Comparison of treatment effects with labial and lingual fixed appliances. Am J Orthod Dentofac Orthop. 1991;99(3):202-9.
- Gorman JC. Treatment of adults with lingual orthodontic appliances. Dent Clin North Am. 1988;32(3):589-620.
- Moran KI. Relative wire stiffness due to lingual versus labial interbracket distance. Am J Orthod Dentofac Orthop. 1987;92(1):24-32.
- Geron S, Romano R, Brosh T. Vertical forces in labial and lingual orthodontics applied on maxillary incisors–a theoretical approach. Angle Orthod. 2004;74(2):195-201.
- Ye L, Kula KS. Status of lingual orthodontics. World J Orthod. 2006;7(4):361-368.
- Ackerman JL. The challenge of adult orthodontics. J Clin Orthod. 1978;12(1):43-47.
- Creekmore T. Lingual orthodontics–its renaissance. Am J Orthod Dentofac Orthop. 1989;96(2):120-137.
- Wiechmann D, Rummel V, Thalheim A, Simon J. Customized brackets and archwires for lingual orthodontic treatment. Am J Orthod Dentofac Orthop. 2003;124(5):593-599.
- Dalessandri D, Lazzaroni E, Migliorati M, et al. Self-ligating fully customized lingual appliance and chair-time reduction: a typodont study followed by a randomized clinical trial. Eur J Orthod. 2013;35(6):758-765.
- Mujagic M, Fauquet C, Galletti C, et al. Digital design and manufacturing of the Lingualcare bracket system. J Clin Orthod. 2005;39(6):375-382.
- Keim RG, Gottlieb EL, Vogels DS, Vogels PB. 2014 JCO study of orthodontic diagnosis and treatment procedures, Part 1: results and trends. J Clin Orthod. 2014;48(10):607-630.
- Proffit WR Jr, Fields HW, Sarver DM. Contemporary Orthodontics. 4th ed. St. Louis, MO: Mosby Elsevier; 2006.
- AlSubaie M, Talic N, Khawatmi S, Alobeid A, Bourauel C, El-Bialy T. Study of force loss due to friction comparing two ceramic brackets during sliding tooth movement. J Orofac Orthop. 2016;77(5):334-340.
- Buschang PH, Shaw SG, Ross M, Crosby D, Campbell PM. Comparative time efficiency of aligner therapy and conventional edgewise braces. Angle Orthod. 2014;84(3):391-396.
- Zheng M, Liu R, Ni Z, Yu Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod Craniofacial Res. 2017;20(3):127-133.
- Ke Y, Zhu Y, Zhu M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health. 2019;19(1):24.
- Keim RG, Gottlieb EL, Vogels DS, Vogels PB. 2017 JCO Orthodontic Practice Study. J Clin Orthod. 2017;51(10):639-656.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
