CEU (Continuing Education Unit): 2 Credits
Educational aims and objectives
This article aims to discuss the efficacy of clear aligner treatment and/or braces in post-COVID-19 treatment plans.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize some history of clear aligner and traditional braces therapies in orthodontics.
- Recognize possible clinical and treatment issues that may arise resulting from the COVID-19 period that may have a lasting effect on orthodontics.
- Realize some characteristics of the biology of tooth movement that will affect patients during COVID-19 treatment.
- Recognize the role that compliance plays in orthodontic treatment.
- Observe some techniques with traditional braces, clear aligner therapy, or a combination of both.

Dr. David Alpan discusses evolving treatment plans in the wake of COVID-19
Abstract
Is clear aligner treatment more effective than braces? What about during a pandemic? Evidence-based research statistically finds that clear aligner treatment facilitates improved oral hygiene compared to braces and creates fewer negative side effects.7,12 Research shows that the gingival health with clear aligner treatment is better in comparison to conventional fixed braces.6,7 With clear aligner therapy, it has been proven to be less painful than braces and overall more comfortable with no food restrictions.3,6,7 Clear aligner treatment is marketed and promoted to the consumer more than braces,4,5 yet braces are still utilized more frequently than clear aligners worldwide. The American Association of Orthodontics (AAO) posted that there are 4.5 million Americans with braces in 2020, and Invisalign® is currently celebrating 8 million cases treated since 1999 worldwide. There are over 30 companies currently manufacturing clear aligners and braces. Why is it that there are so many more braces’ patients than clear aligner patients? There are lots of reasons that we may not be able to explore in this paper. I have found in clinical practice after 23 years that any case types with patients who are compliant, clear aligners are more efficient and effective to use than braces, especially in a COVID-19 world.9
Patients with poor compliance will never achieve an excellent result, no matter the appliance utilized.12 When combining excellent compliance with acceleration and clear aligners, orthodontic treatment is more efficient and effective than braces in many case types, and that is what I will explain in this report. When treating extractions or impacted teeth, a combination of braces and clear aligners is required, as the aligners alone are not efficient with extrusion or changing position of the root apex or torque control5,8,9 — for example, the need for root parallelism post-extraction to help keep the space closed long-term is challenging for clear aligners.9,11,12 Mild-to-moderate crowding, spacing, rotations, surgical orthodontics, and open bite cases treat more efficiently and effectively with clear aligners than braces.18,19 Any severe rotations or tipping will be more effectively treated with braces than clear aligner treatment.8,9,10,11 Braces can deliver a more controlled force application over a longer range of time and, therefore, are more efficient with impacted or severely tipped teeth needing lots of torque.9,10,11,12 Minor rotation control of incisors and molars is equally as effective with clear aligners compared to braces.9,12
Introduction
As an orthodontist, I have a variety of treatment plans utilizing multiple appliances in my armamentarium, but I choose to focus on my list of goals related to the desired treatment outcomes. The list begins based on my initial diagnosis defining all the areas of concern and a treatment plan addressing those concerns.1 The options orthodontists offer to patients can be influenced by many factors: Examples include training, experience level with a certain system, local orthodontic community and dental schools, associations, marketing to the public or the profession, the esthetics of the appliance, the effectiveness, the default or error rate, the negative sequela, etc. The list of influences is as long as the list of orthodontic tools available worldwide to provide orthodontic care.
I choose my appliances based on how well they can achieve my desired goals, and combining modalities or techniques can lead to my ultimate result. A blog on the AAO website states:
“One appliance is not inherently better than another. What is used for an individual’s correction will be based on the goals of treatment and the patient’s lifestyle needs. … The type of appliance used in orthodontic treatment is far less important than the skill in the hands of the person who is providing the treatment. Rely on the skills of the AAO orthodontist, who has the education, experience, and expertise to evaluate diagnostic findings, and translate those into a treatment plan that will help you or your child achieve a healthy and beautiful smile.1”
Djeu G, et al., conclude, “The outcome can only be as good as the orthodontist’s skill in each method. It takes time for a practitioner to develop expertise with any appliance.”2 Therefore, it is safe to say that a skilled orthodontic provider can create just as good of a result with appliance A as another can do with Appliance B.

History
The introduction of clear aligner therapy or a series of tooth positioners dates back to 1944.14 At that time, it was not efficient and did not compare to braces as a reliable tool for many reasons. Comparing the effectiveness of appliances across the world is impossible, as the variables are too numerous and not controllable. Comparing clear aligners to braces in my own practice after 23 years is significant, yet admittedly also anecdotal. I have been in private practice since 1999 and have treated 5,000 patients with braces and 2,500 patients with clear aligners, so my experience is weighted toward braces. It is agreed by peer-reviewed research articles in many journals that clear aligner therapy is shorter in duration than braces.9,11 This may be due to the population of patients treated with clear aligners in those studies, which are typically not as severe, or the goals are not as comprehensive. It could also be that the tooth movements for the cases chosen for the studies eliminated the outliers (difficult tooth movements). Many scientific research articles have found that braces are more effective with rotation of round-shaped teeth and extrusion of anterior teeth.9,12,26 The statistics show that very difficult extreme movements of teeth are better suited with braces.8,9,10
Traditional metal braces started with no prescriptions — zero torque, tip, and angulation programmed into the bracket. Dr. Edward Angle, considered the father of modern orthodontics, used a vertical gold wire with a loop on a band cemented to the tooth to deliver force to create orthodontic tooth movement according to Weinberger.27 Currently, there are hundreds of bracket prescriptions based on preferences, tooth morphology, and various functional or esthetic features. It is common for well-known orthodontists to put their name on the prescription. There is over 100 years of published data on various tools used to control and improve the efficiency of orthodontic tooth movement. As I am an orthodontist focused on excellent outcomes, which set of tools will I be most successful with in the future is a constantly evolving process in private practice orthodontics.
Are braces or clear aligners clinically different when the patient is not able to visit the office as frequently as they had prior to the COVID-19 world? Do I evaluate my outcomes based on the number of visits or how well the teeth finished? Do I compare the effectiveness of my appliance choice based on my most difficult malocclusions and how they finished? Or do I compare the moderate or the easy malocclusions and how they finished? I don’t think there is a right or wrong answer to these questions. The choices begin to be clearer as the list of treatment goals becomes achievable, and the need for efficiency is forced upon us, as is with direct-to-consumer competition or limited access to patients in the COVID-19 world. I started treating my clear aligner patients in 1998 with a mindset that my goals were limited to Class I molar and cuspid cases with 0 mm-3 mm of spacing or crowding. Today I have no limitations with the combination of braces, clear aligners, acceleration, and a compliant patient. As a general reference to understand the difficulty of predictability of tooth movement, see the chart in Figure 1, copied from Weir.14 Currently, there are only a few advantages that require me to use braces, as they are more efficient for root torque and extruding impacted or severely tipped teeth. Modern orthodontics allows me to offer any patient clear aligner therapy in combination with braces, if absolutely necessary, to achieve the desired results. My clinical goals are based on my desired results defined by my treatment plan, not my appliances. The appliance of choice needs to be able to achieve those results predictably and reliably in a wide range of case types.18,19
Biology
The effectiveness of orthodontics is related to the biology of tooth movement and can be influenced in a negative way with patients taking nonsteroidal anti-inflammatory drugs NSAIDs. During 1988 to 2010, multiple researchers found that the application of NSAIDs decreased the rate of tooth movement significantly.15,16,17 Based on this research, all my patients are advised not to take NSAIDs during orthodontic treatment; we only recommend Tylenol® (acetaminophen). Unless the research studies on tooth movement effectiveness tracked if the patients were using NSAIDs to control pain, the results are questionable. I offer vibratory acceleration with pulsatile forces because they offer an analgesic effect,20 which micro-osteo perforations (MOPs) do not. Most patients prefer vibration as a form of acceleration versus MOPs, even though vibration cannot be localized. Accelerated orthodontics with vibration or MOPs has shown a significant result in affecting the treatment outcome and duration.18,19 Incorporating accelerated orthodontics with the use of bone modulation technologies, such as vibration or MOPs, has shown reduction in treatment time and increased treatment predictability.18,19 When comparing clear aligner treatment combined with acceleration, clinical findings show increased predictability with a decrease in treatment time.18,19,20


Results
Braces have a role in very complex situations, and clear aligners can equally be used more than previously understood and accepted. During a pandemic, when our goal is to reduce contact with people, clear aligner treatment is truly more efficient and effective at reducing the number of appointments and reducing overall treatment visits to the office. Clear aligner treatment can be facilitated with virtual initial and progress consults better than braces for the patients and doctors. There is no need for a highly trained assistant, and there are a large number of reduced visits to the office compared to braces.


Compliance
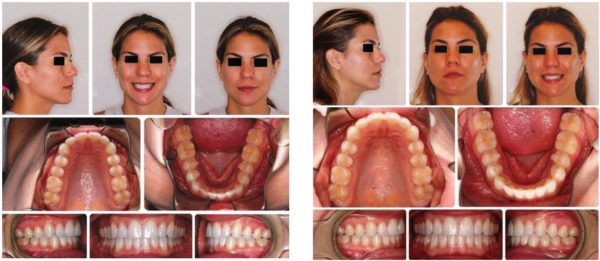
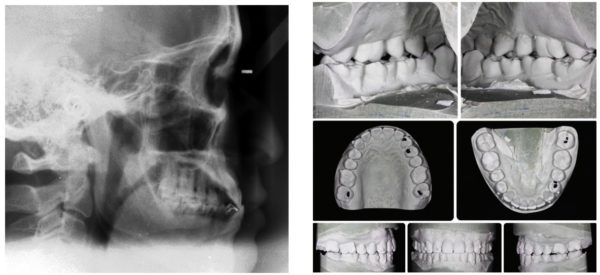
“Compliance is part of any and all orthodontic treatment and contributes a significant part to the success of the treatment outcome. All patients must brush and floss their teeth daily and will need to wear retainers posttreatment.”1 Compliance is a factor that can contribute highly to the outcome independent of the appliance chosen or the complexity of the treatment plan. Many studies have shown increased compliance with clear aligners and a reduction of negative sequela — no effect on speech, no food restrictions, no white spots, less root resorption due to decreased force levels, less pain/discomfort, and reduced treatment time. For example, Figures 2-13 demonstrate treatment with clear aligners combined with vibration. The patient (HA) was in the office for a total of 12 months with 10 office visits, which included exam, diagnosis, treatment plan, records, iTero and i-CAT™ scans, delivery of aligners, one case refinement, occlusal adjustments, incisal edge recontouring, bonded-fixed retainers, and clear vacuum-formed retainers for retention. There was a delay from exam to delivery of 4 weeks and another 4 weeks for the case refinement processing, so she was in active treatment for 10 months. With no emergencies, no negative side effects, the patient was able to resolve all crowding and rotations, and expansion of arches with settled and adjusted occlusion. In our COVID-19 protocol, this treatment would require three virtual visits and five office visits:
Three virtual visits
- Virtual exam
- Virtually evaluate progress and send more aligners
- Virtually progress evaluation CR and send more aligners
Five office visits
- Photos, iTero, i-CAT scan, Dx/Tx Inv submission
- Bonding attachments, IPR, deliver aligners
- Incisal edge recontouring, CR scan, photos
- Occlusal adjustment, impression for retainers
- Deliver retainers



Extraction cases
Extraction cases with braces can take on average 24 to 30 months. Clear aligners alone are not recommended for extraction cases unless the root apex is where we want the finished position to be. Unless fixed appliances are used in conjunction with clear aligners, there is a high probability statistically that the roots will not end up parallel at the end of treatment. If the roots are not parallel, a space will typically open in the retention phase. A combination of sectional braces (cuspid to second molar) with acceleration can accomplish root parallelism and space closure in 6 months. I will then continue with an average aligner treatment of 12 to 18 months to complete all the other goals. My appliance of choice for extraction cases is the combination of braces for leveling and aligning roots and clear aligners to complete the torque, tip angulations, and space closure for compliant patients. Compliance is a huge factor when utilizing clear aligners and patients who are not compliant will be treated with braces only to increase the efficiency and effectiveness.
Surgical orthodontics
Surgical orthodontics is offered for the most severe patients with maxillary and mandibular excess or deficiencies. Orthognathic surgery treatment is considered in orthodontics as one of the most complicated forms of orthodontic treatment. Published results from across the world show orthognathic surgery treatment times on average range between 24 to 30 months and with extractions can be 6 months longer.21,22,23,24 When combining accelerated orthodontics with clear aligner therapy, I can successfully and reliably achieve a total treatment time of 18 to 24 months, including extraction cases.19 Based on my experience with treating orthognathic surgical patients, braces take longer and are not more effective or efficient.18,19 I achieve the same or better results in less time and create a better experience for the patient; therefore, my appliance of choice for all orthognathic cases is clear aligners.
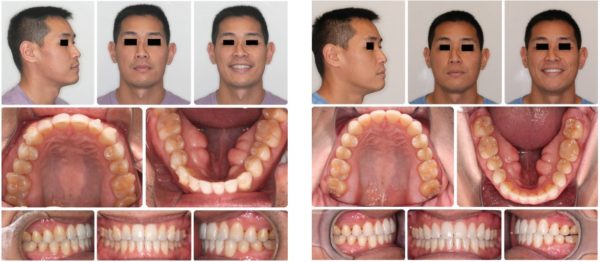
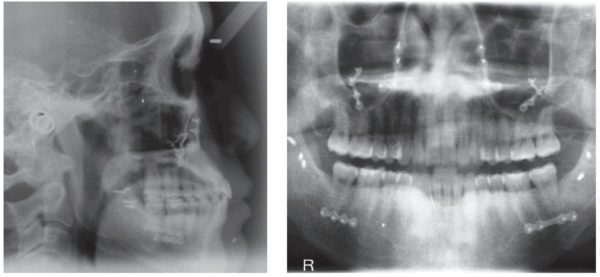
I do not put brackets on the teeth at all, and the surgeon will place one to two TADs per quad and fixate the segments at the time of surgery. Elastics are used from the TADs to initiate function immediately. If I need to extract teeth I will use sectional braces initially to control my root angulations, then followed with clear aligners. Custom digital brackets or aligner systems have shown to be more effective in reducing treatment time for surgical cases due to the coordination of arches digitally.19,21,22 For example, Figures 14-23 show a patient (SK) treated with clear aligner treatment with vibration and orthognathic surgery for a total treatment time of 19 months. A 5-month delay occurred from the date of the exam to delivery of the initial aligners. The patient also waited 2 months for surgery, and each case refinement took about 4 weeks, so he was in active treatment for 10 months and had 11 visits to the office. In our COVID-19 protocol, we can reduce this to three to four virtual appointments and six in-office visits.
Anterior open bite cases
Anterior open bite cases can range from mild, moderate to severe, depending on the amount of vertical growth of the maxilla or protrusion of the dentition. The more severe the open bite, the less it is solely related to the dentition and would require the need for surgical intervention. Mild open bite is defined as a negative 1 mm-3 mm from incisal edge of the maxillary incisors to incisal edge of the mandibular incisors. A moderate open bite can be defined as negative 3 mm-5 mm, and severe is anything greater than negative 5 mm with skeletal discrepancies. The mild-to-moderate open bite cases actually treat out faster and better with clear aligners than with braces according to multiple articles published by Dr. Robert Boyd. Aligners provide a posterior intrusive effect that does not occur with braces, which assists in the bite closure. Aligners prevent extrusion of teeth as braces cause an extrusive effect in general, which is not helpful to close anterior open bites. My appliance of choice for mild and moderate open bite cases is clear aligners with acceleration and no NSAIDs. My appliance of choice for severe skeletal open bite cases is clear aligners, acceleration, and no NSAIDs combined with orthognathic surgery.
Conclusion
In conclusion, based on the literature review and my own clinical experience in practice after 23 years, utilizing clear aligners for compliant patients has led to more efficient9,19,12 and effective treatment outcomes than braces alone. When combining acceleration with compliant clear aligner patients, treatment outcomes are shorter and more effective in achieving the goals than braces in a wide range of case types. In my noncompliant patients, I found that braces are more efficient and effective in achieving the goals independent of the case type. Combining braces and clear aligners with acceleration has facilitated difficult orthodontic tooth movements and allowed me to achieve excellent clinical outcomes in shorter times. Combining acceleration has led to increased predictability and shorter treatment times overall.18,19 Clear aligners offer a more esthetic-oriented treatment process that is more friendly, tolerable, comfortable, and acceptable to the patient. The use of clear aligners is more favorable to the patients’ gingival health before, during, and after orthodontic treatment. The use of clear aligner treatment during a pandemic is far more efficient and effective than braces, as it reduces the number of office visits and emergencies. The reduced health risk by sending more aligners versus doing a braces adjustment in the office is far better for everyone in a COVID-19 world.
Besides discussing the choices between clear aligners or traditional braces, Dr. Alpan has tackled the topic of accelerated orthodontics with orthognatic surgery. Read his CE, take the quiz, and receive 2 CE credits! https://orthopracticeus.com/ce-articles/combining-accelerated-orthodontics-with-orthognathic-surgery-to-reduce-overall-treatment-time/
Author Info
 David Alpan, DDS, MSD, earned his Doctor of Dental Surgery in 1996 and completed his orthodontic specialty certificate from the University of the Pacific (UOP) in 1998 with a Master of Science in Dentistry, as he wrote a thesis on the results of a TMJ research project. Dr. Alpan and Associates has four private practice locations: Los Angeles, Century City, Woodland Hills, and Hawthorne. Dr. Alpan can be contacted at dalpan@aeortho.com or (310) 344-5260.
David Alpan, DDS, MSD, earned his Doctor of Dental Surgery in 1996 and completed his orthodontic specialty certificate from the University of the Pacific (UOP) in 1998 with a Master of Science in Dentistry, as he wrote a thesis on the results of a TMJ research project. Dr. Alpan and Associates has four private practice locations: Los Angeles, Century City, Woodland Hills, and Hawthorne. Dr. Alpan can be contacted at dalpan@aeortho.com or (310) 344-5260.
Dr. Alpan is an active member of ADA, CDA, LADS, PCSO, AAO, CAO, AO, OKU, and TKO. His hobbies are racing cars as a member of Pirelli cup NASA, POC, PCA, CSM, and BMW CCA. He spends his free time with his wife, Mary; son, Zephyr; and daughter, Ambryn.
Disclosures: From 1992 to 1998, Dr. Alpan lectured for Invisalign® at over 250 locations to over 10,000 people. He played an integral part of implementing the Invisalign system into the universities. Dr. Alpan was an Ormco™ insider and helped 3M™ as a research panelist. He is a key opinion leader for AcceleDent® and Propel® and has published several articles on accelerated orthodontics. As a Center of Excellence member for 3M™ Incognito™ and a high-volume Insignia™ provider, Dr. Alpan has incorporated several digital-based systems with custom brackets and wires into his digital workflow.
References
- Braces vs. Clear Aligners [blog]. Association of American Orthodontists (AAO) Member Site. www.aaoinfo.org/blog/braces-vs-clear-aligners. Published January 30, 2019. Accessed August 10, 2020.
- Djeu G, Shelton C, Anthony Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Amer J Orthod Dentofacial Orthop. 2005;128(3):292-298.
- Gao M, Yan X, Zhao R, et al. Comparison of pain perception, anxiety, and impacts on oral health-related quality of life between patients receiving clear aligners and fixed appliances during the initial stage of orthodontic treatment. Eur J Orthod. 2020;1-7.
- Metal Braces vs. Invisalign: Which is Best? Bright Now! Dental website. https://www.brightnow.com/about-us/post/metal-braces-vs-invisalign-which-is-best. Published October 10, 2017. Accessed August 10, 2020.
- Gu J, Tang JS, Skulski B, et al. Evaluation of Invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating index. Amer J Orthod Dentofacial Orthop. 2017;151(2):259-266.
- Buschang PH, Shaw SG, Ross M, Crosby D, Campbell PM. Comparative time efficiency of aligner therapy and conventional edgewise braces. Angle Orthod. 2014;84(3):391-396.
- Azaripour A, Weusmann J, Mahmoodi B, et al. Braces versus Invisalign®: gingival parameters and patients’ satisfaction during treatment: a cross-sectional study. BMC Oral Health. 2015;15:69.
- Zachrisson S, Zachrisson BU. Gingival condition associated with orthodontic treatment. Angle Orthod. 1972;42(1):26-34.
- Papadimitriou A, Mousoulea S, Gkantidis N, Dimitrios K. Clinical effectiveness of Invisalign® orthodontic treatment: a systematic review. Prog Orthod. 2018;19(1):37.
- Gu J, Tang JS, Skulski B, et al. Evaluation of invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the peer assessment rating index. Am J Orthod Dentofacial Orthop. 2017;151(2)259-266.
- Charalampakis O, Iliadi A, Ueno H, Oliver DR, Kim KB. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am J Orthod Dentofacial Orthop. 2018;154(1):47-54.
- Christou T, Abarca R, Christou V, Kau CH. Smile outcome comparison of Invisalign and traditional fixed-appliance treatment: a case-control study. Am J Orthod Dentofacial Orthop. 2020;157(3):357-364.
- Kravitz N, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop.2009;135(1):27-35.
- Weir T. Clear aligners in orthodontic treatment. Australian Dental J. 2017;62:(Suppl 1):58-62.
- Kesling HD. The philosophy of tooth positioning appliance. Am J Orthod. 1945;31(6):297-304.
- Teixeira CC, Khoo E, Tran J, et al. Cytokine expression and accelerated tooth movement. J Dent Res. 2010;89(10):1135-1141.
- Arias OR, Marquez-Orozco MC. Aspirin, acetaminophen, and ibuprofen: their effects on orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006;130(3):364-370.
- Davidovitch Z, Nicolay OF, Ngan PW, Shanfeld JL. Neurotransmitters induces high numbers of cells expressing IFN-gamma at mRNA and protein levels. J Interferon Cytokine Res. 1988;20:7-12.
- Alpan D. Combining accelerated orthodontics with orthognathic surgery to reduce overall treatment time. Orthodontic Practice US. 2018;9(5):39-43.
- Alpan D. A review of accelerated orthodontics. Orthodontic Practice US. 2017;7(5)28-32.
- Lobre WD, Callegari BJ, Gardner G, et al. Pain control in orthodontics using a micropulse vibration device: a randomized clinical trial. Angle Orthod. 2016;86(4)625-630.
- Paunonen J, Helminem M, Peltomaki T. Duration of Orthognathic-Surgical Treatment. Acta Odontol Scand. 2017;75(5):372-375.
- Luther F, Morris DO, Karnezi K. Orthodontic treatment following orthognathic surgery: how long does it take and why? A retrospective study. J Oral Maxillofac Surg.2007;65(10):1969-1976.
- Dowling PA, Espeland L, Krogstad O, Stenvik A, Kelly A. Duration of orthodontic treatment involving orthognathic surgery. Int J Adult Orthodon Orthognath Surg.1999;14(2):146-52.
- Slavnic S, Marcusson A. Duration of orthodontic treatment in conjunction with orthognathic surgery. Swed Dent J.2010;34(3):159-66.
- Rossini G, Parrini S, Castroflorio T, Andrea Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015:85(5):881-889.
- Wienberger W. Dr. Edward Hartley Angle, his influence on orthodontics. Am J Orthod. 1950;36(8):596-607.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
