Editor’s intro: Dr. Donald J. Rinchuse shows two patients who benefitted from insights from orthodontic literature. See their progress here.
Dr. Donald J. Rinchuse shows how evidence-based literature helped guide his treatment plan
An 11-year 7-month old female presented for an orthodontic consultation with a Class II malocclusion and all four second bicuspids extracted as well as the mandibular right first molar (Figures 1A-1E). The extraction spaces for these teeth were open and particularly large for the mandibular right second bicuspid/first molar area. The patient’s mother said that a pediatric dentist removed these teeth some time ago, and she did not know the reason (possibly to mitigate crowding and/or tooth decay).

On evaluation of the initial panoramic radiograph (Figure 2), it was observed that the area of the large extraction space of the missing mandibular right second bicuspid/right first molar was very radiolucent, indicating a bony defect. Further, from a clinical examination of this region (as well as a consideration of the panoramic radiographic findings), it was noted that there was little alveolar ridge in this region. The most logical explanation for the bony defect in this area was that on extraction of the mandibular right second bicuspid and right first molar, the buccal and lingual cortical plates were fractured. Parenthetically, the most distal molar in the mandibular right quadrant was by all accounts a third molar.
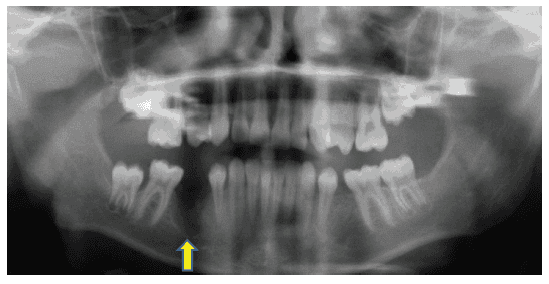
The issue for space closure into the bony defect left from the extractions of the mandibular right second bicuspid and right first molar was whether or not this was possible without jeopardizing the teeth being moved into the defect. That is, would the teeth being moved into the bony defect now be surrounded by defective bone and then be fraught by periodontal and endodontic problems leading to tooth loss? Or, on an optimistic note and based on the literature,1-6 would bringing the so-called good bone of the adjacent teeth into the bony defect augment the bone in this area?
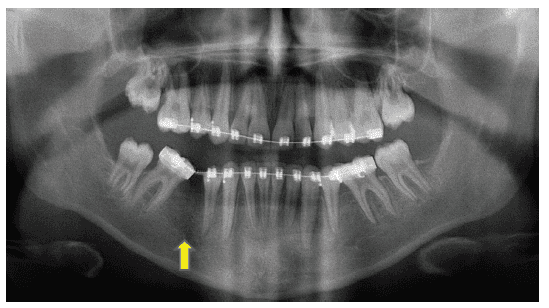
Orthodontic treatment included the use of a .022 inch slot, pre-adjusted, fixed edgewise appliance; light Class II inter-arch elastics; intra-arch power chain elastics; and .016 x .025 inch and .018 x .025 inch stainless steel maxillary and mandibular “working” archwires.
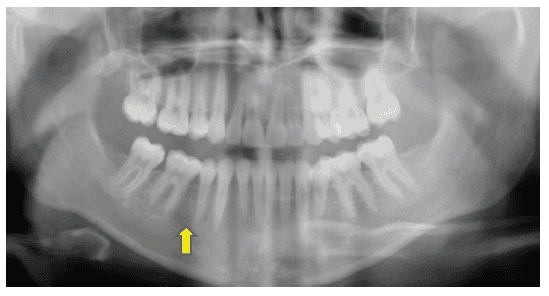
At the end of orthodontic treatment, all the extraction spaces were closed in all four quadrants, including the large one in the mandibular right quadrant. Orthodontic treatment took 23 months and 17 appointments. From an examination of the progress and final panoramic radiographs (Figures 3 and 4), it was evident that orthodontic space closure caused bone augmentation of the mandibular right second bicuspid/first molar region, consistent with reports in the dental literature.1-6 Incidentally, the third molar in the mandibular right quadrant was nicely aligned.
Reading and knowing the dental and orthodontic literature, particularly the evidence-based literature, are clearly an important part of modern-day orthodontic clinical practice and can improve patient care. And as gleaned from this case report, it served to guide the treatment of this patient.
Editor’s call to action
We have orthodontic literature to help your practice grow! Dr. Rinchuse discusses marketing orthodontic practices in “The secret sauce” — more than the golden rule: part 1.
https://orthopracticeus.com/practice-management/secret-sauce-golden-rule-part-1
 Donald J. Rinchuse, DMD, MS, MDS, PhD, is presently in corporate orthodontic practice in Greensburg, Pennsylvania. He has co-authored two books and written over 130 articles.
Donald J. Rinchuse, DMD, MS, MDS, PhD, is presently in corporate orthodontic practice in Greensburg, Pennsylvania. He has co-authored two books and written over 130 articles.
- Goldberg D, Turley PK. Orthodontic space closure of the edentulous maxillary first molar area in adults. Int J Adult Orthodon Orthognath Surg. 1989;4(4):255-266.
- Hom BM, Turley PK. The effect of space closure of the mandibular first molar area in adults. Am J Orthod. 1984;85(6):457-469.
- Lindskog-Stokland B, Wennström JL, Nyman S, Thilander B. Orthodontic tooth movement into edentulous areas with reduced bone height. An experimental study in the dog. Eur J Orthod. 1993;15(2):89-96.
- Wennström JL, Stokland BL, Nyman S, Thilander B. Periodontal tissue response to orthodontic movement of teeth with infrabony pockets. Am J Orthod Dentofacial Orthop. 1993;103(4):313-319.
- Vardimon A, Nemcovsky CE, Dre E. Orthodontic tooth movement enhances bone healing of surgical bony defects in rats. J Periodontol. 2001;72(7):858-864.
- Nemcovsky CE, Beny L, Shanberger S, Feldman-Herman S, Vardimon A. Bone apposition in surgical bony defects following orthodontic movement: a comparative histomorphometric study between root- and periodontal ligament-damaged and peridontally intact rat molars. J Periodontol. 2004;75(7):1013-1019.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
