Dr. Emad Hussein describes how the TrueEase fixed bite corrector leads to occlusal and skeletal improvement and facial harmony after treatment.
Drs. Emad Hussein, Sari Amer, Khaled Qatawi, and Yazan Ashhab discuss a non-extraction option that overcomes compliance problems
Introduction
International epidemiologic studies suggest that there seems to be over 25% prevalence of Class II malocclusions.1-5 However, the number of patients attending our clinics with Class II malocclusion features appear to be higher than the numbers in the epidemiologic studies.
Class II malocclusion can be due to mandibular deficiency, maxillary excess, or a combination of both. McNamara, et al., found that the mandibular deficiency is more common than maxillary excess.6 Class II malocclusion could be also be due to dentoalveolar reasons — e.g., proclined upper incisors and/or retroclined lower incisors.
In general, there are three treatment modalities to treat the Class II malocclusion:
- First, if the patient is young and still growing, then growth modification in order to restrain the maxilla and to enhance growth of the mandible
- Second, camouflage treatment by mainly retracting the upper segment, advancement of the lower segment, or both.
- Third, orthodontic decompensation and orthognathic surgery in adults, keeping in mind that the treatment modality is dependent on a thorough diagnosis
Growth modification appliances — e.g., removable functional appliances and headgear — require good cooperation from the patients, which in most cases considered an important factor in the success of treatment. The same applies to the use of Class II elastics, where the orthodontist has to time during every visit to convince the patient to wear them. Extractions in the treatment of Class II malocclusion sometimes are more successful after growth ceases, but many patients and their families refuse this treatment option.
In order to keep the non-extraction option and, at the same time, to overcome the problem of compliance, bite correctors (also called fixed functional appliances) were introduced to the orthodontic armamentarium. Bite correctors are fixed orthodontic appliances attached to the upper and lower jaws that keep the lower jaw biting in an advanced position to centric occlusion but still can allow the mandibular condyle to go back to its original position in the glenoid fossa.
The TruEase™ bite corrector appliance design
The True Ease™ bite corrector (Ortho Technology®) is a fixed push-type appliance clamped from both ends and bilaterally to the upper and lower archwires in each jaw (Figures 15-17). Each appliance is made of two parallel cylinders housing nickel-titanium coil springs.
Each cylinder ends with a plunger that is incorporated into it. At the ends of both plungers are hex nuts, which attach the appliance to the archwires. In the upper arch, hex nuts are attached mesial to the upper molars, while in the lower arch, hex nuts are attached distal to the lower canines. Each bite corrector delivers a constant pushing force on each side of approximately 200g, thus resisting the pulling forces of the muscles acting on the mandible.
Treatment protocol using TruEase bite corrector
Fixed bite correctors are usually used after leveling and alignment procedures when reaching heavy stainless steel wire .019″ × .025″ in .022″ brackets and .017″ × .025″ in .018″ brackets (Figures 15-17). The purpose of reaching heavy steel wires before fixing the bite correctors is to overcome the side effects of the pushing forces delivered by the bite correctors, flaring of lower incisors, and lingual tipping of upper incisors.
Each arch should act as a single unit; this is possible by a figure-eight ligature wire from first molar to the contralateral first molar, or a cinch-back distal to each molar or simply by the use of a power chain in order to avoid breakage of the tube during cinching back the heavy steel wires.
Then if the overjet is reasonable, the bite corrector can be attached from each side of the mouth when the mandible is slightly closing edge-to-edge. If the overjet is large, then closing in a Class I molar and canine relationship could be satisfactory.
TruEase bite corrector will show a remarkable correction of the Class II molar and canine relationship after 3 to 4 months of installation, but an additional 3 to 4 months are required to retain this correction and to overcome muscle tendency to pull back the mandible to a posterior location in the glenoid fossa.
It is possible to notice an overcorrection and an edge-to-edge incisor relationship during this period; thus an 8-month period is necessary to induce the change and to retain it. And if overcorrection occurred, it is liable to relapse shortly after removal of the bite corrector to a normal overjet and overbite.
After removal of the bite corrector, the case might require some finishing and detailing. In order to maximize the intercuspation, finishing bends and vertical buccal elastics are mainly used to achieve the solid intercuspation. The solid intercuspation is an important factor in stability of the Class II correction. Due to the upward and backward forces acting on the upper molars, they might become intruded with a vertical distance with lower molars upon closure into maximum intercuspation; in some cases, cutting the archwires mesial to the molars may allow molars to erupt passively and freely until maximum interdigitation is reached.
Retention of cases treated by a fixed functional appliance is by a lower fixed retainer from canine to canine in the lower arch. In the upper arch, retention is by a vacuum clear retainer or a Hawley retainer.
Clinical case
Examination and diagnosis
A 12-year-old growing patient presented with the main complaint of protruded and crooked anterior teeth. She had a brachycephalic type of face with low lower anterior face height and competent lips. When smiling, she showed crowded and procumbent incisors. She presented with a convex soft tissue profile with retrognathic mandible and low lower anterior facial height (Figures 1-3).

Intraorally, she had a good oral hygiene, 1 mm upper midline shifting to the left, and 50% overbite. She showed a Class II molar relationship as well as canine relationship on both sides; overjet was 7 mm (Figures 4-6).

Her upper arch was ovoid and symmetric except in the incisor region where crowding shifted the midline 1 mm to the left side; crowding in the upper arch was around 4 mm. The lower arch was also ovoid and symmetric with 4 mm incisor crowding (Figures 7 and 8).
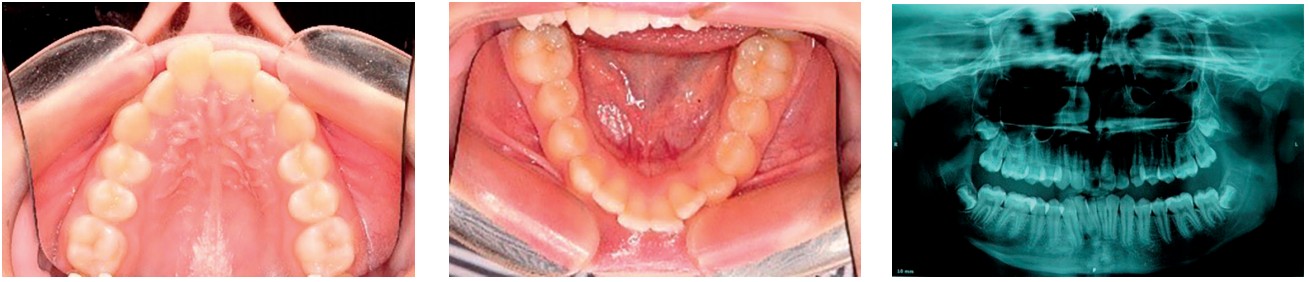
In the orthopantomogram, all third-molar buds are present with lack of space for them to erupt; there were no pathological lesions and no significant root resorption. Her dental age coincided with chronological age (Figure 9).
In the cephalometric analysis, the patient is skeletal Class II based on Wits analysis. All vertical readings indicate horizontal growth and a hypodivergant facial pattern with a decreased lower anterior facial height (Figure 10).
Soft tissue shows normal upper lip with average nasolabial angle, while the lower lip is slightly retrusive.
Dentally, upper incisors were in proclined and protruded position, while the lower incisors were proclined and in an average position (Figure 10).
According to the Cervical Vertebral Maturation (CVM) Method described by Baccetti In 2005,7 the patient was in cervical stage 3, concavities at the lower borders of both C2 and C3 were present, and the body of C3 was trapezoid in shape, which indicated that the peak of mandibular growth would occur during the year after this stage (Figure 11).

Treatment goals
Our main goal of starting treatment at this age for this growing patient was to enhance the growth of the mandible and restrain growth of the maxilla, thus improving facial esthetics. We also aimed to relieve crowding and retract the upper teeth to achieve average overjet and overbite.
Treatment options
The patient was still growing and using a growth modification appliance — e.g., a cervical headgear or a functional appliance was suggested to the patient and her mother, but they refused this option from compliance point of view.
Extractions of two upper first bicuspids was also suggested the patient, but she also refused this option. A fixed functional appliance with bite corrector along with a self-ligating bracket system was our third option for treating this patient with this skeletal and dental malocclusion, and the patient as well as her mother accepted this treatment option.
Treatment progress
A fixed orthodontic appliance of 022 028-inch self-ligating brackets Lotus DS (Ortho Technology) was bonded in the upper and lower arches; .014-inch TruFlex™ copper nickel-titanium wires (Ortho Technology) were used for the leveling and alignment in the upper and lower arches for 6 weeks, followed by 018 copper nickel titanium for another 6 weeks (Figures 12-14).

After using round wires used for alignment, .014 .025-inch copper nickel-titanium wires were used to continue the alignment and start preparation for torque. Six weeks later, .018 .025 copper nickel-titanium wires were used to continue leveling and alignment and torque control and to prepare for steel wires.
Stainless steel .019 .025 inch wires were used in the upper and lower arches after 8 weeks of the use of .018 .025 copper nickel titanium. Four weeks after insertion of the steel wires, a fixed functional appliance, TruEase bite corrector from Ortho Technology, was installed on these heavy steel wires. In the upper arch, the bite corrector was screwed between the first molar and the second premolar; and in the lower arch, it was screwed between the canine and the first premolar (Figures 15-17).

The TruEase bite corrector was used for 10 months until the overjet was zero with reduced overbite to anticipate for relapse after removal. One month before appliance removal, archwires were cut mesial to the upper and lower first molars to allow their settling and better interdigitation.
Treatment results
Treatment resulted in a remarkable improvement in the face due to the continued and enhanced mandibular growth; thus the patient’s convexity has improved. The mentalis muscle strain has decreased due the improvement in the inter jaw relationship. The lower anterior face height was increased, but did not affect facial convexity. Occlusally, the results showed a Class I molar and canine relationship with normal overbite and overjet and good tooth interdigitation (Figures 18-25).



Discussion
Treatment of Class II malocclusion by bite correctors was successful, although most of the correction was a dentoalveolar type and more than a skeletal type. However, if treatment is carried out during the pubertal growth spurt, then the use of a fixed functional appliance can help mandibular growth potential to be expressed fully.8,9
The use of bite correctors will shorten treatment time compared to removable functional appliances, especially due to the fact that bite correctors are installed on the main archwires after leveling and alignment, so we don’t have to wait until the correction of the interarch relationship occurs and then bond the teeth by a fixed orthodontic appliance.10, 11
The forces produced by these bite correctors are similar to the forces produced by the application of a high-pull headgear on the maxilla, leading to intrusion and distalization of the upper molars, and intrusion and proclination of lower anterior teeth.12
The use of heavy archwires is important to overcome proclination of the lower anterior teeth. Torque control of the lower anterior teeth will also help to antagonize these side effects by applying a lingual crown torque in the lower anteriors or using brackets with a negative torque for lower incisors and a positive torque for the upper incisors.9,10
Bite correctors are contraindicated in Class II mandibular deficiency with severely proclined lower incisors, especially those with thin gingival biotype because further proclination is expected with the use of bite correctors despite the use of heavy archwires.
Bite correctors work efficiently in low-to-normal angle cases, but there are no studies about their efficiency in high-angle cases. Probably, the intrusion of upper molars can prevent the increase in vertical dimension during orthodontic treatment, but still treating high-angle cases with bite correctors should be carried out with caution. Still bite correctors are preferred more than Class II elastics because they tend to produce less occlusal plane rotation than Class II elastics. However, patients with a favorable growth pattern and a low mandibular angle will show more treatment success, and better facial changes when treated with bite correctors.9, 13
The use of bite correctors will shorten treatment time compared to removable functional appliances.
Conclusions
TruEase bite correctors managed to correct the Class II malocclusion by a dentoalveolar movement in a non-extraction pattern, and this led to occlusal and skeletal improvement and facial harmony after treatment. The proper interdigitation of the teeth after the use of bite corrector will help in the long-term stability of the results. Keep in mind that stability depends on the severity of the original malocclusion.
After reading about the TruEase fixed bite corrector, check out Dr. Bella Shen Garnett’s technique for fast Class II correction at, “Class II and fast too.” https://orthopracticeus.com/class-ii-and-fast-too/
 Besides his private practice in Ramallah, Professor Emad Hussein has been teaching orthodontics since 2003 at the Arab American University of Palestine until present. He established the department of orthodontics and the residency program of orthodontics at the Arab American University in Palestine where he became a full professor. Dr. Hussein also enrolled in the Palestinian medical council as an examiner in orthodontics from 2006 until September 2019. He also participated in the establishment of a cleft lip and palate society in Palestine. Dr. Hussein published several articles in international orthodontic and dental journals, including The Angle Orthodontist, American Cleft Lip and Palate Journal, World Journal of Orthodontics, Turkish Orthodontic Society Journal, and Saudi Dental Journal. He lectured on several orthodontic topics in the United States, United Kingdom, Cyprus, India, Turkey, Egypt, Dubai, Tunisia, Jordan, and Palestine.
Besides his private practice in Ramallah, Professor Emad Hussein has been teaching orthodontics since 2003 at the Arab American University of Palestine until present. He established the department of orthodontics and the residency program of orthodontics at the Arab American University in Palestine where he became a full professor. Dr. Hussein also enrolled in the Palestinian medical council as an examiner in orthodontics from 2006 until September 2019. He also participated in the establishment of a cleft lip and palate society in Palestine. Dr. Hussein published several articles in international orthodontic and dental journals, including The Angle Orthodontist, American Cleft Lip and Palate Journal, World Journal of Orthodontics, Turkish Orthodontic Society Journal, and Saudi Dental Journal. He lectured on several orthodontic topics in the United States, United Kingdom, Cyprus, India, Turkey, Egypt, Dubai, Tunisia, Jordan, and Palestine.
Sari Amer, Khaled Qatawi, and Yazan Ashhab are residents at the Arab American University in Ramallah.
Disclosure: Dr. Hussein has not received financial remuneration for this article. He is the distributor for this Ortho Technology product in Palestine.
- Horowitz HS, Doyle J. Occlusal relations in children born and reared in an optimally fluoridated community. Angle Orthod. 1970;40(3):104-111.
- Trottman A, Elsbach HG. Comparison of malocclusion in preschool black and white children. Am J Orthod Dentofacial Orthop. 1996;110(1):69-72.
- Lavelle CL. A study of multiracial malocclusions. Community Dent Oral Epidemiol. 1976;4(1):38-41.
- El-Mangoury NH, Mostafa YA. Epidemiologic panorama of malocclusion. Angle Orthod. 1990;60(3):207-214.
- Proffit WR, Fields HW, Sarver DM, Ackerman JL. Contemporary Orthodontics. 5th ed. Mosby Elsevier: St Louis, MO; 2013.
- McNamara Jr, James A. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51(3):177-202.
- Baccetti T, Franchi L, Mcnamara JA Jr The Cervical Vertebral Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Semin Orthod.2005;11:119-129.
- Kragt G, Duterloo HS. The initial effects of orthopedic forces: A study of alterations in the craniofacial complex of a macerated human skull owing to high-pull headgear traction. Am J Orthod Dentofacial Orthop. 1982;81(1):57-64.
- Franchi L, Alvetro L, Giuntini V, et al. Effectiveness of comprehensive fixed appliance treatment used with the Forsus Fatigue Resistant Device in Class II patients. Angle Orthod. 2011;81(4):678-683.
- Chibber A, Upadhyay M, Uribe F, Nanda R. Mechanism of Class II correction in prepubertal and postpubertal patients with Twin Force Bite Corrector. Angle Orthod. 2013;83(4):718-727.
- Chhibber A, Upadhyay M, Uribe F, Nanda R. Long-term stability of Class II correction with the Twin Force Bite Corrector. J Clin Orthod. 2010;44(6):363-376.
- LeCornu M, Cevidanes LH, Zhu H, et al. Three-dimensional treatment outcomes in Class II patients treated with the Herbst appliance: a pilot study. Amer J Orthod Dentofacial Orthop. 2013;144(6):818-830.
- Franchi L, Baccetti T. Prediction of individual mandibular changes induced by functional jaw orthopedics followed by fixed appliances in Class II patients. Angle Orthod. 2006;76(6):950-954.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
